
 |
|
André Vaza; Vinícius Cardoso Serrab
DOI: 10.1590/0100-3984.2025.0047
e20250047
Publish in: July 25 2025
We would like to congratulate Reifegerste et al.(1) for their excellent review of the literature on imaging findings following sternotomy, published in Radiologia Brasileira. The article offers a comprehensive overview of the expected postoperative findings and complications following thoracic surgery. To address this clinically relevant and frequently encountered scenario, the use of a structured report would significantly enhance clarity and consistency, facilitating interdisciplinary communication and enabling improved clinical decision-making and follow-up.
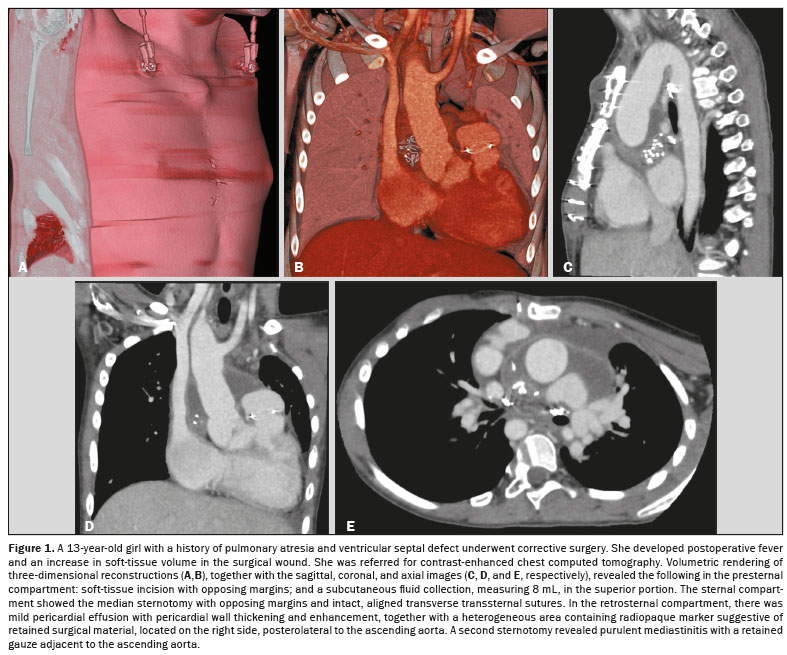
We propose the use of a structured template that categorizes postoperative findings into three anatomical compartments(2–4): presternal, sternal, and retrosternal. Each compartment may present with specific findings as follows (illustrative case in Figure 1).
a) Closure:
– Soft tissue incision with opposing margins.
– Soft tissue dehiscence.
b) Content:
– Mild adipose tissue stranding related to recent manipulation/superficial sternal wound infection.
– Superficial/deep subcutaneous fluid collection, measuring [ ] mL.
c) Devices:
– Tubular drain with superficial/deep subcutaneous tip.
– Vacuum-assisted soft tissue closure.
a) Closure:
– Median sternotomy with opposing margins.
– Delayed sternal closure with fragments separated by [ ] mm.
– Sternal dehiscence with bone fragments separated by [ ] mm at the upper, middle, or lower third.
b) Content:
– Discrete irregularity of the sternal margins suggestive of reparative bone changes.
– Osteolytic lesions at the sternal margins suggestive of osteomyelitis.
c) Devices:
– Intact and aligned transverse peristernal/transsternal/figure-of-eight/Robicsek sutures/plates and screws.
– Transverse peristernal/transsternal/figure-of-eight/Ro- bicsek sutures/plates and screws with fracture/displacement in the upper/middle/lower third.
a) Content:
– Mild mediastinal adipose tissue stranding consistent with recent postoperative changes.
– Persistent/progressive mediastinal adipose tissue stranding suggestive of deep sternal wound infection/mediastinitis.
– Anterior/superior/anterosuperior mediastinal fluid collection defined as mild (< 10 mm), moderate (10–20 mm), or severe (> 20 mm).
– Pericardial effusion defined as mild (< 10 mm), moderate (10–20 mm), or severe (> 20 mm).
– Heterogeneous area containing radiopaque marker suggestive of retained surgical material, located in [ ].
b) Devices:
– Mediastinal drainage tube in a retrosternal, paracardiac, retrocardiac, infracardiac, or supracardiac position.
– Retrosternal synthetic membrane-assisted pericardial closure.
– Temporary pacemaker with epicardial leads.
Publish in July 25 2025.

![]()
![]()
![]()


 PDF English
PDF English
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket