ABSTRACT
The assessment of response to neoadjuvant systemic therapy (NST) is a critical pillar in defining the multidisciplinary therapeutic strategy in breast cancer. This consensus aimed to establish national guidelines for imaging assessment of NST, based on the best scientific evidence adapted to the Brazilian context. To this end, a panel of experts was formed, composed of breast radiologists, breast surgeons, oncologists, onco-radiotherapists and breast pathologists. The methodology was based on a systematic literature review, followed by face-to-face discussions and rounds of virtual voting (adapted Delphi method), defining consensus when agreement was ≥75%. As a result, radiological response criteria were standardized, and accuracy, false-negative, and positive rates were determined, as well as the role of mammography, ultrasound, magnetic resonance imaging, and tomosynthesis, stratified by molecular subtypes. Additionally, recommendations were established for marking the breast lesion and axillary lymph nodes before the start of treatment. Finally, the role of other imaging techniques, such as contrast-enhanced mammography and positron-emission tomography/computed tomography, was discussed, as well as the impact of artificial intelligence as tools for evaluating the response to SNRT.
Keywords:
breast neoplasm; neoadjuvant systemic therapy; imaging assessment; breast magnetic resonance imaging
INTRODUCTION
Neoadjuvant systemic therapy (NST) has become established as an essential therapeutic strategy in the management of breast cancer. It can reduce the extent of breast and axillary surgery, expanding the possibilities for breast preservation, as well as allowing in vivo evaluation of the tumor response to treatment and providing valuable prognostic information. Accurate evaluation of the response to NST is indispensable for future therapeutic decisions, including the extent of surgical resection and adjuvant treatment. In this scenario, imaging methods play a central role in estimating the extent of residual tumor, in the breast and in the axillary lymph nodes(1). However, heterogeneity in the techniques employed and in the criteria applied for interpretation and classification, as well as in the experience of the professionals involved, can generate significant variations in the results and consequent clinical impact(2). Faced with these challenges, specialized multidisciplinary debate and the development of guidelines are essential to guide imaging assessment in this clinical context. The objective of this article is to report the recommendations of a multidisciplinary panel of experts convened to discuss and establish a consensus on the critical steps related to the use of imaging methods in the evaluation of the response to NST for breast cancer in Brazil. Future directions for the application of artificial intelligence (AI) and the development of new imaging techniques are also discussed.
METHODOLOGY
Composition of the expert panel
A multidisciplinary panel was convened. The panel was composed of 16 specialists with recognized expertise in the fields of breast radiology, breast surgeons, clinical oncology, radiotherapy, and breast pathology.
Search of the literature
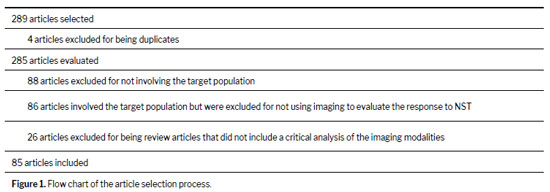
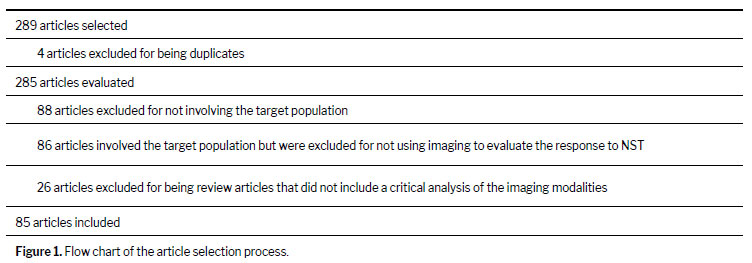
To support the discussions, a systematic search of the literature was conducted in the databases Medline (via PubMed) and Latin-American and Caribbean Health Sciences Literature (via the Brazilian Regional Library of Medicine), using descriptors and National Library of Medicine Medical Subject Headings related to the theme (neoadjuvant chemotherapy, diagnostic imaging, and breast neoplasms). Studies, including clinical trials, systematic reviews/meta-analyses, randomized clinical trials, and review articles, were considered eligible if they were published between July 2014 and July 2024, in Portuguese or English. Studies were selected if they addressed the imaging evaluation of the response to NST for breast cancer using methods such as mammography, ultrasound, magnetic resonance imaging (MRI), tomosynthesis, contrast-enhanced mammography (CEM), and positron-emission tomography/computed tomography (PET/CT). After those search criteria had been applied, 289 references were identified. Two reviewers, working independently, selected the studies using Rayyan software (Qatar Computing Research Institute, Doha, Qatar). In cases of disagreement, the final decision was made by a third reviewer. Articles that did not address the target population or the scope of the panel were excluded, as were articles of low quality or low methodological rigor. Of the 289 articles initially selected, 204 were thus excluded. Therefore, the final sample comprised 85 articles selected to support the development of the panel recommendations (Figure 1).
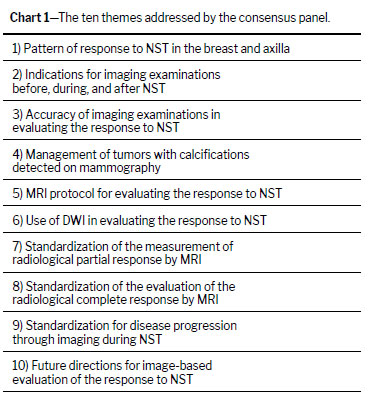
The panel defined 10 themes to be addressed during the in-person meeting, covering the radiological aspects of the response to NST in breast cancer (Chart 1). For each theme, questions were formulated to be answered and put to a vote. Each specialist had 40 days to propose a preliminary text for each question based on the best available scientific evidence.
Consensus meetingAn in-person consensus meeting took place during the 18th Gramado Breast Cancer Event, in the city of Gramado, located in the Brazilian state of Rio Grande do Sul, and was open to the public. Each panelist was given 7–10 min to present the evidence relevant to their clinical question. Next, an open vote was held for each question with the following response options: “agree”, “disagree”, and “abstain”. Consensus was considered to have been reached when ≥ 75% of the panelists agreed with the statement(s) presented. If that proportion was not achieved, the question was submitted to new rounds of discussion, reformulation, and voting, carried out in person (on the day of the meeting), virtually (later), or both, until consensus was reached on all questions proposed by the group.
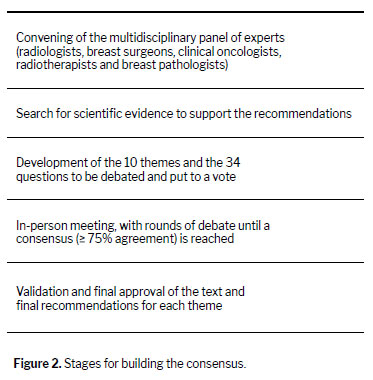
Validation and final approval of the recommendationsAfter consensus was reached, the text was drafted in a preliminary format and submitted for critical analysis and approval by the panel members. The final recommendations were then classified into one of five categories: category A—strong recommendation in favor, based on high-quality evidence; category B—strong recommendation in favor, based on moderate-quality evidence; category C—weak recommendation in favor, based on low-quality evidence; category D—recommendation in favor, based solely on an expert consensus; and category E—recommendation against, with insufficient evidence to support its use. The phases of the process are summarized in Figure 2.
RESULTSThe ten themes proposed for discussion by the panel are listed in Chart 1. For each theme, three to five questions were formulated; a total of 36 questions were put to a vote. Among those 36 questions, consensus was achieved in the first in-person vote for 25 (69.4%), in the first round of virtual voting for two (5.5%), in the second round of virtual voting for three (8.3%), in the third round of virtual voting for three (8.3%), and in the final round of virtual voting for three (8.3%). The answers to the questions are described below, together with the results of the voting by the expert panel. Ultimately, 10 recommendations were issued for the imaging-based evaluation of the response to NST.
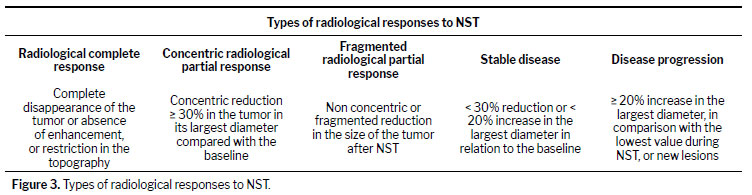
THEME 1: PATTERN OF RESPONSE TO NST IN THE BREAST AND AXILLAWhat types of radiological responses can be identified in the breasts?The types of responses observed in breast imaging examinations are categorized as follows (Figure 3): a radiological complete response—defined as complete disappearance of the tumor (in morphology-based examinations, such as mammography, tomosynthesis, and ultrasound) or the absence of enhancement or restriction in the topography of the tumor (in functional examinations, such as MRI, PET/CT, and CEM); a concentric radiological partial response—defined as a concentric reduction ≥ 30% in the size of the tumor in its largest diameter compared with the initial examination; a fragmented radiological partial response—defined as not concentric or fragmented reduction in the size of the tumor after NST; stable disease—defined as a < 30% reduction or a < 20% increase in the largest diameter of the tumor in relation to the initial examination; and disease progression—defined as a ≥ 20% increase in the largest diameter of the lesion, in comparison with the lowest value recorded since the beginning of therapy, or as the appearance of new lesions. These response patterns affect the accuracy of imaging examinations in identifying residual tumor, with the fragmented response pattern having the lowest agreement with the pathology
(3,4).
Panel results: 88% agreement; 0% disagreement; 12% abstention.How can axillary lymph nodes be evaluated and described to allow pretreatment determination of the tumor burden?The ultrasound assessment should be performed with the patient in the supine position, with one hand behind the head. The scan is initiated from the axillary tail of the breast toward level I of the axilla, proceeding to levels II and III
(5). Given that ultrasound assessment plays a role in therapeutic decision-making
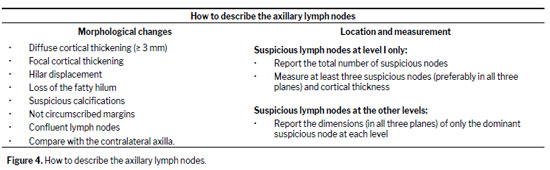
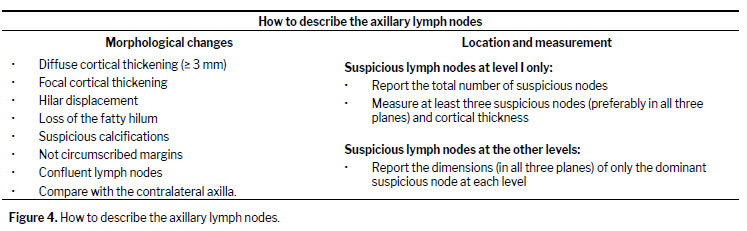
(6,7), it is extremely important to report the type of morphological alteration observed, as well as the respective level at which the involvement is located (Figure 4). The following morphological signs are suggestive of metastatic involvement: diffuse cortical thickening (≥ 3 mm); focal cortical thickening; hilar displacement; loss of the fatty hilum; calcifications with suspicious morphology; ill-defined margins; confluent lymph nodes. It is important to compare with the contralateral axilla, mainly to evaluate the initial signs of involvement. When there are suspicious lymph nodes only at axillary level I, it is recommended that the total number of suspicious lymph nodes be reported, that the size of at least three such lymph nodes be measured (preferably in all three orthogonal planes), and that any cortical thickening be described. If there are suspicious lymph nodes at the other levels (levels II and III), the recommendation is to describe only the dominant suspicious lymph node at each level, measuring its size in all three planes. Doppler evaluation is optional and can be useful to assist in performing the biopsy by identifying the axillary vessels or large-caliber vessels adjacent to the lymph node.
The Response Evaluation Criteria in Solid Tumors (RECIST) method was developed to standardize the evaluation of the response of solid tumors to cancer treatment, being widely used in clinical research and, in some cases, clinical practice. It was published in 2000 and updated (to version 1.1) in 2009. It provides guidance on how to measure and classify target lesions, through imaging examinations, as well as on how to determine whether those lesions have regressed, remained stable, or progressed after treatment. The RECIST method is rarely used or recommended in patients with breast cancer receiving NST, because it presents significant limitations for practical application. Although some of the parameters established in the RECIST method were used for the development of this consensus, its use in isolation for response evaluation is not recommended. Therefore, we recommend instead using the largest tumor diameter, comparing it with that obtained in the initial examination, as a parameter for evaluating the response to NST, as well as volume and diffusion as optional parameters.
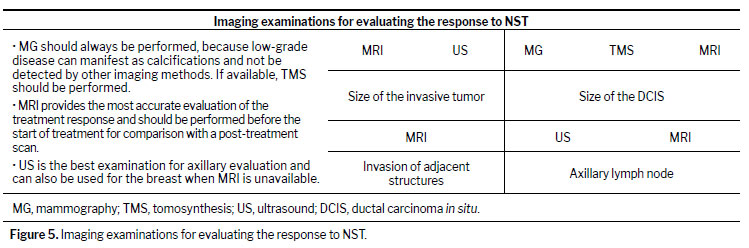
Panel results: 88% agreement; 0% disagreement; 12% abstention.THEME 2: INDICATIONS FOR IMAGING EXAMINATIONS BEFORE, DURING, AND AFTER NSTWhich examinations are important in the imaging evaluation of the response to NST?In the evaluation of the response to NST, mammography should always be performed, because low-grade disease can manifest as calcifications and not be detected by other methods, such as MRI. If available, tomosynthesis should be performed, especially in women under 50 years of age with dense breasts and tumors that present with architectural distortion or asymmetry. The examination that provides the most information about the disease is MRI, which, if available, should be performed prior to the start of treatment and again, for comparison, during or at the end of treatment. The best imaging method for axillary evaluation is ultrasound, which can be used in order to evaluate a breast neoplasm when MRI is not available (Figure 5).
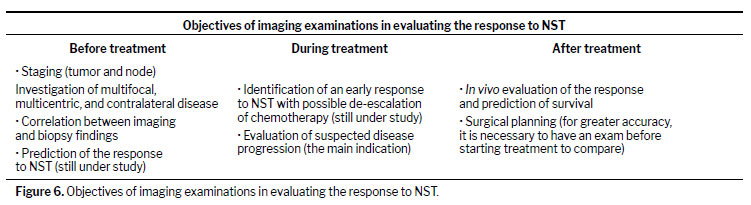
Panel results: 97% agreement; 3% disagreement; 0% abstention.When and for what purposes should these examinations be performed?The objectives of and indications for imaging methods in NST vary according to the stage of treatment (Figure 6). The objectives before the start of treatment are as follows: to identify and assess the extent of disease in the breast and axilla, including the size of the index lesion and the presence of multifocal/multicentric disease or disease in the contralateral breast; to establish a basis for future comparisons; to correlate imaging aspects with biopsy results in order to exclude cases of diagnostic underestimation or sampling error before the start of treatment; and to identify radiological findings that are predictive of a treatment response (this use is an area of intense research). The following are the objectives during treatment: to identify an early tumor response to NST with possible de-escalation of chemotherapy (this use has been extensively studied but the evidence is still under construction); and to investigate the suspicion of disease progression (in practice, this is the main indication during treatment, and the examination should be chosen according to the clinical presentation and initial tumor presentation). At the end of treatment, the main objective is to identify and assess the extent of residual disease in the breast and axilla, for surgical planning
(8).
Panel results: 88% agreement; 3% disagreement; 9% abstention.When is breast lesion marking essential, and what materials should be used?Invasive breast cancer marking should be performed regardless of molecular subtype, preferably before the start of treatment or after the first cycle of treatment, with a metallic clip or radioactive device (radioactive seed), which can be visualized with different imaging methods after the end of NST, or with a charcoal solution, if the team is familiar with that method (which requires visualization by a surgeon during surgery, with no possibility of preoperative marking by the radiologist after the end of NST). In patients with a solitary lesion, the marker should be inserted in the center of the lesion. If there are multiple lesions (multifocal, multicentric, or both), those that influence the surgical planning should be marked. Bilateral lesions should always be marked
(9).
Panel results: 90% agreement; 0% disagreement; 10% abstention.When is axillary lymph node marking essential, and what material should be used?Despite advances in imaging, no imaging examination reliably rules out axillary involvement (any node status), with surgical biopsy being the gold standard for determining axillary response. However, the concept of axillary tumor burden determined by imaging methods is replacing the concept of lymph node involvement in the initial staging of breast cancer (low tumor burden generally being defined as fewer than two suspicious lymph nodes on imaging). This concept of residual axillary tumor burden has not yet been widely validated for use in evaluating the axillary response after NST. The aim of marking the affected lymph node before the start or after the first cycle of NST (with a clip, radioactive device, or charcoal) is to prepare for targeted axillary dissection, which reduces the false-negative rate of axillary stagin
(10). Nevertheless, its implementation and technique are under debate and should follow the protocols of the respective institution.
Panel results: 90% agreement; 0% disagreement; 10% abstention.THEME 3: ACCURACY OF IMAGING EXAMINATIONS IN EVALUATING THE RESPONSE TO NSTDoes the accuracy of imaging examinations vary according to tumor subtype?Imaging examinations play a key role in evaluating the response to NST, assisting in surgical planning and avoiding overtreatment. Accuracy can vary depending on the imaging method and the molecular subtype of the tumor, being lower for luminal tumors and higher for triple-negative tumors, as well as for those with HER2 overexpression
(11).
Panel results: 100% agreement; 0% disagreement; 0% abstention.How accurate is mammography in evaluating the response to NST?In mammography, lesion measurement shows a weak correlation with pathology, with an average coefficient of agreement of 0.55
(11). For the identification of a pathological complete response (pCR), mammography has been reported to have a sensitivity of 65%, a specificity of 81%, a positive predictive value (PPV) of 52%, a negative predictive value (NPV) of 88%, and a rate of agreement with the pathological evaluation of 40%
(12).
Panel results: 100% agreement; 0% disagreement; 0% abstention.How accurate is ultrasound in evaluating the response to NST?Ultrasound is an effective technique when there is residual tumor with a diameter ≥ 0.7 cm. However, its reported accuracy in predicting a response to treatment is only 59.6–80.0%, being limited when the lesion is a ductal carcinoma
in situ, for which it has a sensitivity of 60–80%, a specificity of 70–85%, a PPV of 65–75%, and an NPV of 65–75%
(13).
Panel results: 88% agreement; 12% disagreement; 0% abstention.How accurate is MRI in evaluating the response to NST?In comparison with mammography and ultrasound, MRI has the best accuracy, being the modality recommended as the gold standard for evaluating the response to NST
(14). It has a sensitivity of approximately 90%, a specificity of 60–100%, a PPV of 65–85%, and an NPV of 85–90%. The accuracy of MRI is higher for HER2-positive tumors, and triple-negative tumors, whereas it is lower for luminal subtypes A and B
(15). It has also shown better accuracy in predicting a pCR for tumors with a high proliferative index.
Panel results: 82% agreement; 0% disagreement; 18% abstention.THEME 4: MANAGEMENT OF TUMORS WITH CALCIFICATIONS DETECTED ON MAMMOGRAPHYWhat types of responses to NST can calcifications exhibit?The type of tumor regression and treatment-induced changes affect the accuracy of imaging methods in identifying and determining the extent of residual disease after NST. Although the ability of mammography to detect calcifications is an advantage in breast cancer screening, it can become a disadvantage after treatment. Calcifications can increase, decrease, or remain stable after NST
(16): in most cases (50–83%), they remain stable; in 12–18% of cases, they decrease, disappearing completely in only 4%; and they increase in 8–29% of cases.
Panel results: 100% agreement; 0% disagreement; 0% abstention.What does the persistence of calcifications after the end of NST represent?Calcifications may represent residual tumor (invasive or ductal carcinoma
in situ), tumor necrosis, or other, treatment-related changes. From their morphology, extent, or evolution on mammography, it is not possible to establish whether they represent residual tumor or benign changes. Studies have shown that 50.4–61.5% of post-treatment calcifications at the tumor site represent residual tumor, and a number of studies have reported a poor correlation between their extent on mammography and the dimensions of the tumor in the surgical specimen
(12,17).
Panel results: 100% agreement; 0% disagreement; 0% abstention.How should we manage residual calcifications seen on mammography that do not show enhancement on MRI?A negative result on MRI does not have sufficient accuracy to establish the absence of residual tumor in the clinical scenario of calcifications identified on mammography
(18,19). Thompson et al.
(18) found that residual tumor was present in 76% of women with post-NST calcifications on mammography and a radiological complete response (absence of any type of enhancement) on MRI. Therefore, complete excision of post-NST calcifications in the tumor bed is recommended, regardless of their mammographic appearance, even if there is complete nodule regression and absence of enhancement on MRI
(19). This ensures the resection of any residual tumor and facilitates future surveillance. However, it represents a limitation to post-NST surgical de-escalation, potentially resulting in unnecessary mastectomies in many women.
Panel results: 100% agreement; 0% disagreement; 0% abstention.THEME 5: MRI PROTOCOL FOR EVALUATING THE RESPONSE TO NSTShould the full MRI protocol always be used, or can the abbreviated version be applied?The full MRI protocol is the most suitable for evaluating the response to NST, given that there are no robust data in the literature to support the use of an abbreviated protocol
(20). The relevant studies have been retrospective, with small samples and without standardized protocols, which can mainly result in underestimation of residual tumor requiring surgical re-intervention
(20,21).
Panel results: 100% agreement; 0% disagreement; 0% abstention.At what stage should MRI be performed and for what purposes?It is recommended that MRI be performed before the start of NST (as a baseline examination) to assess the extent of the disease and the presence of multifocal, multicentric, or bilateral lesions. During treatment, a follow-up MRI may be performed after completion of the first or second cycle to evaluate the response to treatment, given the possibility of altering the treatment regimen when it is not effective, although this is still under study and currently without clinical application. After the end of treatment, MRI assists in surgical planning, especially when conservative techniques are employed, precluding the need for a more extensive surgical procedure and reducing the need for reoperation due to residual disease or positive margins.
Panel results: 82% agreement; 0% disagreement; 18% abstention.When is it necessary to proceed with a biopsy in the presence of a new suspicious finding on MRI prior to treatment?Suspicious lesions, with an appearance different from the index lesion (suspected of being other tumor subtypes), and those that might modify the treatment plan should be biopsied prior to the start of the proposed treatment regimen.
Panel results: 100% agreement; 0% disagreement; 0% abstention.What should be done if an MRI finding is probably benign before the start of treatment?Category 3 of the Breast Imaging Reporting and Data System (BI-RADS) is applied to findings considered “probably benign,” with a less than 2% chance of malignancy. Although BI-RADS category 3 findings are well-defined and have been validated for mammography and ultrasound, there are still limited data for MRI
(22). Although the use of category 3 as a criterion is discouraged in the context of imaging evaluation of a known neoplasm, lesions of that character are often found, and their management is challenging. Because the patient is already scheduled for treatment and has a high risk of malignancy, some professionals choose to confirm these lesions by biopsy, especially if the lesions in question are near the index lesion. However, several studies have demonstrated a low (0.8–1.4%) risk of malignancy for patients with BI-RADS 3 lesions
(23,24), which could justify imaging follow-up. Therefore, the best course of action should be individualized and discussed in a multidisciplinary context, taking into account the type of lesion, the risk group, and the treatment proposed.
Panel results: 94% agreement; 0% disagreement; 6% abstention.THEME 6: USE OF DIFFUSION-WEIGHTED IMAGING IN EVALUATING THE RESPONSE TO NSTWhat are the parameters for a good diffusion-weighted imaging sequence?Diffusion-weighted imaging (DWI) can be used in order to assess the response to NST. These sequences do not require the use of contrast and allow quantitative assessment through calculation of the apparent diffusion coefficient (ADC). The necessary equipment, parameters, and cutoff point that allow good differentiation between benign and malignant lesions on DWI have been well established in the recommendations of the European Society of Breast Imaging
(25–27), covering several aspects: a ≥ 1.5 T scanner; a dedicated coil with at least 4 channels; axial acquisitions including both breasts; acquisition preferably before contrast administration; an echo-planar imaging spectral attenuated inversion recovery sequence with fat saturation; minimum resolution of 2 × 2 mm; slice thickness ≤ 4 mm; the use of two b values (0–50 s/mm
2 and 800 s/mm
2); and an acquisition time of 2–5 min. However, the low resolution and long acquisition time are factors that still limit the use of DWI at many institutions.
Panel results: 75% agreement; 0% disagreement; 25% abstention.What values are used in order to determine the response to NST?Several studies and meta-analyses have sought to establish ADC cutoff values to differentiate patients who have achieved a pCR, as well as to predict, at the beginning of treatment, those with a higher probability of achieving a pCR
(27) . However, there is considerable heterogeneity among the published works, in relation to the population studied, the type of treatment used, the DWI acquisition technique, and the post-processing of the images. This variability makes it difficult to define universally applicable ADC cutoff values. However, tumors with lower ADC values before the start of therapy tend to show a better response to treatment and a greater chance of achieving a pCR. In addition, an increase in ADC over the course of treatment generally reflects a tumor response. In the absence of exact cutoff values, experts recommend that, for early response assessment (after the first or second cycle of treatment), the criterion of a > 25% increase in the ADC values over the baseline values should be used in order to identify patients who have achieved a good response
(28,29). For the end-of-treatment analysis, a documented increase in the ADC values (> 40% over baseline) suggests a radiological complete response, as do ADC values similar to or above those observed for normal breast tissue
(30). Conversely, the persistence of low ADC values, close to those observed before treatment, suggests residual tumor.
Panel results: 75% agreement; 0% disagreement; 25% abstention.How accurate is DWI in evaluating the response to NST?In the assessment of the early response to NST (after the first or second cycle of treatment), a > 25% increase in the ADC has been shown to have a sensitivity of 83%, a specificity of 76–84%, and an accuracy of 84% for identifying a pCR
(28,29), whereas an ADC increase > 40% has been shown to have a sensitivity of 100%, a specificity of 91%, and an accuracy of 96% for identifying a pCR at the end of treatment
(30). A recent meta-analysis of 21 articles demonstrated that, for identifying a pCR,/ the use of DWI has a sensitivity of 89% (range, 86–91%) and a specificity of 72% (range, 68–75%) in patients undergoing NST
(31).
Panel results: 75% agreement; 0% disagreement; 25% abstention.THEME 7: STANDARDIZATION OF THE MEASUREMENT OF A RADIOLOGICAL PARTIAL RESPONSE BY MRIWhat are the methods for quantifying a partial response, depending on the type of lesion?The method for quantifying a partial response depends on the observed pattern of response to NST. The measurement is most reproducible in cases of a concentric partial response, in which there is a pattern of retraction or shrinkage, with the best correlation being between the size of the lesion on imaging and the pathology result. In this measurement, the entire lesion should be included in all three planes with multiplanar reconstruction (anteroposterior, latero-lateral, and craniocaudal axes) and key images (in at least the two orthogonal planes containing the three major axes) should be obtained for documentation. In the case of a concentric partial response in a lesion containing areas of necrosis, the cystic portions without enhancement should be included in the measurement of the lesion in the three major planes. In the case of a fragmentation response pattern, the total extent of the lesion in all three planes should be measured (to allow surgical planning), as should the largest residual focus, which can be used for staging the lesion, according to the tumor–node–metastasis classification (TNM)
(32,33).
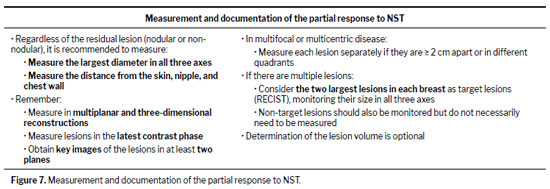
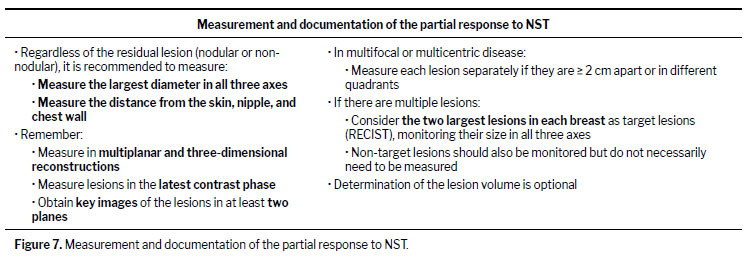
Panel results: 94% agreement; 0% disagreement; 6% abstention.How to quantify a partial response in single, multifocal, multicentric, and bilateral lesionsRegardless of the type of residual lesion (nodular or non-nodular), when the lesion is solitary, measure the largest diameter in all three axes, as well as the distance from the skin, nipple, and chest wall. Use multiplanar and three-dimensional reconstructions for this measurement, as well as the latest contrast phase (or the phase with the greatest tumor enhancement). Obtain key images of the largest axis in each plane, and document the size in at least two orthogonal planes. In the case of lesions that are multifocal or multicentric, measure each lesion separately, especially if there is a ≥ 2 cm distance between them or if they are in different quadrants. When there are multiple lesions, consider the two largest in each breast as the target lesions (as recommended in the RECIST), monitoring the measurements in all three axes. The remaining lesions (i.e., the non-target lesions) should also be monitored but do not necessarily need to be measured. The determination of lesion volume is optional but can be useful in some cases (Figure 7).
The causes of divergence between imaging measurements and pathology include the presence of ductal carcinoma
in situ, an adjacent inflammatory process, the presence of necrosis, non-nodular lesions, residual microscopic foci, anti-angiogenic therapy, and late tumor enhancement
(32,33). The correlation is stronger for tumors with an initial diameter ≤ 5 cm, high-grade carcinomas, and hormone receptor-negative tumors.
Panel results: 94% agreement; 0% disagreement; 6% abstention.How do benign lesions behave over the course of the treatment?Benign lesions can undergo changes during neoadjuvant chemotherapy, because chemotherapeutic drugs affect vascularization and reduce circulating hormone levels
(33,34). The possible effects on benign lesions include the following: none (stability); a reduction in size; a reduction in enhancement, reflecting decreased blood supply or cellular activity; and resolution, especially if the lesions are hormone-sensitive or inflammatory nature.
Panel results: 94% agreement; 0% disagreement; 6% abstention.THEME 8: STANDARDIZATION OF THE EVALUATION OF THE RADIOLOGICAL COMPLETE RESPONSE BY MRIWhat is the definition of a radiological complete response and the most accurate parameters to identify it: absence of enhancement or enhancement smaller than parenchyma?It is recommended to adopt the absence of enhancement in the later phases of a dynamic MRI study as a criterion for a radiological complete response. This criterion is the most widely used in the literature because it has been well studied, has been widely validated, and is easy to implement. In the presence of minimal residual enhancement, the calculation of the signal enhancement ratio (SER) can be useful, given that the parameters with the highest specificity (90.4%) for a pCR are a SER ≤ 1.6 and enhancement extending ≤ 0.2 cm
(35–37).
Panel results: 82% agreement; 6% disagreement; 12% abstention.How should we proceed in cases of lesions in which high signal intensity persists on T2-weighted imaging but there is no enhancement?Tumors that become necrotic, hemorrhagic, or fibrotic after NST can show high signal intensity on T2-weighted imaging. However, that finding should not necessarily be interpreted as residual lesion, especially if there is no accompanying enhancement
(35–37).
Panel results: 88% agreement; 0% disagreement; 12% abstention.What are the causes of false positives and false negatives in determining a radiological complete response?The causes of false positives in determining a radiological complete response include fibrosis and post-treatment inflammatory changes, which can present as enhancement in the tumor bed. False negatives are mainly related to non-nodular enhancement-type tumors and the antiangiogenic action of chemotherapeutic agents such as taxanes and anthracyclines, which reduce blood flow and vascular permeability
(33,35–37).
Panel results: 88% agreement; 6% disagreement; 6% abstention.How to evaluate signs of a radiological complete response in the axilla by MRI?The response to NST in the axilla has been described as a return to the usual appearance of the lymph nodes; that is, symmetrical (in relation to the contralateral axilla), with a thin cortex and a preserved fatty hilum, and showing homogeneous contrast enhancement
(35–37).
Panel results: 82% agreement; 0% disagreement; 18% abstention.How accurate are image-guided biopsy methods for confirming a pCR?Image-guided minimally invasive biopsies have shown promise in identifying a pCR. Although there is no standardization in the literature, it is recommended, on the basis of the best results obtained, that sampling be done by vacuum-assisted biopsy with 7–10 gauge needles, collecting 6–12 representative fragments from the tumor bed, with clip retrieval, in patients who meet the criteria for a radiological complete response or minimal residual disease on MRI
(37,38).
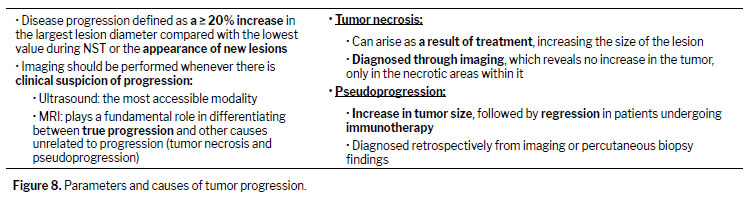
Panel results: 88% agreement; 0% disagreement; 6% abstention.THEME 9: STANDARDIZATION OF SCREENING FOR DISEASE PROGRESSION THROUGH IMAGING DURING NSTWhat should be the definition of tumor progression and the parameters used in order to identify it?Disease progression is the least common type of response to NST. It is characterized by a ≥ 20% increase in the largest lesion diameter in comparison with the lowest value recorded since the start of therapy or the appearance of new lesions. Early recognition of progression can modify treatment and avoid unnecessary toxicities. Whenever there is clinical suspicion of progression, imaging studies should be ordered. Ultrasound can be an accessible alternative when it can clearly confirm disease progression. However, in many cases MRI plays a fundamental role in differentiating between true progression and other causes of a clinically relevant increase in the size of lesion that are unrelated to growth of the tumor itself, such as tumor necrosis
(39), as described in Figure 8.
Panel results: 94% agreement; 0% disagreement; 6% abstention.Does the average time to a response after the start of therapy vary according to the molecular subtype?Triple-negative molecular subtype and tumors with HER2 overexpression that show an early response (after the first cycle of treatment) have a higher probability of achieving a pCR at the end of treatment. Changes in the enhancement curve and diffusion precede changes in dimensions. Conversely, receptor-positive (luminal) tumors undergoing NST have a later response and a lower chance of achieving a pCR
(39).
Panel results: 94% agreement; 0% disagreement; 6% abstention.What are the factors that can mimic disease progression during NST?During NST, tumor necrosis and pseudoprogression can mimic progression of breast cancer (Figure 8). Tumor necrosis can arise as a result of treatment, causing an increase in the clinical dimensions of the lesion. The diagnosis is made through imaging examinations, which can confirm that the increase in size is not due an increase in the tumor but rather to expansion of the necrotic areas within it that lead to an overall increase in the lesion size. Pseudoprogression is defined as an increase in tumor size or the appearance of a new lesion followed by regression in patients undergoing immunotherapy. It is diagnosed by using retrospective imaging data. Histopathology shows infiltration of multiple immune cells, rather than tumor cells. Biopsy is a relatively simple procedure that can be used in order to differentiate between true progression and pseudoprogression
(40–42).
Panel results: 94% agreement; % disagreement; 6% abstention.THEME 10: FUTURE DIRECTIONS FOR IMAGE-BASED EVALUATION OF THE RESPONSE TO NSTHow will the introduction of AI change mammography and ultrasound examinations?The use of AI in combination with imaging methods for predicting the response to NST has been extensively studied in the literature. There have been small, heterogeneous studies using mammography, some of which have employed AI to evaluate changes in breast density as a means of predicting the response to treatment, with interesting preliminary result
(43). Combining ultrasound with AI algorithms makes it possible to evaluate the biophysical properties of breast tissue and produce satisfactory results in predicting treatment respons
(44). Another great potential of AI in ultrasound is the possibility of predicting axillary lymph node metastasis.
Panel results: 88% agreement; 0% disagreement; 12% abstention.How will the introduction of AI change MRI examinations?The most accurate method for predicting the treatment response is MRI. Currently, qualitative (morphology and enhancement) data are being combined with multiparametric MRI data
(4), as well as radiomics, deep learning, and machine learning data, making this analysis predominantly quantitative, with improved accuracy
(45,46). The use of AI in combination with the experience of the radiologist and the technological advances in imaging methods has great potential for optimizing the prediction of the response to NST.
Panel results: 88% agreement; 0% disagreement; 12% abstention.What is the impact of new imaging methods being studied, such as CEM?The sensitivity of CEM in predicting the treatment response is similar to that of MRI. Therefore, CEM represents an acceptable alternative when MRI is contraindicated or unavailable
(47).
Panel results: 88% agreement; 0% disagreement; 12% abstention.Can PET/CT play a role in evaluating the response to NST?For predicting the response to NST, PET/CT has greater specificity than does MRI, whereas MRI has greater sensitivity. New radiopharmaceuticals and the combination with radiomics has the potential to improve the performance of PET/CT
(9). Although still in the research phase, dedicated breast PET and PET/MRI provide better image quality and functional parameters
(2,48), which makes them promising new modalities.
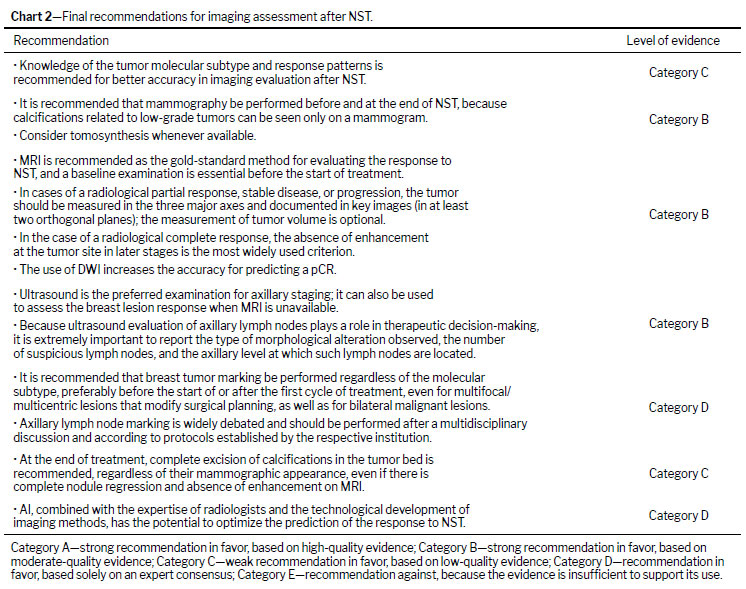
Panel results: 88% agreement; 0% disagreement; 12% abstention .CONCLUSIONThis consensus presents a comprehensive overview of the image-based evaluation of the response to NST, addressing response patterns, examination techniques, measurement methodologies, and documentation of the results, as well as discussing future directions for the application of AI and the development of new imaging techniques (Chart 2). It serves as a practical guide, not only for radiologists but also for all professionals on multidisciplinary teams involved in the care of breast cancer patients, and is consistent with similar documents published in other countries
(49,50). However, we recognize that in some regions of Brazil, especially within the setting of the Unified Health Care System, there may be restrictions on access to more complex examinations or procedures, such as MRI or prior marking for NST, which can limit the full applicability of these recommendations at facilities with less infrastructure or of lesser complexity. In such situations, it is essential that each institution follow the established protocols, considering local availability. Finally, we emphasize that this document will be reviewed periodically, with updates planned every three years, thus ensuring the incorporation of new evidence and technologies.
AcknowledgmentsWe give special thanks to Drs. Antônio Frasson, Carlos Barrios, and Felipe Zerwes, great researchers and visionaries, who enabled and encouraged the creation of this important consensus document during the 18th Gramado Breast Cancer Event.
REFERENCES1. Álvarez-Benito M. Imaging evaluation of neoadjuvant breast cancer treatment: where do we stand? Eur Radiol. 2024;34(10):6271-6272.
2. Caracciolo M, Castello A, Urso L, et al. Comparison of MRI vs. 18FDG PET/CT for Treatment Response Evaluation of Primary Breast Cancer after Neoadjuvant Chemotherapy: Literature Review and Future Perspectives. J Clin Med. 2023;12(16):5355.
3. Kim TH, Kang DK, Yim H, et al. Magnetic resonance imaging patterns of tumor regression after neoadjuvant chemotherapy in breast cancer patients: correlation with pathological response grading system based on tumor cellularity. J Comput Assist Tomogr. 2012;36(2):200–206.
4. Cheng Q, Huang J, Liang J, el al. The diagnostic performance of DCE-MRI in evaluating the pathological response to neoadjuvant chemotherapy in breast cancer: a meta-analysis. Front Oncol. 2020;10:93.
5. Di Paola V, Mazzotta G, Pignatelli V, et al. Beyond N Staging in Breast Cancer: Importance of MRI and Ultrasound-based Imaging. Cancers. 2022;14:4270.
6. Jung JG, Ahn SH, Lee S, Kim EK, et al. No Axillary Surgical Treatment for Lymph Node-Negative Patients after Ultra-Sonography: Protocol of a Prospective Randomized Clinical Trial. BMC Cancer. 2022;22:189.
7. Gentilini OD, Botteri E, Sangalli C, Galimberti V, et al. Sentinel Lymph Node Biopsy vs. No Axillary Surgery in Patients with Small Breast Cancer and Negative Results on Ultrasonography of Axillary Lymph Nodes: The SOUND Randomized Clinical Trial. JAMA Oncol. 2023;9:1557–1564.
8. Fowler AM, Mankoff DA, Joe BN. Imaging Neoadjuvant Therapy Response in Breast Cancer. Radiology. 2017 Nov;285(2):358-375.
9. Oh JL, Nguyen G, Whitman GJ, et al. Placement of radiopaque clips for tumor localization in patients undergoing neoadjuvant chemotherapy and breast conservation therapy. Cancer. 2007;110(11):2420-7.
10. Donker M, Straver ME, Wesseling J, et al. Marking axillary lymph nodes with radioactive iodine seeds for axillary staging after neoadjuvant systemic treatment in breast cancer patients: the MARI procedure. Ann Surg. 2015;261(2):378-82.
11. Conti M, Morciano F, Bufi E, et al. Surgical Planning after Neoadjuvant Treatment in Breast Cancer: A Multimodality Imaging-Based Approach Focused on MRI. Cancers (Basel). 2023; 15(5):1439.
12. An YY, Kim SH, Kang BJ. Residual microcalcifications after neoadjuvant chemotherapy for locally advanced breast cancer: comparison of the accuracies of mammography and MRI in predicting pathological residual tumor. World J Surg Oncol. 2017 Nov 6;15(1):198.
13. Adrada BE, Candelaria R, Moulder S, et al. Early ultrasound evaluation identifies excellent responders to neoadjuvant systemic therapy among patients with triple-negative breast cancer. Cancer. 2021;127(16):2880–7.
14. Reis J, Thomas O, Lahooti M, et al. Correlation between MRI morphological response patterns and histopathological tumor regression after neoadjuvant endocrine therapy in locally advanced breast cancer: a randomized phase II trial. Breast Cancer Res Treat. Breast Cancer Res Treat. 2021;189(3):711-723.
15. Samiei S, De Mooij CM, Lobbes MBI, et al. Diagnostic Performance of Noninvasive Imaging for Assessment of Axillary Response After Neoadjuvant Systemic Therapy in Clinically Node-positive Breast Cancer: A Systematic Review and Meta-analysis. Ann Surg. 2021 Apr 1;273(4):694-700.
16. Portnow LH, Kochkodan-Self JM, Maduram A, et al. Multimodality Imaging Review of HER2-positive Breast Cancer and Response to Neoadjuvant Chemotherapy. Radiographics. 2023;43(2):e220103.
17. Azam R, Lim D, Curpen B, et al. Correlation of Mammographic Microcalcifications with Final Surgical Pathology After Neoadjuvant Chemotherapy for Breast Cancer. Ann Surg Oncol. 2023;30(7):4123-4131.
18. Thompson BM, Chala LF, Shimizu C, et al. Pre-treatment MRI tumor features and post-treatment mammographic findings: may they contribute to refining the prediction of pathologic complete response in post-neoadjuvant breast cancer patients with radiologic complete response on MRI?. Eur Radiol. 2022;32(3):1663-1675.
19. Feliciano Y, Mamtani A, Morrow M, et al. Do Calcifications Seen on Mammography After Neoadjuvant Chemotherapy for Breast Cancer Always Need to Be Excised?. Ann Surg Oncol. 2017;24(6):1492-1498.
20. Yirgin I. K, Engin G, Yildiz S, et al. Abbreviated and Standard Breast MRI in Neoadjuvant Chemotherapy Response Evaluation: A Comparative Study. Current Medical Imaging, 2022, 18, 1052-1060.
21. Tang W, Chen S, Hu W, et al. Abbreviated Versus Full-Protocol MRI for Breast Cancer Neoadjuvant Chemotherapy Response Assessment: Diagnostic Performance by General and Breast Radiologists. AJR. 2023;220(6):817-825.
22. Fazeli S, Stepenosky J, Guirguis MS, et al. Understanding BI-RADS Category 3. Radiographics. 2025;45(1):e240169.
23. Lee SE, Lee JH, Han K, et al. BI-RADS category 3, 4, and 5 lesions identified at preoperative breast MRI in patients with breast cancer: implications for management. Eur Radiol. 2020 May;30(5):2773-2781.
24. Gweon HM, Cho N, Kim SY, et al. Management for BI-RADS category 3 lesions detected in preoperative breast MR imaging of breast cancer patients. Eur Radiol. 2017 Aug;27(8):3211-3216.
25. Baltzer P, Mann RM, Lima M, et al. EUSOBI international Breast Diffusion-Weighted Imaging working group. Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur Radiol. 2020 Mar;30(3):1436-1450.
26. Gullo RL, Partridge SC, Shin HJ, et al. Update on DWI for Breast Cancer Diagnosis and Treatment Monitoring. AJR Am J Roentgenol. 2024 Jan;222(1):e2329933.
27. van der Hoogt KJJ, Schipper RJ, Winter-Warnars GA, et al. Factors affecting the value of diffusion-weighted imaging for identifying breast cancer patients with pathological complete response on neoadjuvant systemic therapy: a systematic review. Insights Imaging. 2021;12(1):187.
28. Hottat NA, Badr DA, Lecomte S, et al. Value of diffusion-weighted MRI in predicting early response to neoadjuvant chemotherapy of breast cancer: comparison between ROI-ADC and whole-lesion-ADC measurements. Eur Radiol. 2022 Jun;32(6):4067-4078.
29. Pereira NP, Curi C, Osório CABT, et al. Diffusion-Weighted Magnetic Resonance Imaging of Patients with Breast Cancer Following Neoadjuvant Chemotherapy Provides Early Prediction of Pathological Response - A Prospective Study. Sci Rep. 2019;9(1):16372.
30. Shin HJ, Baek HM, Ahn JH, et al. Prediction of pathologic response to neoadjuvant chemotherapy in patients with breast cancer using diffusion-weighted imaging and MRS. NMR Biomed. 2012;25(12):1349-59.
31. Gao W, Guo N, Dong T. Diffusion-weighted imaging in monitoring the pathological response to neoadjuvant chemotherapy in patients with breast cancer: a meta-analysis. World J Surg Oncol. 2018;16(1):145.
32. Expert Panel on Breast Imaging: Slanetz PJ, Moy L, Baron P, et al. ACR Appropriateness Criteria® Monitoring Response to Neoadjuvant Systemic Therapy for Breast Cancer. J Am Coll Radiol. 2017;14(11S):S462-S475.
33. Reig B, Lewin AA, Du L, et al. Breast MRI for Evaluation of Response to Neoadjuvant Therapy. Radiographics. 2021;41(3):665-679.
34. Leddy R, Irshad A, Hewett L, et al. Effects of Neoadjuvant Chemotherapy on Benign Breast Lesions Compared to Cancers: Should an Additional Lesion on Magnetic Resonance Imaging Responding Similar to Cancer after Neoadjuvant Chemotherapy be Viewed with Suspicion? J Clin Imaging Sci. 2016;6:39.
35. Gu YL, Pan SM, Ren J, et al. Role of Magnetic Resonance Imaging in Detection of Pathologic Complete Remission in Breast Cancer Patients Treated With Neoadjuvant Chemotherapy: A Meta-analysis. Clin Breast Cancer. 2017 Jul;17(4):245-255.
36. Kim SY, Cho N, Shin SU, Lee HB, Han W, Park IA, Kwon BR, Kim SY, Lee SH, Chang JM, Moon WK. Contrast-enhanced MRI after neoadjuvant chemotherapy of breast cancer: lesion-to-background parenchymal signal enhancement ratio for discriminating pathological complete response from minimal residual tumour. Eur Radiol. 2018;28(7):2986-2995.
37. Heil J, Kuerer HM, Pfob A, et al. Eliminating the breast cancer surgery paradigm after neoadjuvant systemic therapy: current evidence and future challenges. Ann Oncol. 2020 Jan;31(1):61-71.
38. Heil J, Sinn P, Richter H, et al. RESPONDER - diagnosis of pathological complete response by vacuum-assisted biopsy after neoadjuvant chemotherapy in breast Cancer - a multicenter, confirmative, one-armed, intra- individually-controlled, open, diagnostic trial. BMC Cancer. 2018;18(1):851.
39. Panzeri MM, Losio C, Della Corte A, et al. Prediction of chemoresistance in women undergoing neo-adjuvant chemotherapy for locally advanced breast cancer: volumetric analysis of first-order textural features extracted from multiparametric MRI. Contrast Media Mol Imaging. 2018;2018:8329041.
40. Jha CK, Verma H, Sinha U, Singh PK. Acute inflammatory response to multiple chemotherapy regimen in breast carcinoma: An unreported entity1. Breast Dis. 2022;41(1):391-395.
41. Park HJ, Kim KW, Pyo J, et al. Incidence of Pseudoprogression during Immune Checkpoint Inhibitor Therapy for Solid Tumors: A Systematic Review and Meta-Analysis. Radiology. 2020;297(1):87-96.
42. Sheikhbahaei S, Marcus CV, Sadaghiani MS, et al. Imaging of Cancer Immunotherapy: Response Assessment Methods, Atypical Response Patterns, and Immune-Related Adverse Events, From the AJR Special Series on Imaging of Inflammation. AJR Am J Roentgenol. 2022;218(6):940-952.
43. Skarping I, Larsson M, Förnvik D. Analysis of mammograms using artificial intelligence to predict response to neoadjuvant chemotherapy in breast cancer patients: proof of concept. Eur Radiol. 2022;32(5):3131-3141
44. Bahl M, Chang JM, Mullen LA, et al. Artificial Intelligence for Breast Ultrasound: AJR Expert Panel Narrative Review. AJR Am J Roentgenol. 2024 Dec;223(6):e2330645.
45. Li W, Partridge SC, Newitt DC, et al. Breast Multiparametric MRI for Prediction of Neoadjuvant Chemotherapy Response in Breast Cancer: The BMMR2 Challenge. Radiol Imaging Cancer. 2024;6(1):e230033
46. Pesapane F, Agazzi GM, Rotili A, et al. Prediction of the Pathological Response to Neoadjuvant Chemotherapy in Breast Cancer Patients With MRI-Radiomics: A Systematic Review and Meta-analysis. Curr Probl Cancer. 2022;46(5):100883.
47. Bernardi D, Vatteroni G, Acquaviva A, et al. Contrast-Enhanced Mammography Versus MRI in the Evaluation of Neoadjuvant Therapy Response in Patients With Breast Cancer: A Prospective Study. AJR Am J Roentgenol. 2022;219(6):884-894.
48. Fowler AM, Strigel RM. Clinical advances in PET-MRI for breast cancer. Lancet Oncol. 2022;23(1):e32-e43.
49. Expert Panel on Breast Imaging; Hayward JH, Linden OE, Lewin AA, et al. ACR Appropriateness Criteria® Monitoring Response to Neoadjuvant Systemic Therapy for Breast Cancer: 2022 Update. J Am Coll Radiol. 2023;20(5S):S125-S145
50. Schiavone A, Ventimiglia F, Zarba Meli E, et al. Third national surgical consensus conference of the Italian Association of Breast Surgeons (ANISC) on management after neoadjuvant chemotherapy: The difficulty in reaching a consensus. Eur J Surg Oncol. 2024;50(7):108351
1. Clínica de Diagnóstico Avançado por Imagem (DAPI), Curitiba, PR, Brazil
2. Grupo Fleury Medicina e Saúde, São Paulo, SP, Brazil
3. Instituto Orizonti de Longevidade e Saúde, Belo Horizonte, MG, Brazil
4. Lucilo Maranhão Diagnósticos, Recife, PE, Brazil
5. A.C.Camargo Câncer Center, São Paulo, SP, Brazil
6. Grupo Dasa, São Paulo, SP, Brazil
7. Hospital São Vicente de Paulo, Rio de Janeiro, RJ, Brazil
8. Beneficência Portuguesa de São Paulo, São Paulo, SP, Brazil
9. Hospital Israelita Albert Einstein, São Paulo, SP, Brazil
10. Hospital Mãe de Deus, Porto Alegre, RS, Brazi
11. Hospital Nora Teixeira, Porto Alegre, RS, Brazil
12. University of Iowa Hospitals and Clinics, Iowa City, IA, USA
13. Redimama-Redimasto, Belo Horizonte, MG, Brazil
14. Universidade Estadual Paulista, UNESP, Botucatu, SP, Brazil
15. Hospital de Câncer Araújo Jorge, Goiana, GO, Brazil
16. Cebrom Oncoclínicas, Goiana, GO, Brasil
17. Instituto de Mastologia e Oncologia, Goiana, GO, Brazil
18. Grupo Oncoclínicas, Salvador, BA, Brazil
19. Faculdade de Medicina da Universidade de São Paulo (FMUSP), São Paulo, SP, Brazil
a.
https://orcid.org/0000-0003-2017-9776b.
https://orcid.org/0000-0002-8469-4681c.
https://orcid.org/0000-0001-7040-6549d.
https://orcid.org/0000-0001-9085-2204e.
https://orcid.org/0000-0003-0192-9885f.
https://orcid.org/0009-0007-9134-6064g.
https://orcid.org/0009-0002-6578-1808h.
https://orcid.org/0000-0002-4836-8053i.
https://orcid.org/0000-0002-4054-8236j.
https://orcid.org/0000-0003-1682-113Xk.
https://orcid.org/0000-0002-4295-1002l.
https://orcid.org/0000-0002-3789-4461m.
https://orcid.org/0000-0002-8330-0222n.
https://orcid.org/0000-0002-9445-8674o.
https://orcid.org/0000-0009-4702-2002p.
https://orcid.org/0000-0002-5838-3636Correspondence:Linei Augusta Brolini Delle Urban
Clínica de Diagnóstico Avançado por Imagem (DAPI),
Rua Ângelo Domingos Durigan, 1240, Casa 01, Curitiba, PR, Brasil, 82020-452.
Email:
lineiurban@hotmail.comEditor in charge: Dr. Valdair Francisco Muglia.
Received in
October 6 2025.
Accepted em
December 15 2025.
Publish in
July 3 2026.

 |
|



 PDF English
PDF English
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket