ABSTRACT
This study presents a systematic review of the role of imaging in the diagnosis of central nervous system toxoplasmosis, in addition to a case series from a tertiary university hospital. The review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines and registered in the International Prospective Register of Systematic Reviews (ID: CRD420251107718). Studies published after January 1, 2000 were retrieved from the PubMed, Embase, Scopus, and Latin-American and Caribbean Health Sciences Literature databases. Two authors, working independently, selected studies that met the eligibility criteria, which were organized with Rayyan software. Imaging findings were described using computed tomography (CT), conventional magnetic resonance imaging (MRI), advanced MRI sequences or nuclear imaging, focusing on single-photon-emission computed tomography, with and without thallium-201, and positron-emission tomography/CT. Extracted data focused on lesion topography, signal characteristics, enhancement, restricted diffusion, and when available, spectroscopy and perfusion MRI findings. To illustrate typical and atypical imaging features, a complementary case series was included, evaluating patients with confirmed cerebral toxoplasmosis. The review demonstrates that CT and MRI remain essential for diagnosis and follow-up, whereas advanced MRI sequences provide additional value in differentiating toxoplasmosis from other opportunistic infections and neoplastic processes.
Keywords:
Toxoplasma; Toxoplasmosis, cerebral/diagnosis; Toxoplasmosis/diagnostic imaging; Neuroimaging.
RESUMO
Este estudo apresenta uma revisão sistemática do papel da imagem no diagnóstico da toxoplasmose do sistema nervoso central, além de uma série de casos de um hospital universitário terciário. A revisão foi conduzida de acordo com as diretrizes Preferred Reporting Items for Systematic reviews and Meta-Analyses e registrada prospectivamente no International Prospective Register of Systematic Reviews (ID: CRD420251107718). Estudos publicados após 1º de janeiro de 2000 foram recuperados do PubMed, Embase, Scopus e Literatura Latino-Americana e do Caribe em Ciências da Saúde. Dois autores independentes selecionaram estudos que atendiam aos critérios de elegibilidade, os quais foram organizados usando o Rayyan.ai. Os achados de imagem foram descritos usando tomografia computadorizada (TC), ressonância magnética (RM) convencional, sequências avançadas de RM ou medicina nuclear, com foco em tomografia computadorizada por emissão de fóton único, com e sem cloreto de tálio-201, e tomografia por emissão de pósitrons/TC. Os dados extraídos focaram na topografia das lesões, características de sinal, realce, restrição à difusão e, quando disponíveis, achados de espectroscopia e perfusão. Para ilustrar características de imagem típicas e atípicas, foi incluída uma série de casos complementar, referente a pacientes com neurotoxoplasmose confirmada. A revisão demonstra que a TC e a RM permanecem essenciais para o diagnóstico e acompanhamento, enquanto sequências avançadas de RM fornecem valor adicional na diferenciação da toxoplasmose de outras infecções oportunistas e neoplasias.
Palavras-chave:
Toxoplasma; Toxoplasmose cerebral/diagnóstico; Toxoplasmose/diagnóstico por imagem; Neuroimagem
INTRODUCTION
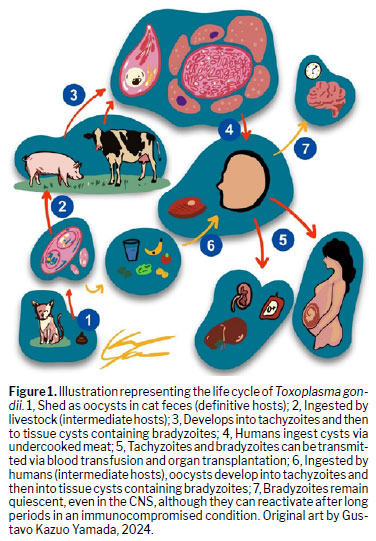
Toxoplasma gondii is a protozoan of the phylum Apicomplexa whose definitive hosts are cats. However, it can infect many intermediate hosts, including all mammals and birds. Humans are typically infected by ingesting oocysts in food, acting as definitive hosts, or consuming undercooked meat containing viable cysts, acting as intermediate hosts. Transmission can also occur through blood transfusions and organ transplants, as well as through vertical transmission, leading to cases of congenital toxoplasmosis(1,2). Figure 1 illustrates the life cycle of T. gondii. It is, therefore, a highly prevalent, ubiquitous infection, with approximately 25–30% of the global population currently infected by the parasite, being most prevalent in Latin American and African nations(3–5). Despite its high prevalence, most acquired forms of toxoplasmosis in immunocompetent individuals are mild(6). However, latent stages of the protozoan can remain dormant and later reactivate in immunosuppressed and congenitally infected individuals, primarily targeting the central nervous system (CNS). In addition, toxoplasmosis is the leading cause of cerebral mass lesions in immunosuppressed patients with HIV/AIDS who are not receiving appropriate prophylaxis. According to the literature, most cases of cerebral toxoplasmosis in HIV-infected patients are associated with low CD4+ counts, especially below 100 cells/µL(7–9). Cerebral toxoplasmosis also occurs in other forms of immunosuppression, most notably in individuals using immunosuppressive agents for the treatment of autoimmune diseases, with a wide variety of cases being reported in the literature. Durieux et al.(10)described a multicenter analysis and literature review on this subject, concluding that the most common drugs associated with cerebral toxoplasmosis were corticosteroids, antimetabolites, and anti-tumor necrosis factor alpha. Furthermore, reports in the literature have showcased cerebral toxoplasmosis as a possibility in patients treated with biologic agents such as the monoclonal antibodies rituximab, adalimumab, and infliximab(11,12). It is important to differentiate between the manifestations of cerebral toxoplasmosis and the primary neuropsychiatric manifestations seen in systemic lupus erythematosus(13).
Transplant recipients are also affected by cerebral toxoplasmosis, including those undergoing solid organ transplantation, especially kidney, liver, and heart transplant recipients, and those undergoing hematopoietic stem cell transplantation (HSCT). A multicenter analysis of transplant recipients in Europe showed that the prevalence of cerebral toxoplasmosis was highest among HSCT recipients
(14), among whom it has been found to be the most common CNS infection
(14,15). In patients with cancer, toxoplasmosis is also a possibility, albeit a relatively uncommon opportunistic disease. Among such patients, cerebral toxoplasmosis is most common in those with hematological malignancies, especially Hodgkin lymphoma
(16).
In patients with cerebral toxoplasmosis, the most common symptoms are headaches, fever, focal deficits, hemiparesis, ataxia, cranial nerve palsies, changes in consciousness, and seizures. More rarely, chorea, ballismus, and rigidity can be observed
6,7).
A definitive diagnosis of cerebral toxoplasmosis can be made only through histopathological analysis of brain biopsies, the gold-standard diagnostic modality, or molecular assays to identify
T. gondii DNA in cerebrospinal fluid (CSF). However, these procedures have considerable limitations: biopsies are invasive and depend on the location of the lesion and the clinical condition of the patient; and access to molecular assays is limited (especially in low- and middle-income countries). Although polymerase chain reaction of CSF has high (96–100%) specificity for diagnosing cerebral toxoplasmosis, it is significantly less sensitive and a negative result therefore cannot rule out the disease
(6,7,17). In fact, evaluation of the CSF is irrelevant in diagnosing the disease, given that toxoplasmosis rarely involves the meninges, and CSF changes are usually nonspecific. Similarly, serological diagnosis is not particularly elucidative, because cerebral toxoplasmosis is related to reactivation of latent infection and immunoglobulin M (IgM) titers are therefore negative. In addition, the presence of
T. gondii IgG antibodies is inconclusive, because high IgG titers do not necessarily indicate the presence of
T. gondii, and the absence of such antibodies is also insufficient to rule out cerebral toxoplasmosis
(6–8). Therefore, neuroimaging plays a pivotal role in the diagnosis and emerges as an important resource in overcoming these limitations. It establishes a presumptive diagnosis of the disease by identifying one or more brain lesions that are consistent with the disease and improve after 10–14 days of specific treatment
(7,8,18).
The aim of this study was to assess the importance of neuroimaging methods in the correct diagnosis of cerebral toxoplasmosis. To that end, we conducted a systematic review of the literature and a retrospective analysis of confirmed cases from a tertiary university hospital.
METHODSProtocol and registrationThis systematic review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines. The review protocol was registered in the International Prospective Register of Systematic Reviews (ID: CRD420251107718).
Search strategy and study selectionStudies were selected from the following databases: Embase; Latin-American and Caribbean Health Sciences Literature; PubMed, and Scopus. Only studies published in English, Spanish, or Portuguese were included. The search terms included the following: cerebral toxoplasmosis, neurotoxoplasmosis; central nervous system toxoplasmosis; magnetic resonance imaging; MRI; diffusion-weighted imaging; DWI; magnetic resonance spectroscopy; perfusion imaging; computed tomography; CT; CT scan; diagnosis; diagnostic imaging; diagnostic accuracy; sensitivity; and specificity.
The AI-powered software Rayyan (Qatar Computing Research Institute, Doha, Qatar) was used in order to organize the selected studies. Two researchers, each with at least 5 years of experience in the field, conducted the database searches and study selection. The two researchers, working independently, assessed the eligibility of the articles found, with discrepancies being resolved through discussion. The initial screening was based on the titles and abstracts of the paper, and the full texts were then analyzed to determine whether they include analyses if imaging methods, for inclusion or exclusion.
Eligibility criteriaThe review included studies involving human patients of any age, gender, or immunological status, with a confirmed or suspected diagnosis of cerebral toxoplasmosis, based on clinical, laboratory, or radiological criteria. Eligible studies included those employing magnetic resonance imaging (MRI) or computed tomography (CT) of the brain or spine, using conventional sequences—T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), fluid-attenuated inversion recovery (FLAIR) sequences, or contrast-enhanced sequences—or advanced MRI techniques—diffusion-weighted imaging (DWI), spectroscopy, or perfusion MRI). Studies featuring imaging findings obtained from other nuclear imaging modalities, such as single-photon-emission computed tomography (SPECT), with or without thallium-201, and positron-emission tomography/CT (PET/CT), were also included. We included only observational studies (cohort, case-control, or cross-sectional studies) and case series with five or more patients. Therefore, case reports with fewer than five patients, reviews, editorials, animal studies, and
in vitro studies were excluded, as were studies involving patients with CNS coinfections (e.g., cryptococcosis or tuberculosis), without separate data for toxoplasmosis, and studies with insufficient neuroimaging data.
Data extractionIn this retrospective study, we reviewed CT, MRI, PET/CT and SPECT scans of cases with a confirmed or suspected diagnosis of toxoplasmosis. In addition to data from the literature, illustrative CT and MRI scans of patients with confirmed cerebral toxoplasmosis from a tertiary university hospital were included in order to exemplify typical and atypical findings. Structural images and advanced sequences were obtained in 1.5-T and 3.0-T MRI scanners (Achieva; Philips Medical Systems, Best, the Netherlands). The following characteristics were analyzed by an experienced neuroradiologist (with over 20 years of experience): topography; diffusion-weighted aspects; T1WI and T2WI signal intensity; enhancement pattern; spectroscopy findings (if available); and perfusion MRI findings (if available). No authors were contacted for missing information, and no additional data beyond those published were requested.
Data synthesisThe findings were summarized in narrative format and in structured tables. The focus was on information related to imaging modalities, imaging findings, and diagnostic accuracy.
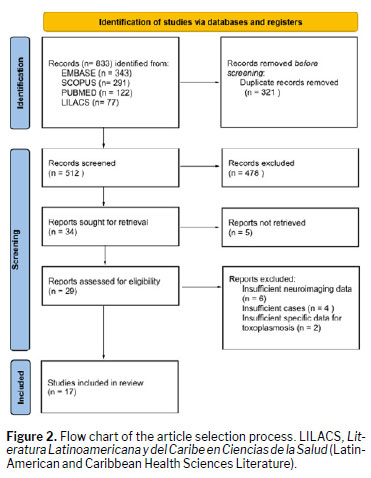
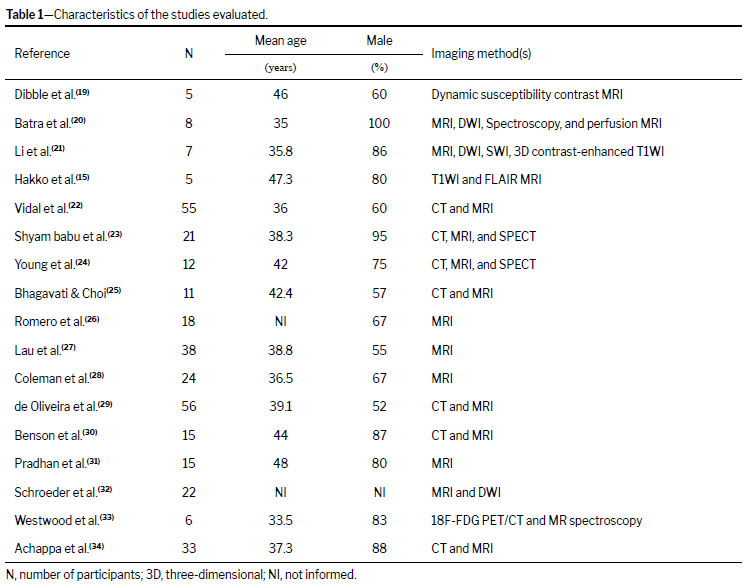
RESULTSVia our search strategy, 833 studies were selected. From those, 321 duplicates were removed. During the initial screening, titles and abstracts were reviewed, resulting in the exclusion of 478 articles. In addition, five studies were inaccessible. Therefore, 29 studies were included in the full-text analysis. Finally, after the full manuscript review, 17 studies were found to meet the eligibility criteria and were selected for inclusion in the systematic review. Figure 2 shows the article selection process. The details of the selected studies are shown in Table 1. The results of the review are summarized in Table 2 and Table 3.
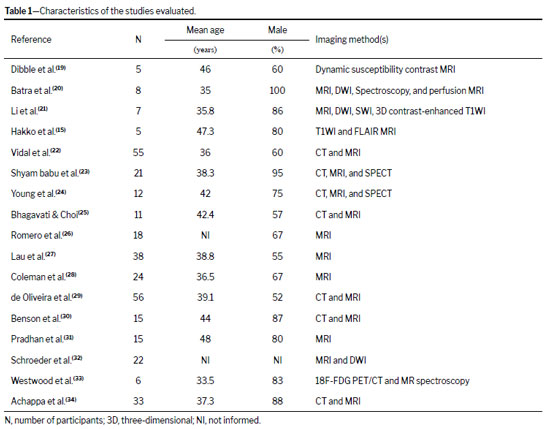
The mean age of the patients involved was 39.6 years (range, 33.5–48.0 years). In most of the study samples, there was a predominance of males, with proportions as high as 80–90% in some samples. The majority of patients were immunocompromised, primarily due to advanced HIV/AIDS, and some samples included patients who had undergone transplantation or had other immunosuppressive conditions.
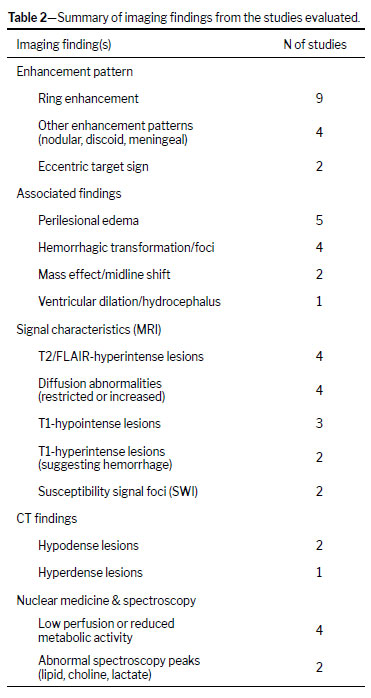
The most common CT finding was that of hypodense lesions with surrounding vasogenic edema and mass effect, typically showing ring or nodular contrast enhancement. The use of MRI revealed hypointense lesions on T1WI and hyperintense signals on T2/FLAIR sequences, with characteristic peripheral ring enhancement. The eccentric target sign was cited in only two studies, with no mention of the concentric target sign
(22,24). The DWI findings were varied, with some studies reporting restricted diffusion and others suggesting mixed or absent restriction; susceptibility-weighted imaging (SWI) typically showed complete, smooth, low-signal-intensity rims; perfusion MRI revealed low relative cerebral blood volume; and MR spectroscopy commonly demonstrated an elevated lipid peak with reduced choline and N-acetylaspartate.
Nuclear medicine studies were important in differentiating toxoplasmosis from primary CNS lymphoma. In many cases, technetium-99m (
99mTc) SPECT suggested inflammatory lesions; thallium-201 (201Tl) SPECT showed lower uptake in toxoplasmosis-related lesions than in lymphoma-related lesions; and
18F-fluorodeoxyglucose (
18F-FDG) PET/CT consistently demonstrated low or nonexistent intralesional metabolic activity, thus differentiating it from the elevated activity present in lymphoma lesions.
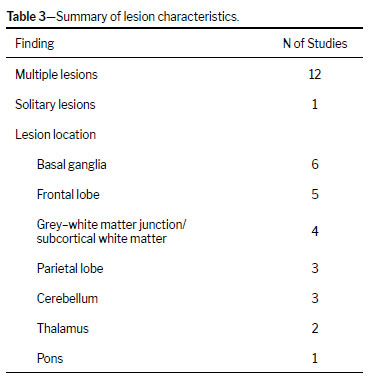
In the majority of studies, multiple lesions were described as the most common pattern in cerebral toxoplasmosis. Only one study cited solitary lesions as being the more common presentation, and there were four studies in which the pattern of lesion distribution was not reported
(31). Seven studies provided information on the total number of lesions; the mean number of lesions per patient was 5.47. The most common lesion locations were the basal ganglia and frontal lobe, whereas the least common sites were the pons and the deep grey matter.
DISCUSSIONImages were collected to demonstrate the most common patterns and some differential diagnoses.
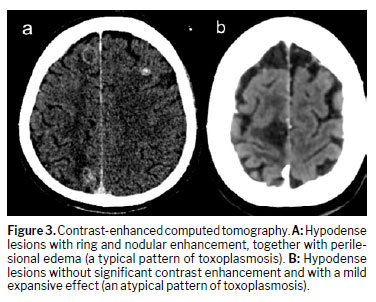
CTDespite being less sensitive than MRI, especially for smaller lesions, CT can also be used for the initial diagnosis of cerebral toxoplasmosis. The typical pattern observed on CT (in approximately 80% of cases) is one of hypodense lesions with perilesional vasogenic edema, with ring or nodular enhancement on contrast-enhanced images. Atypical patterns on CT (in approximately 20% of cases) include hypodense lesions without enhancement and with mass effect and diffuse cerebral edema without visible focal lesions. The most common lesion locations on CT are the basal ganglia and corticomedullary junction (in approximately 85% of cases), with multiple lesions
(35,36). Figure 3 shows lesions at the corticomedullary junction.
MRIThe gold-standard imaging modality for evaluating patients with suspected cerebral toxoplasmosis is MRI. Studies
(6,8,35)have proven that MRI is more sensitive than is CT, because it can accurately diagnose lesions that would be otherwise misinterpreted. In addition, MRI has a higher histopathological correlation, representing a reliable option with fewer false-negative results. On MRI, findings of expansile mass lesions, with peripheral (ring) enhancement, often with an eccentric mural nodule, in patients with immunosuppression indicate cerebral toxoplasmosis as the most likely diagnosis, with differential hypotheses being considered only when there is no response within the first 14 days of the specific treatment for toxoplasmosis.
Two specific findings on MRI are the eccentric target sign and the concentric target sign
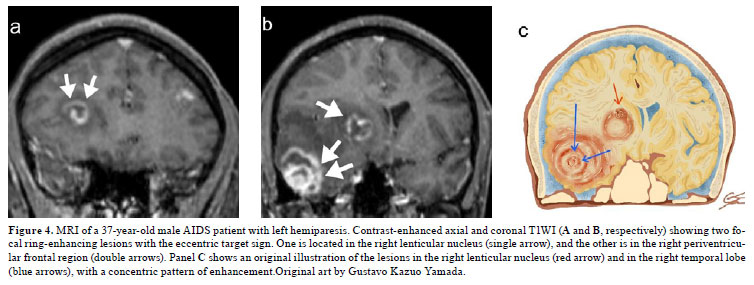
(36,37). Present in approximately 30% of cases, the eccentric target sign is depicted on contrast-enhanced T1WI and consists of an enhanced inner eccentric core, a hypointense intermediate zone, and an enhanced peripheral border
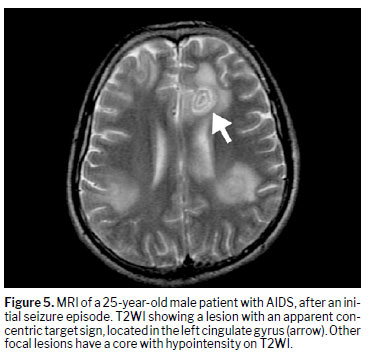
(38), as illustrated in Figure 4, with 95% specificity and 25% sensitivity for the diagnosis of cerebral toxoplasmosis. It may indicate hemorrhage or coagulative necrosis of the tissue, and can be accompanied by external areas of edema and inflammatory cell infiltration. The concentric target sign is depicted on T2WI or FLAIR sequences and is characterized by alternating patterns of concentric zones of hypointensity and hyperintensity in deep parenchymal lesions (Figure 5). It is believed to be more specific for cerebral toxoplasmosis than is the eccentric target sign, although its specificity and histopathological correlation require further validation
(39–41).
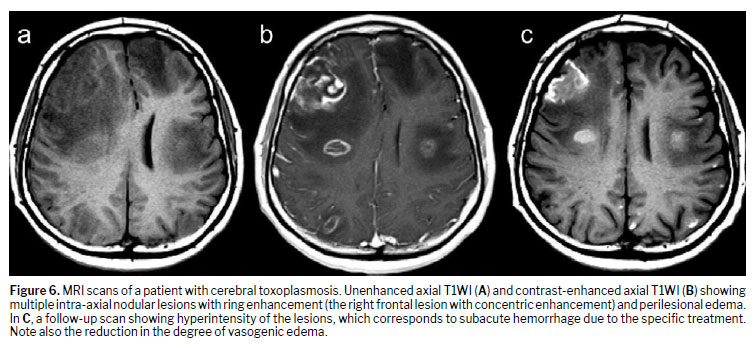
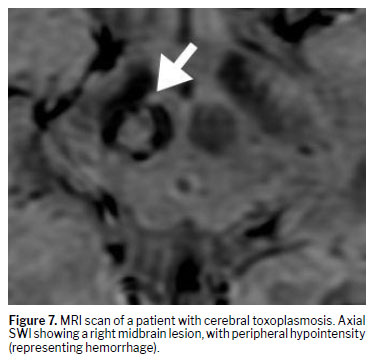
In the vast majority of patients with cerebral toxoplasmosis, SWI shows foci of intralesional susceptibility signals, most probably representing hemorrhage, as illustrated in Figure 6 (on T1WI) and Figure 7 (on SWI). It is important to note how these findings aren’t unique to toxoplasmosis, although SWI techniques have superior sensitivity in detecting hemorrhagic lesions
(30). SWI images are important to depict calcifications and hemorrhage as areas of hypointense signal intensity
(41).
Advanced imaging techniquesAdvanced imaging techniques are other important tools for identifying cerebral toxoplasmosis lesions. On DWI, restricted diffusion may be seen at the periphery of the lesions. However, the apparent diffusion coefficient (ADC) value is less reliable, with conflicting findings in the literature, in which there is a wide spectrum of ADC values, with varying results even between lesions in the same patient in some studies,
(33) whereas other studies have shown high ADC values (indicating that there is no restricted diffusion) for toxoplasmosis-related lesions and relatively lower ADC values for lymphoma-related lesions
(21,42,43).
Dynamic susceptibility contrast-enhanced T2-weighted gradient echo echo planar sequences acquired during the first pass of a standard dose of gadolinium-based contrast agent shows reduced relative cerebral blood volume (rCBV) in toxoplasmosis lesions and in the surrounding edema, which results from a lack of vasculature in the lesions and vasoconstriction caused by increased interstitial pressure in the edema, respectively. The rCBV levels are lower in toxoplasmosis-related lesions than in lymphoma-related lesions, which facilitates the diagnosis
(44).
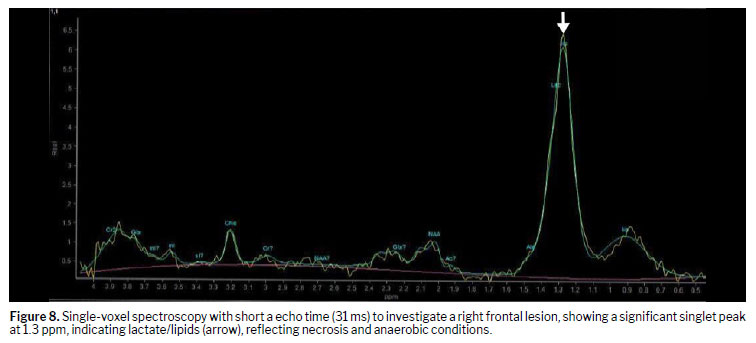
Magnetic resonance spectroscopy provides information about the metabolic profile beyond the anatomical information and has been extensively used to evaluate brain focal lesions. In toxoplasmosis, there is classically the presence and elevation of lipid and lactate peaks, accompanied by reduction of the other metabolites, such as creatine, choline, N-acetylaspartate, and myoinositol, as demonstrated in Figure 8
(45). However, the technique is only modestly capable of differentiating toxoplasmosis from lymphoma. The occurrence of an overlap in metabolic values between the two conditions is widely reported in the literature, although some studies also state the existence of unique profiles, such elevated choline levels in lymphomas
(34).
Molecular imagingMolecular imaging is increasingly employed, especially with techniques such as SPECT and
18F-FDG PET. It has been shown that there is no uptake of thallium-201 by cerebral toxoplasmosis lesions on 201Tl SPECT. In addition,
18F-FDG PET/CT is an important diagnostic tool for cerebral toxoplasmosis, showing that there is less
18F-FDG uptake by toxoplasmosis lesions than by normal brain cortex.
The application of molecular imaging is useful in differentiating cerebral toxoplasmosis lesions from primary lymphomas, the latter characterized by higher uptake values. That being said,
18F-FDG-PET/CT should be implemented when neuroimaging findings are inconclusive or atypical for cerebral toxoplasmosis. In addition, the diagnostic value of 201Tl SPECT has decreased considerably due to increased uptake in patients with cerebral toxoplasmosis undergoing highly active antiretroviral therapy
(46). Therefore,
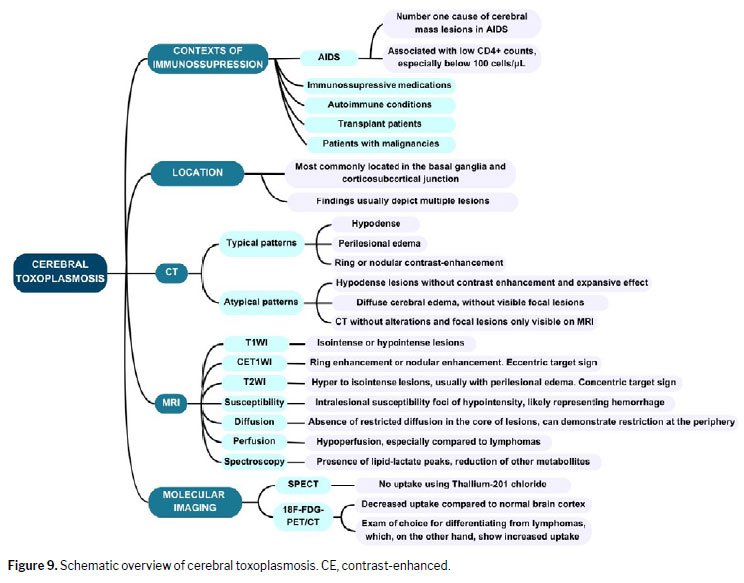
18F-FDG-PET/CT is now the molecular imaging examination of choice, being particularly helpful in diagnosing patients suspected of having cerebral toxoplasmosis who do not respond to specific therapy. Figure 9 provides an overview of findings in cerebral toxoplasmosis.
Specific clinical presentationsT. gondii myelitisCases of myelopathy associated with
T. gondii infection are rare, with few examples reported. Data in the literature suggest that myelitis is a finding present mostly in AIDS patients
(47,48). Classical symptoms related to spinal cord toxoplasmosis are motor loss (mainly affecting the lower extremities), paraparesis, bilateral sensory loss with specific spinal level, bladder dysfunction, and lumbar pain. Lastly, a review of the literature has shown that simultaneous cerebral and spinal cord involvement is common, as described in half of the analyzed cases
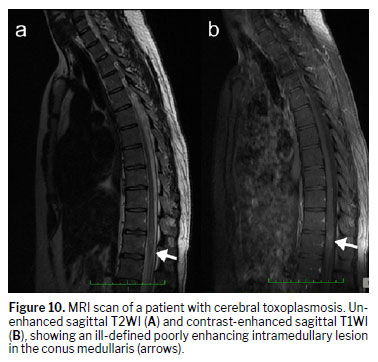
(49). Infectious myelopathy is characterized by hyperintensity on T2WI sequences and hypointensity on T1WI sequences. In addition, the lesions are classically associated with longitudinal spinal cord edema and intense, heterogeneous contrast enhancement. Toxoplasmosis-related lesions preferentially affect the thoracic spinal cord segments. Figure 10 shows a toxoplasmosis-related lesion in an unusual location (the conus medullaris).
Cerebral toxoplasmosis and immune reconstitution inflammatory syndromeImmune reconstitution inflammatory syndrome (IRIS) represents a paradoxical deterioration of an opportunistic infection despite immunological recovery during treatment. In the case of cerebral toxoplasmosis, patients might develop a CNS-related form of IRIS, marking a worsening of the neurological condition. In patients with toxoplasmosis and HIV infection, there is an increase in the CD4+ cell count after antiretroviral therapy, which mediates the exacerbation via trafficking of CD4 and CD8 T lymphocytes to the nervous system. The combination of cerebral toxoplasmosis and CNS-IRIS has rarely been described in the literature, with other opportunistic infections appearing as more likely differential diagnoses, such as chronic infection with a mycobacterial, viral, or fungal pathogen. Histopathological proof of extensive inflammatory granulomatous processes does not affect the diagnosis or treatment of cerebral toxoplasmosis, only lengthening its natural clinical course
(50–52). In cases of CNS-IRIS caused by opportunistic pathogens, contrast-enhancing lesions in the brain are usually found. However, because cases of cerebral toxoplasmosis with and without IRIS have similar neuroimaging appearances, it is often necessary to take the clinical scenario and neuropathology into account in order to differentiate between them
(53,54).
Differential diagnosisLocal epidemiology is an important factor to explore when determining the differential diagnosis of toxoplasmosis. In high-income countries, primary CNS lymphoma (PCNSL) is the main differential diagnosis, whereas focal forms of cerebral tuberculosis (tuberculomas and tuberculous abscesses) are the main alternatives in low- and middle-income countries. Cerebral toxoplasmosis and PCNSL can both cause contrast-enhancing lesions with mass effect
(4,8).
PCNSLPatients with AIDS or other immunosuppressive conditions have a higher probability of PCNSL presenting as multifocal lesions with necrosis and hemorrhage. Differentiating between PCNSL-related lesions and toxoplasmosis-related lesions may be difficult
(46).
Tuberculosis of the CNSTuberculomas and tuberculous abscesses usually appear on CT images as solitary or multiple ring-enhancing lesions with a hypodense center and surrounding vasogenic edema. A central calcification surrounded by a ring of enhancement, known as a target sign, is also common, although none of its appearances on CT are specific for tuberculomas. MRI is the preferred method for diagnosing possible tuberculomas is MRI, which reveals different possible patterns of enhancement: irregular, ring-like, open rings, and lobular. It should be borne in mind that tuberculomas can assume various patterns depending on the stage of the disease and the immunological status of the patient. As on CT scans, tuberculous abscesses appear as typical cerebral abscesses on MRI
(55–58), and restricted diffusion can be observed in the necrotic component. Leptomeningitis (with leptomeningeal enhancement) is also common in tuberculosis.
ParacoccidioidomycosisParacoccidioidomycosis is a neglected tropical disease that is especially prevalent in Latin America, representing the leading cause of death due to systemic mycosis in immunocompetent patients in Brazil
(59–61). Involvement of the CNS can manifest as intraparenchymal or meningeal lesions, with the latter being less common. The intraparenchymal manifestations are granulomas classically located in the brain hemispheres, appearing as irregular lesions with mass effect, peripheral contrast-enhancement, and perilesional edema. The meningeal forms are associated with leptomeningeal contrast enhancement and small cortical nodules. Lastly, spectroscopy can show a trehalose peak in paracoccidioidomycosis and other fungal infections
(62–65).
CryptococcosisCryptococcosis is an infectious disease caused by pathogenic encapsulated yeasts of the genus
Cryptococcus, mainly
C. neoformans and
C. gattii. Like toxoplasmosis, cryptococcosis is especially harmful in immunocompromised hosts with AIDS. Typical imaging findings of cryptococcal meningoencephalitis include dilated perivascular spaces, pseudocysts, cryptococcomas, leptomeningeal or parenchymal enhancing lesions, and the hazy brain base sign.
Dilated perivascular spaces are common in immunocompetent and immunocompromised hosts alike
(66). The perivascular spaces are part of the glymphatic system, surrounding the vessels to protect them from mechanical injury and to allow chemical exchanges, mainly the depuration of toxins.
Cryptococcomas are intra-axial cryptococcal granulomas that are more common in immunocompetent hosts. These lesions usually show hypointensity on T1WI and hyperintensity on T2WI, with a ring or nodular enhancement and surrounding vasogenic edema
(67-69).
Leptomeningeal involvement, associated with focal parenchymal edema, tends to be mild, similar to immune reactions. The most sensitive imaging modality to demonstrate these findings is a contrast-enhanced FLAIR sequence, which typically reveals infratentorial lesions. The hazy brain base sign represents a pattern seen in typical cryptococcal meningitis, probably indicating fungal yeast penetration of the basal parenchyma along the perivascular spaces
(70).
Future directionsThe diagnosis of cerebral toxoplasmosis remains a challenging task. Although radiological findings can reliably help the process, the diagnosis is confirmed only if the patient responds to the specific treatment, because the symptoms and signs overlap with those of the differential diagnoses. Therefore, it is imperative to further evaluate new diagnostic modalities, such as the use of biomarkers that could help diagnose and possibly assess the treatment response. Molecular biology methods have great diagnostic potential, substantiating the need for a cost-effective technique that is highly sensitive and specific. In addition, identifying genetic risk factors for reactivation of cerebral toxoplasmosis should facilitate the stratification of patients. Furthermore, the study of imaging techniques already in use should continue, to better evaluate their sensitivity and specificity in diagnosing cerebral toxoplasmosis.
CONCLUSIONCerebral toxoplasmosis is a relevant condition in immunosuppressed and congenitally infected individuals, being the leading cause of cerebral mass lesions in patients with AIDS. Encephalitis represents the most common clinical manifestation, typically with multiple lesions in the basal ganglia. However, it is a multifaceted condition presenting in various patterns, including the rare occurrence of infectious myelitis. Advanced MRI techniques may aid in the diagnosis, because typical toxoplasmosis-related lesions do not demonstrate restricted diffusion in their core, do not have increased perfusion (i.e., show no increase in rCBV values), and, on spectroscopy, may show an increase in the peaks of lipids and lactate, with reductions in the other metabolites.
After reviewing the literature, we can state that neuroimaging, especially MRI, is an essential tool for the early diagnosis of toxoplasmosis, for the evaluation of its initial extent, and for monitoring treatment responses. We found that CT and MRI consistently demonstrate findings characteristic of the disease, with advanced techniques and nuclear medicine studies improving the distinction from differential diagnoses, most importantly, PCNSL. Most patients respond favorably to treatment, although residual complications such as calcifications and intralesional hemorrhage have been reported. The characteristic eccentric target sign was reported in only a small portion of the studies included in our review, with no mention of the concentric target sign. Therefore, a multimodal imaging approach is essential to increase diagnostic accuracy and support clinical decision-making.
AcknowledgmentsThis work received financial support from the Brazilian
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq, National Council for Scientific and Technological Development (Grant no. 305981/2023-4).
REFERENCES1. Montoya JG, Liesenfeld O. Toxoplasmosis. Lancet. 2004 Jun 12;363(9425):1965-76. doi: 10.1016/S0140-6736(04)16412-X. PMID: 15194258.
2. Lyons RE, McLeod R, Roberts CW. Toxoplasma gondii tachyzoite-bradyzoite interconversion. Trends Parasitol. 2002 May;18(5):198-201. doi: 10.1016/s1471-4922(02)02248-1. PMID: 11983592.
3. Pappas G, Roussos N, Falagas ME. Toxoplasmosis snapshots: global status of Toxoplasma gondii seroprevalence and implications for pregnancy and congenital toxoplasmosis. Int J Parasitol. 2009 Oct;39(12):1385-94. doi: 10.1016/j.ijpara.2009.04.003. Epub 2009 May 9. PMID: 19433092.
4. Vidal JE. HIV-Related Cerebral Toxoplasmosis Revisited: Current Concepts and Controversies of an Old Disease. J Int Assoc Provid AIDS Care. 2019 Jan-Dec;18:2325958219867315. doi: 10.1177/2325958219867315. PMID: 31429353; PMCID: PMC6900575.
5. Elsheikha HM, Marra CM, Zhu XQ. Epidemiology, Pathophysiology, Diagnosis, and Management of Cerebral Toxoplasmosis. Clin Microbiol Rev. 2020 Nov 25;34(1):e00115-19. doi: 10.1128/CMR.00115-19. PMID: 33239310; PMCID: PMC7690944.
6. Pereira-Chioccola VL, Vidal JE, Su C. Toxoplasma gondii infection and cerebral toxoplasmosis in HIV-infected patients. Future Microbiol. 2009 Dec;4(10):1363-79. doi: 10.2217/fmb.09.89. PMID: 19995194.
7. Marra CM. Central nervous system infection with Toxoplasma gondii. Handb Clin Neurol. 2018;152:117-122. doi: 10.1016/B978-0-444-63849-6.00009-8. PMID: 29604970.
8. Dian S, Ganiem AR, Ekawardhani S. Cerebral toxoplasmosis in HIV-infected patients: a review. Pathog Glob Health. 2023 Feb;117(1):14-23. doi: 10.1080/20477724.2022.2083977. Epub 2022 Jun 11. PMID: 35694771; PMCID: PMC9848325.
9. Dwinata IM, Widyadharma IPE, Dewi PR, Tedyanto EH. Risk factors of cerebral toxoplasmosis in HIV patients: A systematic review. Rom J Neurol. 2021;20(3):143-148. doi: 10.37897/RJN.2021.3.7.
10. Durieux MF, Lopez JG, Banjari M, Passebosc-Faure K, Brenier-Pinchart MP, Paris L, Gargala G, Berthier S, Bonhomme J, Chemla C, Villena I, Flori P, Fréalle E, L’Ollivier C, Lussac-Sorton F, Montoya JG, Cateau E, Pomares C, Simon L, Quinio D, Robert-Gangneux F, Yera H, Labriffe M, Fauchais AL, Dardé ML. Toxoplasmosis in patients with an autoimmune disease and immunosuppressive agents: A multicenter study and literature review. PLoS Negl Trop Dis. 2022 Aug 8;16(8):e0010691. doi: 10.1371/journal.pntd.0010691. PMID: 35939518; PMCID: PMC9387931.
11. Pulivarthi S, Reshi RA, McGary CT, Gurram MK. Cerebral toxoplasmosis in a patient on methotrexate and infliximab for rheumatoid arthritis. Intern Med. 2015;54(11):1433-6. doi: 10.2169/internalmedicine.54.3977. Epub 2015 Jun 1. PMID: 26028002.
12. de Almeida GB, Cristóvão M, Pontinha C, Januário G. Cerebral Toxoplasmosis as an Uncommon Complication of Biologic Therapy for Rheumatoid Arthritis: Case Report and Review of the Literature. Brain Sci. 2022 Aug 8;12(8):1050. doi: 10.3390/brainsci12081050. PMID: 36009113; PMCID: PMC9405725.
13. de Amorim JC, Torricelli AK, Frittoli RB, Lapa AT, Dertkigil SSJ, Reis F, Costallat LT, França Junior MC, Appenzeller S. Mimickers of neuropsychiatric manifestations in systemic lupus erythematosus. Best Pract Res Clin Rheumatol. 2018 Oct;32(5):623-639. doi: 10.1016/j.berh.2019.01.020. Epub 2019 Feb 22. PMID: 31203921.
14. Robert-Gangneux F, Meroni V, Dupont D, Botterel F, Garcia JMA, Brenier-Pinchart MP, Accoceberry I, Akan H, Abbate I, Boggian K, Bruschi F, Carratalà J, David M, Drgona L, Djurković-Djaković O, Farinas MC, Genco F, Gkrania-Klotsas E, Groll AH, Guy E, Hirzel C, Khanna N, Kurt Ö, Junie LM, Lazzarotto T, Len O, Mueller NJ, Munoz P, Pana ZD, Roilides E, Stajner T, van Delden C, Villena I, Pelloux H, Manuel O. Toxoplasmosis in Transplant Recipients, Europe, 2010-2014. Emerg Infect Dis. 2018 Aug;24(8):1497-1504. doi: 10.3201/eid2408.180045. PMID: 30014843; PMCID: PMC6056100.
15. Hakko E, Ozkan HA, Karaman K, Gulbas Z. Analysis of cerebral toxoplasmosis in a series of 170 allogeneic hematopoietic stem cell transplant patients. Transpl Infect Dis. 2013 Dec;15(6):575-80. doi: 10.1111/tid.12138. Epub 2013 Sep 18. PMID: 24103000.
16. Israelski DM, Remington JS. Toxoplasmosis in patients with cancer. Clin Infect Dis. 1993 Nov;17 Suppl 2:S423-35. doi: 10.1093/clinids/17.supplement_2.s423. PMID: 8274608.
17. Dubey JP. Toxoplasma Gondii. In: Baron S, editor. Medical Microbiology. 4th ed. Galveston (TX): University of Texas Medical Branch at Galveston; 1996. Chapter 84. PMID: 21413265.
18. Júnior JRLA. Fundamentação histopatológica das alterações de imagem por ressonância magnética das lesões no sistema nervoso central de pacientes com síndrome de imunodeficiência adquirida e neurotoxoplasmose [dissertation]. Recife, Brazil: Universidade Federal de Pernambuco, Departamento de Patologia; 2006.
19. Dibble EH, Boxerman JL, Baird GL, Donahue JE, Rogg JM. Toxoplasmosis versus lymphoma: Cerebral lesion characterization using DSC-MRI revisited. Clin Neurol Neurosurg. 2017 Jan;152:84-89. doi: 10.1016/j.clineuro.2016.11.023. Epub 2016 Dec 2. PMID: 27940418.
20. Batra A, Tripathi RP, Gorthi SP. Magnetic resonance evaluation of cerebral toxoplasmosis in patients with the acquired immunodeficiency syndrome. Acta Radiol. 2004 Apr;45(2):212-21. doi: 10.1080/02841850410003969. PMID: 15191109.
21. Li J, Xue M, Lv Z, Guan C, Huang S, Li S, Liang B, Zhou X, Chen B, Xie R. Differentiation of Acquired Immune Deficiency Syndrome Related Primary Central Nervous System Lymphoma from Cerebral toxoplasmosis with Use of Susceptibility-Weighted Imaging and Contrast Enhanced 3D-T1WI. Int J Infect Dis. 2021 Dec;113:251-258. doi: 10.1016/j.ijid.2021.10.023. Epub 2021 Oct 17. PMID: 34670145.
22. Vidal JE, Hernandez AV, de Oliveira AC, Dauar RF, Barbosa SP Jr, Focaccia R. Cerebral toxoplasmosis in HIV-positive patients in Brazil: clinical features and predictors of treatment response in the HAART era. AIDS Patient Care STDS. 2005 Oct;19(10):626-34. doi: 10.1089/apc.2005.19.626. PMID: 16232047.
23. Shyam babu C, Satishchandra P, Mahadevan A, Pillai Shibu V, Ravishankar S, Sidappa N, Udaykumar R, Ravi V, Shankar SK. Usefulness of stereotactic biopsy and neuroimaging in management of HIV-1 Clade C associated focal brain lesions with special focus on cerebral toxoplasmosis. Clin Neurol Neurosurg. 2013 Jul;115(7):995-1002. doi: 10.1016/j.clineuro.2012.10.012. Epub 2012 Nov 12. PMID: 23153789; PMCID: PMC4483268.
24. Young RJ, Ghesani MV, Kagetsu NJ, Derogatis AJ. Lesion size determines accuracy of thallium-201 brain single-photon emission tomography in differentiating between intracranial malignancy and infection in AIDS patients. AJNR Am J Neuroradiol. 2005 Sep;26(8):1973-9. PMID: 16155145; PMCID: PMC8148819.
25. Bhagavati S, Choi J. Frequent hemorrhagic lesions in cerebral toxoplasmosis in AIDS patients. J Neuroimaging. 2009 Apr;19(2):169-73. doi: 10.1111/j.1552-6569.2008.00274.x. PMID: 19705517.
26. Romero YO, Reyes Rodriguez C, Salomón LJA, Rodríguez CL. Aspectos clinicoepidemiológicos e imagenológicos de pacientes con virus de inmunodeficiencia humana/sida y diagnóstico de neurotoxoplasmosis. Medisan. 2022 Dec 1;26(6).
27. Lau A, Jain MK, Chow JY, Kitchell E, Lazarte S, Nijhawan A. Toxoplasmosis Encephalitis: A Cross-Sectional Analysis at a U.S. Safety-Net Hospital in the Late cART Era. J Int Assoc Provid AIDS Care. 2021 Jan-Dec;20:23259582211043863. doi: 10.1177/23259582211043863. PMID: 34663116; PMCID: PMC8529305.
28. Coleman B, Smith BR, Kapoor R, Proschan MA, Sereti I, Hammoud DA, Kovacs JA. Persistence of Human Immunodeficiency Virus-Associated Cerebral Toxoplasmosis Lesions in Successfully Treated Patients Receiving Combination Antiretroviral Therapy. Open Forum Infect Dis. 2023 Apr 19;10(5):ofad208. doi: 10.1093/ofid/ofad208. PMID: 37213420; PMCID: PMC10199119.
29. de Oliveira GB, da Silva MA, Wanderley LB, da Cunha Correia C, Ferreira EC, de Medeiros ZM, Filho JL, de Melo FL, de Araújo PS, Santos AH. Cerebral toxoplasmosis in patients with acquired immune deficiency syndrome in the neurological emergency department of a tertiary hospital. Clin Neurol Neurosurg. 2016 Nov;150:23-26. doi: 10.1016/j.clineuro.2016.08.014. Epub 2016 Aug 16. PMID: 27573702.
30. Benson JC, Cervantes G, Baron TR, Tyan AE, Flanagan S, Lucato LT, McKinney AM, Ott F. Imaging features of neurotoxoplasmosis: A multiparametric approach, with emphasis on susceptibility-weighted imaging. Eur J Radiol Open. 2018 Mar 17;5:45-51. doi: 10.1016/j.ejro.2018.03.004. PMID: 29719858; PMCID: PMC5926851.
31. Pradhan S, Yadav R, Mishra VN. Toxoplasma meningoencephalitis in HIV-seronegative patients: clinical patterns, imaging features and treatment outcome. Trans R Soc Trop Med Hyg. 2007 Jan;101(1):25-33. doi:10.1016/j.trstmh.2006.02.021.
32. Schroeder PC, Post MJ, Oschatz E, Stadler A, Bruce-Gregorios J, Thurnher MM. Analysis of the utility of diffusion-weighted MRI and apparent diffusion coefficient values in distinguishing central nervous system toxoplasmosis from lymphoma. Neuroradiology. 2006 Oct;48(10):715-20. doi: 10.1007/s00234-006-0123-y. Epub 2006 Sep 1. PMID: 16947010.
33. Westwood TD, Hogan C, Julyan PJ, Coutts G, Bonington S, Carrington B, Taylor B, Khoo S, Bonington A. Utility of FDG-PETCT and magnetic resonance spectroscopy in differentiating between cerebral lymphoma and non-malignant CNS lesions in HIV-infected patients. Eur J Radiol. 2013 Aug;82(8):e374-9. doi: 10.1016/j.ejrad.2013.03.008. Epub 2013 Apr 8. PMID: 23578921.
34. Achappa B, Mahalingam S, Shamir AR, Krishnan UB, Ramapuram JT, Rao S, et al. Clinical spectrum and outcomes for toxoplasma encephalitis among AIDS patients before and during the era of anti-retroviral therapy in Mangalore, India. J Clin Diagn Res. 2011 Nov;5(7):1397-1401. doi:10.7860/JCDR/2011/.1671.
35. Abdel Razek AA, Watcharakorn A, Castillo M. Parasitic diseases of the central nervous system. Neuroimaging Clin N Am. 2011 Nov;21(4):815-41, viii. doi: 10.1016/j.nic.2011.07.005. Epub 2011 Sep 3. PMID: 22032501.
36. Levy RM, Mills CM, Posin JP, Moore SG, Rosenblum ML, Bredesen DE. The efficacy and clinical impact of brain imaging in neurologically symptomatic AIDS patients: a prospective CT/MRI study. J Acquir Immune Defic Syndr (1988). 1990;3(5):461-71. PMID: 2324943.
37. Ciricillo SF, Rosenblum ML. Use of CT and MR imaging to distinguish intracranial lesions and to define the need for biopsy in AIDS patients. J Neurosurg. 1990 Nov;73(5):720-4. doi: 10.3171/jns.1990.73.5.0720. PMID: 2213162.
38. Kumar GG, Mahadevan A, Guruprasad AS, Kovoor JM, Satishchandra P, Nath A, Ranga U, Shankar SK. Eccentric target sign in cerebral toxoplasmosis: neuropathological correlate to the imaging feature. J Magn Reson Imaging. 2010 Jun;31(6):1469-72. doi: 10.1002/jmri.22192. PMID: 20512900; PMCID: PMC2908244.
39. Mahadevan A, Ramalingaiah AH, Parthasarathy S, Nath A, Ranga U, Krishna SS. Neuropathological correlate of the “concentric target sign” in MRI of HIV-associated cerebral toxoplasmosis. J Magn Reson Imaging. 2013 Aug;38(2):488-95. doi: 10.1002/jmri.24036. Epub 2013 Feb 25. PMID: 23440973; PMCID: PMC4442780.
40. Gupta RK, Jobanputra KJ, Yadav A. MR spectroscopy in brain infections. Neuroimaging Clin N Am. 2013 Aug;23(3):475-98. doi: 10.1016/j.nic.2013.03.004. Epub 2013 Jun 13. PMID: 23928201.
41. Ramsey RG, Gean AD. Neuroimaging of AIDS. I. Central nervous system toxoplasmosis. Neuroimaging Clin N Am. 1997 May;7(2):171-86. PMID: 9113684.
42. Chong-Han CH, Cortez SC, Tung GA. Diffusion-weighted MRI of cerebral toxoplasma abscess. AJR Am J Roentgenol. 2003 Dec;181(6):1711-4. doi: 10.2214/ajr.181.6.1811711. PMID: 14627601.
43. Camacho DL, Smith JK, Castillo M. Differentiation of toxoplasmosis and lymphoma in AIDS patients by using apparent diffusion coefficients. AJNR Am J Neuroradiol. 2003 Apr;24(4):633-7. PMID: 12695194; PMCID: PMC8148695.
44. Ernst TM, Chang L, Witt MD, Aronow HA, Cornford ME, Walot I, Goldberg MA. Cerebral toxoplasmosis and lymphoma in AIDS: perfusion MR imaging experience in 13 patients. Radiology. 1998 Sep;208(3):663-9. doi: 10.1148/radiology.208.3.9722843. PMID: 9722843.
45. Chang L, Miller BL, McBride D, Cornford M, Oropilla G, Buchthal S, Chiang F, Aronow H, Beck CK, Ernst T. Brain lesions in patients with AIDS: H-1 MR spectroscopy. Radiology. 1995 Nov;197(2):525-31. doi: 10.1148/radiology.197.2.7480706. Erratum in: Radiology 1996 Feb;198(2):586. PMID: 7480706.
46. Marcus C, Feizi P, Hogg J, Summerfield H, Castellani R, Sriwastava S, Marano GD. Imaging in Differentiating Cerebral Toxoplasmosis and Primary CNS Lymphoma With Special Focus on FDG PET/CT. AJR Am J Roentgenol. 2021 Jan;216(1):157-164. doi: 10.2214/AJR.19.22629. Epub 2020 Oct 28. PMID: 33112669.
47. Vyas R, Ebright JR. Toxoplasmosis of the spinal cord in a patient with AIDS: case report and review. Clin Infect Dis. 1996 Nov;23(5):1061-5. doi: 10.1093/clinids/23.5.1061. PMID: 8922803.
48. Rodríguez C, Martínez E, Bolívar G, Sánchez S, Carrascal E. Toxoplasmosis of the spinal cord in an immunocompromised patient: case report and review of the literature. Colomb Med (Cali). 2013 Dec 31;44(4):232-5. PMID: 24892240; PMCID: PMC4001992.
49. Miyoshi IC, de Toledo AHN, Pereira FV, Villarinho LL, Dalaqua M, de Ávila Duarte J, Reis F. Infectious Myelitis. Semin Ultrasound CT MR. 2023 Oct;44(5):424-435. doi: 10.1053/j.sult.2023.03.015. Epub 2023 Apr 5. PMID: 37555684.
50. Johnson T, Nath A. Immune reconstitution inflammatory syndrome and the central nervous system. Curr Opin Neurol. 2011 Jun;24(3):284-90. doi: 10.1097/WCO.0b013e328346be57. PMID: 21499099.
51. Lawn SD. Immune reconstitution disease associated with parasitic infections following initiation of antiretroviral therapy. Curr Opin Infect Dis. 2007 Oct;20(5):482-8. doi: 10.1097/QCO.0b013e3282a6463d. PMID: 17762781.
52. Martin-Blondel G, Alvarez M, Delobel P, Uro-Coste E, Cuzin L, Cuvinciuc V, Fillaux J, Massip P, Marchou B. Toxoplasmic encephalitis IRIS in HIV-infected patients: a case series and review of the literature. J Neurol Neurosurg Psychiatry. 2011 Jun;82(6):691-3. doi: 10.1136/jnnp.2009.199919. Epub 2010 Jul 26. PMID: 20660912.
53. Pfeffer G, Prout A, Hooge J, Maguire J. Biopsy-proven immune reconstitution syndrome in a patient with AIDS and cerebral toxoplasmosis. Neurology. 2009 Jul 28;73(4):321-2. doi: 10.1212/WNL.0b013e3181af788e. PMID: 19636053.
54. Post MJ, Thurnher MM, Clifford DB, Nath A, Gonzalez RG, Gupta RK, Post KK. CNS-immune reconstitution inflammatory syndrome in the setting of HIV infection, part 2: discussion of neuro-immune reconstitution inflammatory syndrome with and without other pathogens. AJNR Am J Neuroradiol. 2013 Jul;34(7):1308-18. doi: 10.3174/ajnr.A3184. Epub 2012 Jul 12. PMID: 22790252; PMCID: PMC4905746.
55. Ramachandran R, Muniyandi M, Iyer V, Sripriya T, Priya B, Govindarajan TG. Dilemmas in the diagnosis and treatment of intracranial tuberculomas. J Neurol Sci. 2017 Oct 15;381:256-264. doi: 10.1016/j.jns.2017.08.3258. Epub 2017 Sep 1. PMID: 28991694.
56. Garg RK. Tuberculosis of the central nervous system. Postgrad Med J. 1999 Mar;75(881):133-40. doi: 10.1136/pgmj.75.881.133. PMID: 10448488; PMCID: PMC1741157.
57. Prakash M, Johnny JC. Intra cranial complications of tuberculous otitis media. J Pharm Bioallied Sci. 2015 Apr;7(Suppl 1):S51-4. doi: 10.4103/0975-7406.155795. PMID: 26015748; PMCID: PMC4439708.
58. Ripamonti D, Barbò R, Rizzi M, Finazzi MG, Ravasio L, Bonaldi G, Suter F. New times for an old disease: intracranial mass lesions caused by Mycobacterium tuberculosis in 5 HIV-negative African immigrants. Clin Infect Dis. 2004 Sep 1;39(5):e35-45. doi: 10.1086/422876. Epub 2004 Aug 11. PMID: 15356800.
59. Hahn RC, Hagen F, Mendes RP, Burger E, Nery AF, Siqueira NP, Guevara A, Rodrigues AM, de Camargo ZP. Paracoccidioidomycosis: Current Status and Future Trends. Clin Microbiol Rev. 2022 Dec 21;35(4):e0023321. doi: 10.1128/cmr.00233-21. Epub 2022 Sep 8. PMID: 36074014; PMCID: PMC9769695.
60. Marques SA. Paracoccidioidomycosis. Clin Dermatol. 2012 Nov-Dec;30(6):610-5. doi: 10.1016/j.clindermatol.2012.01.006. PMID: 23068148.
61. Rodrigues AM, Hagen F, Puccia R, Hahn RC, de Camargo ZP. Paracoccidioides and Paracoccidioidomycosis in the 21st Century. Mycopathologia. Apr 2023;188(1-2):129-133. doi:10.1007/s11046-022-00704-y.
62. Rosa Júnior M, Baldon IV, Amorim AFC, Fonseca APA, Volpato R, Lourenço RB, Baptista RM, de Mello RAF, Peçanha P, Falqueto A. Imaging paracoccidioidomycosis: A pictorial review from head to toe. Eur J Radiol. 2018 Jun;103:147-162. doi: 10.1016/j.ejrad.2018.03.026. Epub 2018 Mar 31. PMID: 29685479.
63. Pedroso VS, Vilela Mde C, Pedroso ER, Teixeira AL. Paracoccidioidomicose com comprometimento do sistema nervoso central: revisão sistemática da literatura [Paracoccidioidomycosis compromising the central nervous system: a systematic review of the literature]. Rev Soc Bras Med Trop. 2009 Nov-Dec;42(6):691-7. Portuguese. doi: 10.1590/s0037-86822009000600016. PMID: 20209357.
64. de Almeida SM, Queiroz-Telles F, Teive HA, Ribeiro CE, Werneck LC. Central nervous system paracoccidioidomycosis: clinical features and laboratorial findings. J Infect. 2004 Feb;48(2):193-8. doi: 10.1016/j.jinf.2003.08.012. PMID: 14720496.
65. Reis F, Collier PP, Souza TF, Lopes GP, Bronzatto E, Silva Junior NA, Pereira RM, Appenzeller S. Neuroparacoccidioidomycosis (NPCM): magnetic resonance imaging (MRI) findings. Mycopathologia. 2013 Feb;175(1-2):181-6. doi: 10.1007/s11046-012-9607-y. Epub 2012 Dec 11. PMID: 23229616.
66. Duarte SBL, Oshima MM, Mesquita JVDA, do Nascimento FBP, de Azevedo PC, Reis F. Magnetic resonance imaging findings in central nervous system cryptococcosis: comparison between immunocompetent and immunocompromised patients. Radiol Bras. 2017 Nov-Dec;50(6):359-365. doi: 10.1590/0100-3984.2016.0017. PMID: 29307925; PMCID: PMC5746879.
67. Maziarz EK, Perfect JR. Cryptococcosis. Infect Dis Clin North Am. 2016 Mar;30(1):179-206. doi: 10.1016/j.idc.2015.10.006. PMID: 26897067; PMCID: PMC5808417.
68. Mathews VP, Alo PL, Glass JD, Kumar AJ, McArthur JC. AIDS-related CNS cryptococcosis: radiologic-pathologic correlation. AJNR Am J Neuroradiol. 1992 Sep-Oct;13(5):1477-86. PMID: 1414845; PMCID: PMC8335225.
69. Xia S, Li X, Li H. Imaging characterization of cryptococcal meningoencephalitis. Radiol Infect Dis. 2016;3(4):187-191. doi:10.1016/j.jrid.2016.05.003.
70. Katchanov J, Branding G, Jefferys L, Arastéh K, Stocker H, Siebert E. Neuroimaging of HIV-associated cryptococcal meningitis: comparison of magnetic resonance imaging findings in patients with and without immune reconstitution. Int J STD AIDS. 2016 Feb;27(2):110-7. doi: 10.1177/0956462415574633. Epub 2015 Feb 18. PMID: 25693580.
1. Department of Radiology and Oncology, Universidade Estadual de Campinas, Campinas, SP, Brazil
2. Department of Radiology, Réseau Hospitalier Neuchâtelois, Neuchâtel, Switzerland
3. Hospital do Coração, São Paulo, SP, Brazil
4. Hospital Beneficência Portuguesa, São Paulo, SP, Brazil
5. Department of Orthopedics and Rheumatology, Universidade Estadual de Campinas, Campinas, SP, Brazil
6. Department of Radiology and Diagnostic Imaging, Hospital de Clínicas de Porto Alegre (HCPA), Porto Alegre, RS, Brazil
a.
https://orcid.org/0009-0007-4124-4262b.
https://orcid.org/0009-0008-9740-8411c.
https://orcid.org/0000-0001-9360-0547d.
https://orcid.org/0000-0002-0324-8568e.
https://orcid.org/0000-0003-2944-9947f.
https://orcid.org/0009-0003-9949-1208g.
https://orcid.org/0000-0001-5075-4474h.
https://orcid.org/0000-0003-4973-2889i.
https://orcid.org/0000-0003-2256-4379Corresponding:Pedro Henrique Abreu Tiradentes
UNICAMP - Universidade Estadual de Campinas, Rua Vital Brasil, 251, Cidade Universitária Zeferino Vaz, Campinas, SP, Brazil, 13083-888.
Email:
phtiradentes@hotmail.comEditor in charge: Dr. Valdair Francisco Muglia
Received in
September 18 2025.
Accepted em
November 21 2025.
Publish in
June 23 2026.

 |
|



 PDF English
PDF English
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket