
 |
|
Francisco Carlos da Silva1,a; Gabriel Antonio Nascentes2,b; Antonio Carlos Oliveira Meneses3,c; Dalmo Correia Filho4,d
ABSTRACT
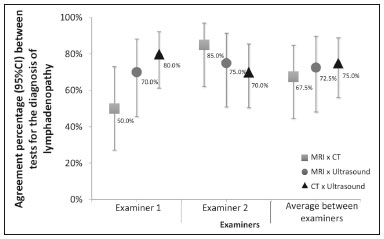
OBJECTIVE: To assess the percent agreement between diagnostic imaging modalities for the evaluation of lymphadenopathies in HIV-infected/AIDS patients. MATERIALS AND METHODS: This was an open, comparative, prospective study of diagnostic imaging methods for lymphadenopathy evaluation. We evaluated 30 patients (19 men and 11 women). All underwent ultrasound and computed tomography (CT). Twenty of the patients also underwent magnetic resonance imaging (MRI). We determined the percent agreement between two examiners using the various imaging methods to evaluate lymphadenopathies. RESULTS: CT had the highest percent agreement, at 93.3%, with a kappa coefficient of 0.85, corresponding to 28 of the 30 examinations. When we compared the percent agreement between the two examiners and between CT and ultrasound, examiner 1 had an observed rate of 80.0%, with a kappa of 0.49, corresponding to 24 of the 30 examinations, whereas examiner 2 had a rate of 70.0%, with a kappa of 0.31, corresponding to 21 of the 30 examinations. Between MRI and CT, the percent agreement for examiner 1 was 50.0%, with a kappa of −0.18, corresponding to 10 of the 20 examinations, whereas that for examiner 2 was 85.0%, with a kappa of 0.69, corresponding to 17 of the 20 examinations. For MRI and ultrasound, examiner 1 had a percent agreement of 70.0%, with a kappa of 0.20, corresponding to 14 of the 20 examinations, and examiner 2 had a percent agreement of 75.0%, with a kappa of 0.38, corresponding to 15 of the 20 examinations. CONCLUSION: This study indicates that intermethod agreement is highly dependent on the way in which the research is conducted, rather than on the level of experience of the examiner.
Keywords: HIV; Acquired immunodeficiency syndrome; Lymphadenopathy; Ultrasonography; Tomography, X-ray computed; Magnetic resonance imaging..
RESUMO
OBJETIVO: Avaliar a porcentagem de concordância entre métodos de diagnóstico por imagem na avaliação de linfonodomegalias em pacientes HIV(+)/AIDS. MATERIAIS E MÉTODOS: Foi realizado estudo aberto, comparativo e prospectivo dos métodos de diagnóstico por imagem na avaliação de linfonodomegalias. Foram avaliados 30 pacientes (19 homens e 11 mulheres). Todos foram submetidos a ultrassonografia e tomografia computadorizada (TC) e 20 também foram submetidos a ressonância magnética (RM). Foi determinado o grau de concordância entre dois examinadores usando-se métodos de diagnóstico por imagem. RESULTADOS: A TC obteve o maior grau de concordância, com taxa de 28/30 (93,3%) e coeficiente kappa de 0,85. Quando comparado o grau de concordância para linfonodomegalias entre dois examinadores e entre TC e ultrassonografia, o examinador 1 teve taxa de 24/30 (80,0%) e kappa de 0,49, e o examinador 2 teve taxa de 21/30 (70,0%) e kappa de 0,31. Entre RM e TC, o examinador 1 teve taxa de 10/20 (50,0%) e kappa de –0,18, e o examinador 2 teve taxa de 17/20 (85,0%) e kappa de 0,69. Entre RM e ultrassonografia, o examinador 1 teve taxa de 14/20 (70,0%) e kappa de 0,20, e o examinador 2 teve taxa de 15/20 (75,0%) e kappa de 0,38. CONCLUSÃO: Este estudo indica que a concordância entre métodos depende fortemente da forma como a pesquisa é conduzida e não da capacidade do examinador.
Palavras-chave: HIV; Síndrome da imunodeficiência adquirida; Linfadenopatia; Ultrassonografia; Tomografia computadorizada; Ressonância magnética.
INTRODUCTION
Acquired immunodeficiency syndrome (AIDS) is caused by infection with HIV, a retrovirus that exhibits tropism for cells of the immune system and central nervous system, affecting CD4+ T lymphocytes in particular(1,2). HIV, which belongs to the genus Lentivirus, has a molecular structure comprising 15 proteins encoded by two RNA molecules(3).
Worldwide, there are nearly 37.6 million people living with HIV infection, and 2.1 million new cases were reported in 2015; a significant number of those occurred in African countries. In Latin America, a total of 2 million cases have been reported; more than a third of those occurred in Brazil(4). Recent data suggest that the HIV epidemic will end by 2030, given that reductions in the numbers of new cases exceed 50% in some countries(5). In Brazil, there is currently a clear trend toward an increase in the incidence of AIDS among young people, particularly among women 13–19 years of age, which has reduced the male:female ratio, the number of AIDS cases per 100,000 population being 2.0 among males and 1.6 among females(4).
Superficial and deep lymphadenopathies are among the main clinical manifestations of early- and late-stage AIDS; the latter often featuring inflammatory, infectious, or neoplastic comorbidities(6,7). Physiologically, lymph nodes have a diameter of 1.0–1.5 cm, feature an oval shape, have predominantly central vascularization, and are located in surface or cavitary chains(6).
In HIV-infected/AIDS patients, lymphadenopathies appear early in the infectious process, as a component of disease progression, and can occur in response to opportunistic infectious agents (e.g., bacteria, fungi, and viruses) or malignant degeneration (e.g., lymphoma and sarcoma)(8). The most common causes of lymphadenopathy in HIV-infected/AIDS patients are diseases related to infection with bacteria, mycobacteria (e.g., tuberculosis), fungi (e.g., histoplasmosis, cryptococcosis, and paracoccidioidomycosis), or viruses (e.g., cytomegalovirus infection and herpes virus infection), as well as those related to colonization by parasites (e.g., toxoplasmosis and leishmaniasis). Such lymphadenopathies are often generalized and minimally painful, mainly affecting the cervical and retroperitoneal lymph nodes. Patients with tuberculosis nearly always originate from endemic areas and exhibit some degree of pulmonary impairment(9).
Lymphoproliferative disorders also comprise part of the spectrum of lymphadenopathies in HIV-infected/AIDS patients. Among such disorders, the most common histological types are B-cell lymphomas, Hodgkin lymphoma, and Burkitt lymphoma(10–12).
Imaging modalities are important tools in the diagnosis of lymphadenopathies. Several imaging methods can be used to characterize the condition as inflammatory (infectious or not) or related to malignancy (primary or metastatic).
Because of its ease of use, accessibility, and low cost, ultrasound examination is indicated for the evaluation of peripheral lymphadenopathies. However, computed tomography (CT) and magnetic resonance imaging (MRI) are the best methods for evaluating cavitary lymphadenopathies(13–16).
CT can clearly characterize lymph nodes, distinguish them from neighboring structures, and suggest an inflammatory, infectious, or malignant etiology. The disadvantage of CT is the use of iodinated contrast, which is contraindicated in many patients (e.g., those with diabetes, kidney failure, or allergies).
The efficacy of MRI is similar and, in some cases, superior to that of CT. Therefore, MRI can be used to characterize the extent of lesions and distinguish lymph nodes from lesions, as well as to determine the number, volume, and appearance of lesions(7).
The objective of the present study was to evaluate the level of agreement between diagnostic imaging methods (ultrasound, CT, and MRI) for the evaluation of lymphadenopathies. Specifically, we compared the three methods in terms of their efficacy in evaluating superficial and deep lymphadenopathies in HIV-infected/AIDS patients.
MATERIALS AND METHODS
This was a prospective, cross-sectional, open, comparative study of the diagnostic imaging methods available for the evaluation of lymphadenopathies at the Universidade Federal do Triângulo Mineiro (UFTM)—Federal University of Triângulo Mineiro—between February 2012 and September 2013. We also compared the results with those of the gold standard methods (histopathological analysis and culture). The study was approved by the UFTM Research Ethics Committee (Protocol No. 2327).
We recruited HIV-infected/AIDS patients with a fever of unclear etiology, abdominal pain, wasting syndrome, superficial or cavitary inflammatory lymphadenopathies, or acute abdominal inflammation who were treated in the Department of Infectious and Parasitic Diseases, Clinical Ward, or Emergency Room of the UFTM Clinical Hospital during the period under study. We also included patients seen at the Infectious and Parasitic Diseases Outpatient Clinic of the UFTM Clinical Hospital.
This final sample comprised 30 patients (19 males and 11 females). The mean age was 42 years (range, 20–61 years). These demographic characteristics are consistent with those of many published studies on this topic(17–19). All participating patients gave written informed consent.
Diagnostic imaging examinations (ultrasound, CT, and MRI) were performed by two different examiners, both of whom were blinded to the serological status of the patients. Each examiner issued reports independently (without any knowledge of the reports issued by the other examiner). All imaging examinations were performed in the Imaging Department of the UFTM Clinical Hospital.
Ultrasound evaluation
All of the patients underwent ultrasound evaluation. We employed an Accuvix V10 ultrasound system (Samsung Medison, Seoul, South Korea), using a 5–12 MHz linear probe to study surface lymphadenopathies and a 3–5 MHz convex probe to study cavitary lymphadenopathies. For the purposes of this study, the following examination protocol was established: analysis of anatomical features (size, shape, echotexture, topography, number, presence of calcifications, central necrosis, distribution of vascularization, adherence to deep layers, and presence of hemorrhage); and analysis of characteristics suggestive of malignancy (e.g., anteroposterior diameter greater than the longitudinal diameter, invasion of surrounding tissues, and loss of corticomedullary differentiation). Color Doppler analysis was also used.
CT evaluation
All of the patients underwent CT evaluation. In all CT examinations, we used a 64-channel multislice spiral CT scanner (Aquilion; Toshiba Corporation, Tokyo, Japan) and particular attention was given to lymphadenopathies detected previously by ultrasound. All patients except those with a history of hypersensitivity to iodinated agents received intravenous contrast via peripheral venipuncture in an upper limb. Patients were exposed to a minimal radiation dose because all slices were obtained simultaneously in a fraction of 10–15 s. During the CT scans, in addition to the aspects evaluated via ultrasound, we evaluated the presence or absence of contrast uptake and peripheral enhancement.
MRI evaluation
For economic reasons, only 20 patients underwent MRI scans for comparison with the ultrasound and CT images. All of those patients underwent MRI examination in a 1.5 T scanner (Avanto; Siemens AG, Berlin, Germany). The MRI scans allowed better evaluation of cavitary lymphadenopathies and included additional elements, such as multiplanar reformatting, as well as more detailed analyses of anatomical, inflammatory, and neoplastic aspects. Gadolinium contrast was used.
The descriptive CT and MRI findings were compared with the ultrasound data in terms of the levels of agreement and disagreement regarding the parameters related to lymphadenopathy (size, number, shape, location, necrosis, calcifications, distinction from surrounding tissues, vascularization, corticomedullary differentiation, adherence to deep layers, and hepatosplenomegaly).
Statistical analysis
The statistical analysis of categorical data was conducted using appropriate tests. Possible associations between risk factors and the presence of lymphadenopathy were assessed by using the chi-square test with Yates correction, and kappa coefficients were calculated with 95% confidence intervals. The kappa coefficient was used in order to assess agreement between the diagnostic tests, as well as between the examiners. The level of agreement was based on the indices suggested by Landis and Koch, as follows: kappa ≤ 0 = none; 0.01–0.40 = weak; 0.41–0.60 = discreet; 0.61–0.80 = moderate; 0.81–0.99 = substantial; and 1.00 = perfect. Statistical analyses were performed using Statistica software, version 10.0 (Statsoft Inc., Tulsa, OK, USA).
RESULTS
Between February 2012 and September 2013, 81 patients with a confirmed diagnosis of HIV infection/AIDS with fever and lymphadenopathies underwent ultrasound evaluation. The mean age of those patients was 42 years (range, 20–61 years). Of those 81 patients, 30 (11 females and 19 males) were selected to undergo ultrasound and CT scans, 20 of those 30 being selected to undergo MRI as well. The remaining 51 patients were excluded for the following reasons: hospital discharge before the examinations; refusal of admission to the hospital; death before completion of examinations (especially histopathology); or specific constraints regarding each imaging method (e.g., metallic prostheses or artificial pacemakers, for MRI, and allergy to iodine, for CT).
Sixteen patients (53%) underwent fine-needle aspiration biopsy. Among those 16 patients, the results were inconclusive in 14 (87.5%) and lymphoid hyperplasia was detected in two (12.5%). Thirty patients underwent lymph node excision, and the subsequent histopathological study revealed necrosis in one. The following histopathological diagnoses were made: lymphoid hyperplasia, in six patients (20%); tuberculosis, in six (20%); nonspecific chronic inflammation, in four (14%); histoplasmosis, in three (10%); paracoccidioidomycosis, in three (10%); acute suppurative inflammation, in two (7%); Hodgkin lymphoma, in one (3%); B-cell lymphoma, in one (3%); toxoplasmosis, in one (3%); and leishmaniasis, in one (3%). The lymphadenopathies were distributed as follows: in the cervical region, in 25 cases (83%); in the abdominal region, in 18 (60%); in the thoracic region, in three (10%); in the inguinal region, in three (10%); in the axillary region, in three (10%); in the retroperitoneal region, in one (0.3%); in the periaortic region, in one (0.3%); and in the peripancreatic region, in one (0.3%).
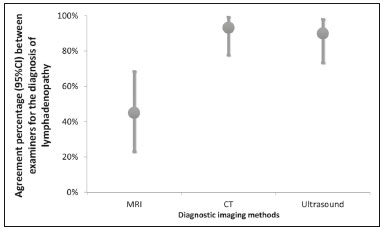
We evaluated the percent agreement (95% CI) between the two examiners in the diagnosis of lymphadenopathies for each of the three diagnostic imaging methods (Figure 1). The highest percent agreement was observed for the CT scans—93.3% (95% CI: 77.9% to 99.2%), with a kappa coefficient of 0.85 (95% CI: 0.65 to 1.00), corresponding to 28 of the 30 examinations.

![]()
![]()
![]()


 PDF English
PDF English
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket