
 |
|
Laís Rodrigues Bertochea; Waldinei Mercês Rodriguesb; Caroline von Abel de Sousac; Vitor Maltoni Damasiod; Hélder Jorge Andrade Gomese; Eduardo Vieira Pontef
DOI: 10.1590/0100-3984.2025.0004
e20250004
Publish in: July 8 2025
ABSTRACT
OBJECTIVE: To evaluate the frequency of the typical computed tomography (CT) pattern in individuals with coronavirus 2019 (COVID-19), comparing those who were vaccinated with those who were unvaccinated.
MATERIALS AND METHODS: This was a retrospective study of the medical records of patients with clinical suspicion of COVID-19 between August 2021 and February 2022. The vaccination status was classified as absent/incomplete (0 or 1 dose) or complete (2 or more doses). The pattern seen on the first chest CT was defined as typical, atypical, indeterminate, or normal, the last three patterns being combined to form what was designated the non-typical group.
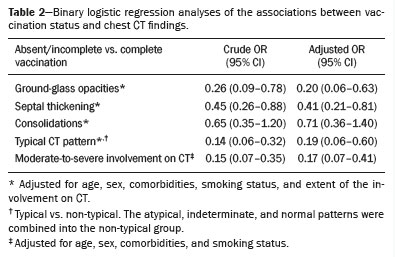
RESULTS: Binary logistic regression analysis showed that individuals with a complete vaccination status were less likely to present with the typical CT pattern than were those with an absent/incomplete vaccination status (adjusted OR = 0.19, 95% CI: 0.06–0.60).
CONCLUSION: This information is important because it demonstrates that the frequency of the CT pattern considered typical of COVID-19 is currently lower than it was before the vaccines became available. Therefore, the typical CT pattern is no longer expected.
Keywords: Tomography, X-ray computed; Thorax; COVID-19; Vaccines.
RESUMO
OBJETIVO: Avaliar a frequência do padrão da tomografia computadorizada (TC) de indivíduos com COVID-19, comparando os vacinados com os não vacinados.
MATERIAIS E MÉTODOS: Estudo retrospectivo em que foram selecionados prontuários de pacientes com suspeita clínica de COVID-19, entre agosto/2021 e fevereiro/2022. Os pacientes foram classificados, conforme a situação vacinal, em vacinação ausente/incompleta (0 ou 1 dose) ou vacinação completa (2 ou mais doses). A primeira TC de tórax do paciente foi classificada como típica, atípica, indeterminada ou normal, agrupando-se os padrões atípico, indeterminado ou normal em não típico.
RESULTADOS: A análise de regressão logística binária mostrou que indivíduos com vacinação completa tinham menor probabilidade de apresentar um padrão típico na TC de tórax em comparação com indivíduos com vacinação ausente/incompleta (OR ajustado: 0,19, IC 95%: 0,06–0,60).
CONCLUSÃO: Esta informação é importante porque demonstra que, atualmente, a frequência de padrões tomográficos típicos é menor e, portanto, o padrão tomográfico típico não é mais esperado como foi visto previamente antes da vacinação.
Palavras-chave: Tomografia computadorizada por raios X; Tórax; COVID-19; Vacinas.
INTRODUCTION
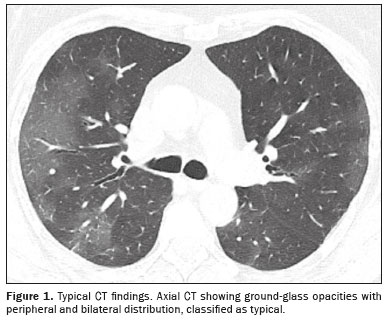
Some individuals infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) develop acute respiratory failure. During the coronavirus disease 2019 (COVID-19) pandemic, the Radiological Society of North America created a guideline that established the radiological pattern considered typical of COVID-19 and identified three other patterns to classify suspicious cases, designated the indeterminate, atypical, and normal patterns(1). The characteristics on chest computed tomography (CT) considered typical of COVID-19 were multiple, bilateral subsegmental or lobular consolidations or bilateral ground-glass opacities(2,3). In the period before the vaccines against COVID-19 became available, the CT pattern was important to differentiate COVID-19 from other causes of acute respiratory failure that could affect individuals infected with SARS-CoV-2, such as venous thromboembolism, decompensated heart failure, and bacterial pneumonia.
The development and administration of COVID-19 vaccines have changed the clinical and epidemiological scenario. The incidence of COVID-19 reduced rapidly; if diagnosed with the disease, vaccinated individuals had better clinical outcomes and less extensive lung involvement on chest CT(4–8). However, little is known about the effect of the vaccine on the chest CT pattern in individuals with COVID-19. We hypothesized that the CT pattern considered typical of COVID-19 would be less common in vaccinated individuals than in those who were unvaccinated. Clarifying this issue is important because the absence of the typical CT pattern might not be sufficient to exclude the diagnosis of COVID-19 in vaccinated individuals who present hypoxemia during a SARS-CoV-2 infection. Therefore, the objective of this study was to determine whether, among individuals with COVID-19, the frequency of the typical CT pattern differed between vaccinated and unvaccinated individuals.
MATERIALS AND METHODS
This was a retrospective study conducted in the city of Jundiaí, SP, Brazil, a municipality with 400,000 inhabitants. We reviewed the medical records of all individuals with clinical suspicion of COVID-19 who presented to the emergency room of a public hospital between August 2021 and February 2022. We selected the records of individuals ≥ 18 years of age with SARS-CoV-2 infection confirmed by reverse transcription-polymerase chain reaction (RT-PCR). Individuals in whom the CT image was of poor quality were excluded, as were those in whom the CT findings were consistent with an expansile process or fibrotic changes. The study was approved by the local institutional review board (Reference no. 5.711.929). Because the data were collected retrospectively, the requirement for informed consent was waived.
Data retrieve
During the COVID-19 pandemic, the hospital protocol established in the city stated that individuals who presented to health care facilities with hypoxemia should undergo RT-PCR or an antigen test for SARS-CoV-2, as well as a chest CT scan, and be hospitalized. The electronic medical records of all such individuals were screened for this study. This study criteria for a diagnosis of COVID-19 were peripheral oxygen saturation below 94% on hospital admission and positivity for SARS-CoV-2 infection on one of the confirmatory tests. The electronic medical records included patient data collected systematically for epidemiological study by the Jundiaí Municipal Health Department: vaccination status; comorbidities (asthma, chronic obstructive pulmonary disease, congestive heart failure, hypertension, diabetes mellitus, and chronic renal failure); and smoking history. All of those data were retrieved for the purposes of this study.
Vaccination status and analysis of chest CT
At the time of hospital admission, a health professional systematically reviewed the vaccination card of each individual to record the number of doses of COVID-19 vaccine received. This information was retrieved by researchers to classify the vaccination status of individuals included in the study as absent/incomplete (zero or one dose) or complete (two or more doses).
For each individual, the first chest CT scan was retrieved and evaluated by three radiologists who were blinded to the vaccination status. The images were classified by consensus as typical, atypical, indeterminate, or normal according to the Radiological Society of North America Expert Consensus Statement(1). For statistical analysis purposes, we combined the atypical, indeterminate, and normal patterns into a group designated the non-typical group. Subsequently, we quantified the extent of lung involvement on CT. Each segment of each lung lobe was scored for the extent of involvement(4): 1 point if 0–5%; 2 points if 5–25%; 3 points if 25–50%; 4 points if 50–75%; and 5 points if 75–100%. Those scores were summed to establish a final score, which was used in order to classify the overall extent of lung involvement as mild (≤ 8 points), moderate (9–15 points), or severe (> 15 points).
Statistical analysis
To calculate the sample size, the alpha was set at 0.05 and the power was set at 80%. We estimated the minimum sample size to be 62 individuals in each group considering that a CT pattern typical of COVID-19 would be present in 70% of individuals with a complete vaccination status and in 90% of those with an absent/incomplete vaccination status(9). We applied the chi-square and Mann-Whitney tests to compare categorical and continuous variables, respectively. We used binary logistic regression analysis to measure the association between vaccination status (independent variable) and the CT pattern (dependent variable). We adjusted the analyses for age, sex, comorbidities, smoking status, and the extent of lung involvement on chest CT because these covariates could affect the relationship between the dependent and independent variables(10). The method of data entry into the regression model was the backward likelihood ratio approach. The level of significance required for a given variable to remain in the model was 0.10. We used the Hosmer-Lemeshow test to measure goodness-of-fit, as well as the tolerance test and variance inflation factor to measure collinearity. The data fitted the model well (Hosmer-Lemeshow test > 0.05), an we observed no collinearity (tolerance test > 0.10; variance inflation factor < 10).
RESULTS
During the study period, 783 individuals presented with peripheral oxygen saturation less than 94%, and 274 of those individuals tested positive for SARS-CoV-2 infection by RT-PCR or antigen test. Of those 274 individuals, 58 were excluded: 27 because they did not undergo chest CT; 22 because their medical records did not contain information about their vaccination status; and nine for various other reasons. Therefore, the final sample comprised 216 individuals diagnosed with COVID-19.
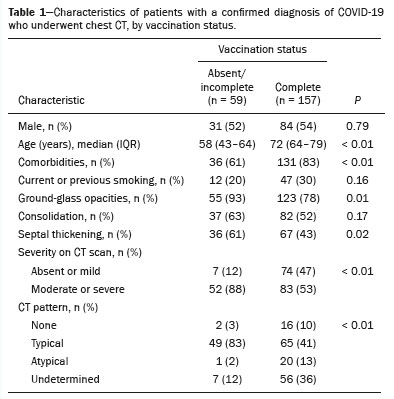
Among the 216 individuals evaluated, 157 (73%) were fully vaccinated and 59 (27%) had an absent/incomplete vaccination status. Of those with a complete vaccination status, 84 (54%) were men, compared with 31 (52%) of those with an absent/incomplete vaccination status (p = 0.79). The median age in the two groups was 72 years (range, 64–79 years) and 58 years (range, 43–64 years), respectively (p < 0.01). Comorbidities were more common among individuals with a complete vaccination status than among those without, being identified in 131 (83%) and 36 (61%) of the individuals, respectively (p < 0.01).
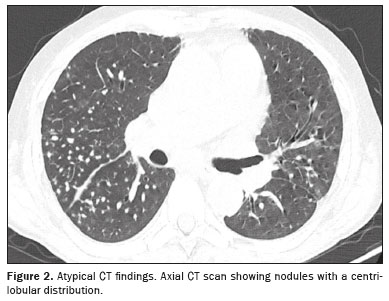
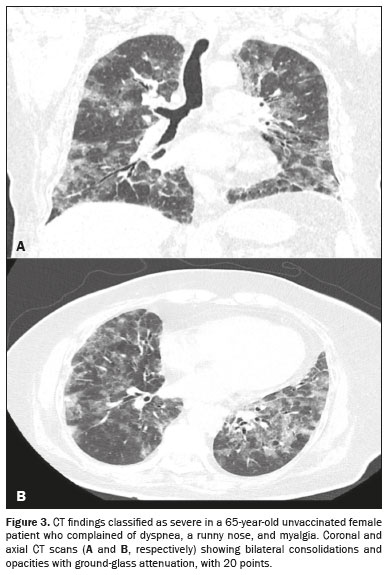
Typical CT pattern was observed in only 41% of the individuals with a complete vaccination status, compared with 83% of the individuals with an absent/incomplete vaccination status (p < 0.01) (Table 1). The binary logistic regression analysis showed that having a complete vaccination status reduced the chance of presenting the typical pattern on CT scan by 81% compared with having an absent/incomplete vaccination status (adjusted OR = 0.19, 95% CI: 0.06–0.60) (Table 2). Typical and atypical CT findings are illustrated in Figures 1 and 2, respectively. Ground-glass opacities and septal thickening were less common among individuals with a complete vaccination status than among those with an absent/incomplete vaccination status (adjusted OR = 0.20, 95% CI: 0.06–0.63 and adjusted OR = 0.41, 95% CI: 0.21–0.81, respectively), whereas there was no association between consolidations and vaccination status (adjusted OR = 0.71, 95% CI: 0.36–1.40). Additionally, individuals with a complete vaccination status were less prone to have moderate/severe lung involvement on chest CT (adjusted OR = 0.17, 95% CI: 0.07–0.41). Figure 3 illustrates CT findings classified as severe.
Received in
January 8 2025.
Accepted em
March 28 2025.
Publish in
July 8 2025.

![]()
![]()
![]()


 PDF English
PDF English
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket