
 |
|
Rodrigo Gomes de Oliveira1,a; Domingos de Morais Filho2,b; Carlos Alberto Engelhorn3,c; Iruena Moraes Kessler4,d; Felipe Coelho Neto5,e
ABSTRACT
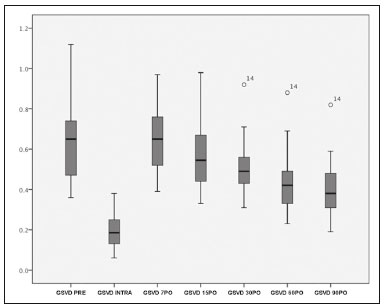
OBJECTIVE: To assess changes in the great saphenous vein (GSV) after foam sclerotherapy for varicose veins. MATERIALS AND METHODS: This was a prospective study of 33 patients who were treated with polidocanol foam sclerotherapy after having had varicose veins with a clinical severity-etiology-anatomy-pathophysiology classification of C4-C6 for three months. The patients were evaluated by ultrasound before, during, and after the procedure (on post-procedure days 7, 15, 30, 60, and 90). The GSV diameter, the rate of venous occlusion, and the rate of reflux elimination were determined. Two patients were excluded for having a history of deep vein thrombosis history, and one was excluded for having bronchial asthma. RESULTS: Thirty patients (26 females and 4 males, with mean age of 62 years) completed the protocol. The mean pre-procedure GSV diameter was 6.0 ± 0.32 mm (range, 3.6-11.2 mm). During the sclerotherapy, the mean GSV diameter was reduced to 1.9 ± 0.15 mm (range, 0.6-3.8 mm). On post-procedure day 7, the mean GSV diameter increased to 6.3 ± 0.28 mm (range, 3.9-9.7 mm). On post-procedure day 90, the mean GSV diameter was 4.0 ± 0.22 mm (range, 1.9-8.2 mm). The rate of GSV reflux was significantly lower in the assessment performed on post-procedure day 90 than in the pre-procedure assessment (p < 0.0028). CONCLUSION: On the basis of our ultrasound analysis, we can conclude that foam sclerotherapy for varicose veins results in a significant reduction in GSV diameter, as well as in the elimination of GSV reflux.
Keywords: Ultrasonography; Varicose veins; Sclerotherapy; Saphenous vein; Venous insufficiency.
RESUMO
OBJETIVO: Avaliar alterações ultrassonográficas na veia safena magna (VSM) após escleroterapia com espuma para varizes. MATERIAIS E MÉTODOS: Estudo prospectivo de 33 pacientes com varizes classificadas como C4-C6 (classificação clinical severity- etiology-anatomy-pathophysiology), durante três meses, submetidos a escleroterapia com espuma de polidocanol. Os pacientes foram acompanhados por ultrassonografia vascular antes, durante e 7, 15, 30, 60 e 90 dias após o procedimento. Avaliaram-se o diâmetro da VSM, a taxa de oclusão venosa e a taxa de abolição do refluxo. Dois indivíduos foram excluídos do estudo por apresentarem história prévia de trombose venosa profunda e um paciente não participou do estudo por asma brônquica. RESULTADOS: Dos 30 pacientes que completaram o protocolo, 26 eram do sexo feminino e 4 eram do sexo masculino, com idade média de 62 anos. O diâmetro da VSM médio pré-operatório foi 6,0 ± 0,32 mm (variação: 3,6-11,2 mm). Na escleroterapia, houve redução do diâmetro médio para 1,9 ± 0,15 mm (variação: 0,6-3,8 mm). Em 7 dias, houve aumento médio do diâmetro da VSM para 6,3 ± 0,28 mm (variação: 3,9-9,7 mm). Em 90 dias, o diâmetro da VSM médio reduziu para 4,0 ± 0,22 mm (variação: 1,9-8,2 mm). O refluxo venoso apresentou redução estatisticamente significante entre o pré-operatório e pós-operatório após 90 dias (p < 0,0028). CONCLUSÃO: Com base em nossa análise ultrassonográfica, podemos concluir que a escleroterapia com espuma para varizes resulta em uma redução significativa do diâmetro da VSM, bem como abolição do refluxo da VSM.
Palavras-chave: Ultrassonografia; Escleroterapia; Varizes; Veia safena; Insuficiência venosa.
INTRODUCTION
The ideal treatment for primary varicose veins in the lower extremities should be minimally invasive, repeated when necessary, and free from significant complications. It should also be effective for eliminating points of reflux and reducing venous hypertension at the extremities, as well as being affordable, providing esthetic improvement, and requiring patients to take little time off from work(1).
The advent of Doppler vascular ultrasound has driven new endovascular treatment methods, such as laser photocoagulation, radiofrequency ablation, and foam sclerotherapy, the last having proven to be an attractive technique, because anesthesia, hospital admission, and post-treatment bed rest are unnecessary(2). The foam is produced by mixing a sclerosing agent with room air and can be used to treat saphenous veins as well as trunk varicose veins and perforating veins, particularly in advanced cases with skin lesions and ulcers(3,4). Doppler vascular ultrasound is indispensable for performing the procedure and for follow up, because it can monitor occlusion of the vein and detect reflux relapses(5).
The objective of this study was to use duplex ultrasound to evaluate changes in the diameter of the great saphenous vein (GSV) and the rate of venous reflux elimination after treatment with polidocanol foam sclerotherapy.
MATERIALS AND METHODS
This was an open prospective study evaluating the impact that polidocanol foam sclerotherapy for chronic venous insufficiency (CVI) has on the diameters of the saphenous veins treated and on the rate of venous occlusion. The study was conducted at a private vascular surgery clinic between February and September of 2009. The study was approved by the institutional ethics committee, and all participating patients gave written informed consent.
The inclusion criteria were being ≥ 18 years of age; having lower-limb CVI classified as clinical stage C4, C5, or C6 according to the clinical severity-etiology-anatomy-pathophysiology (CEAP) classification(6); and proximal, multisegmental, or diffuse reflux in the GSV(7). Patients in whom ultrasound showed acute deep vein thrombosis or deep vein thrombosis that was not recanalized were excluded, as were those with varicose veins unrelated to GSV reflux and those who had previously undergone varicose vein surgery, as well as those with thrombophilia, active neoplasm or cancer under surveillance, lung disease, or peripheral arterial disease (ankle-brachial index < 0.9).
Sclerotherapy technique
The sclerotherapy technique employed in the present study has been described elsewhere(8). The patients underwent treatment of the GSV and of tributary varicose veins. When complete closure of target veins was not achieved, additional sessions were conducted until complete closure was achieved. Additional sessions, with one or more punctures, were conducted, as necessary (on a case-by-case basis), at 7-day intervals. In all cases, foam was produced by mixing 3% polidocanol with room air, at a proportion of 1:4, and the total volume of foam per session did not exceed 10 mL(9).
After the injection of the foam, the limb was elevated and bound with 12-cm wide inelastic bandages, which were left in place for three days, and patients wore 30/40 mmHg 7/8 elastic compression stockings for three months thereafter. At the end of the procedure, patients were instructed to walk and to resume their normal routines.
Ultrasound assessment
The examinations were standardized and were all conducted by the same physician. Patients were examined in a standing position with their weight on the contralateral leg, with the limb being examined in external rotation and the calf musculature relaxed, maintaining stability. We employed an ultrasound system (EnVisor; Philips Medical Systems, Andover, MA, USA) with a 10-12 MHz multifrequency transducer. The deep vein system was assessed for acute or previous venous thrombosis. The examination of the superficial vein system focused on the saphenofemoral and saphenopopliteal junctions, together with the great and small saphenous veins, as well as on identifying incompetent perforating veins. Reflux was induced by manual compression of the calf and defined as flow in the retrograde direction for periods greater than 0.5 s for saphenous veins and 0.35 s for perforating veins(10). The GSV diameter was measured at three points: at the saphenofemoral junction; in the proximal third of the thigh, 5 cm distal to the inguinal crease; in the middle third of the thigh, between the inguinal crease and the knee joint line; and in the distal third of the thigh, 5 cm proximal to the knee joint line. The mean of these measurements was calculated for the purposes of comparison.
In most cases, patients underwent seven ultrasound assessments: the first assessment-performed prior to the procedure, to identify reflux patterns; the second assessment-performed during the procedure, with the objective of guiding puncture of the GSV, monitoring injection of the foam and preventing it from entering the deep vein system; the third assessment-performed on post-procedure day 7, with the objective of detecting deep vein thromboses and verifying the occlusion of the GSV; the fourth, fifth, and sixth assessments-performed on post-procedure days 15, 30, and 60, respectively, to evaluate venous thrombus and changes in the diameter of the GSV; and the seventh assessment-performed on post-procedure day 90, to assess treatment efficacy. Patients in whom the GSV was not occluded by the time of the third assessment underwent another foam sclerotherapy session and an assessment following the criteria and objectives of the second assessment, therefore undergoing a total of eight ultrasound assessments.
Statistical analysis
The Bartlett test was applied in order to assess the homogeneity of variances, and the Shapiro-Wilk test was employed to determine whether the study data fitted a normal distribution. Fisher's exact test was used in order to determine whether there was an association between treatment failure and occlusion of the GSV. Statistical calculations were made on an electronic spreadsheet (Microsoft Excel 2000), and statistical analyses were performed with the IBM SPSS Statistics software package, version 23.0 (IBM Corporation, Armonk, NY, USA).
RESULTS
We recruited 33 patients with primary varicose veins in the lower extremities. In all of the patients, the primary varicose veins were classified as CEAP clinical stage C4, C5, or C6 and GSV reflux was classified as proximal, multisegmental, or diffuse. Of those 33 patients, 3 were excluded: two for having a history of deep vein thrombosis, and 1 for having bronchial asthma. Therefore, a total of 30 patients-26 women and 4 men, with a mean age of 62 years (range, 32-70 years)-completed the 90-day protocol.
The primary varicose vein was classified as CEAP C4 in 19 patients (63.3%), as CEAP C5 (with healed ulcers) in 5 (16.7%), and as CEAP C6 (with unhealed ulcers) in 6 (20.0%). All of the patients showed GSV reflux, which was classified as diffuse in 12 patients (40%) and as proximal in 9 (30%). In the pre-procedure assessments, the mean GSV diameter was 6.0 ± 3.2 mm (range, 3.6-11.2 mm).
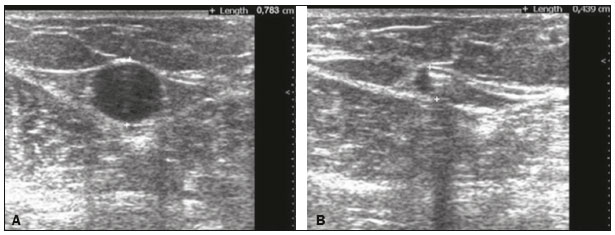
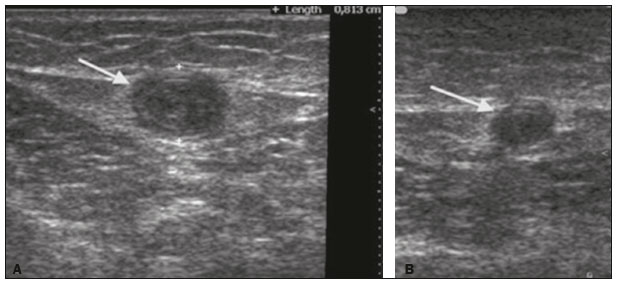
The first change to the saphenous vein observed on duplex ultrasound immediately after injection of the foam is a rapid reduction in the caliber of the vessel, caused by the vasospasm provoked by the foam. Figure 1 illustrates the reduction in caliber of the saphenous vein in one of the patients evaluated in the present study. During sclerotherapy, the mean GSV diameter was 1.9 ± 0.15 mm (range, 0.6-3.8 mm). In the follow-up ultrasound examination performed on post-procedure day 7, the calibers of treated GSVs had increased, the mean diameter being 6.3 ± 0.28 mm (range, 3.9-9.7 mm). All veins that had been treated with sclerotherapy were not compressible with the transducer, exhibiting parietal thickening, as well as luminal content with a homogenous appearance that was predominantly hypoechoic. In all cases, there was no flow seen on color or pulsed-wave Doppler.

![]()
![]()
![]()


 PDF English
PDF English
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket