Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 4 - July / Aug. of 2009
Vol. 42 nº 4 - July / Aug. of 2009
|
REVIEW ARTICLE
|
|
Thyroid ophthalmopathy revisited |
|
|
Autho(rs): Karina Freitas Soares Machado, Marcelo de Mattos Garcia |
|
|
Keywords: Thyroid ophthalmopathy, Extraocular muscles, Magnetic resonance imaging, Computed tomography |
|
|
Abstract:
Karina Freitas Soares Machado; Marcelo de Mattos Garcia Titular Members of Colégio Brasileiro de Radiologia e Diagnóstico por Imagem (CBR), São Paulo, SP, MDs, Radiologists at Axial Centro de Imagem, Belo Horizonte, MG, Brazil
INTRODUCTION Thyroid ophthalmopathy is an autoimmune orbital disorder closely associated with hyperthyroidism (Graves' disease), although both conditions may also occur isolatedly. The most accepted theory to explain the association between thyroid ophthalmopathy and autoimmune thyroid disease comprises a possible cross-reaction of sensitized T-lymphocytes and/or antibodies against common antigens for both the thyroid and the orbita(1). In a great number of cases, thyroid ophthalmopathy may occur concomitantly with the onset of hyperthyroidism, but also it may precede or follow the onset of the thyroid dysfunction(1,2), although in few cases euthyroid and hypothyroid patients may be affected(3,4). In most of cases, the disease is self-limited, and if a treatment is indicated, systemic corticoid therapy is the main strategy adopted(1). Thyroid ophthalmopathy is the most frequent cause of orbital disease in the adult population, responsible for 15% to 28% of cases of unilateral exophthalmia and 80% of cases of bilateral exophthalmia(1,2). The active phase of the disease is progressive, lasting from several months to few years, usually from one to three years, with the inflammation settling to a more quiescent or inactive phase characterized by the presence of fibrosis(2,5). This disease is characterized by inflammation, congestion, hypertrophy, fat and orbital muscles fibrosis leading to increase in volume of these muscles(1). Supplementary evaluation is performed with computed tomography (CT) and magnetic resonance imaging (MRI) which plays a significant role in the demonstration and better characterization of a wide spectrum of clinical findings.
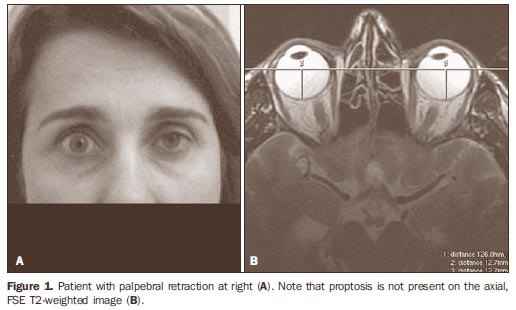
CLINICAL AND IMAGING FINDINGS The natural history of the disease is divided into an acute or inflammatory, progressive phase histologically associated with lymphocytic infiltration and edema, followed by an inactive and fibrotic phase associated with fibrotic alterations and fat infiltration of retro-orbital tissues, particularly the extraocular muscles(4,5). Usually, signs and symptoms of thyroid ophthalmopathy develop within one year after the thyroid dysfunction onset. Extraocular muscles are most frequently involved by the immunological phenomenon and, as a result, they present increase in volume which, in association with abnormalities in the retro-orbital fat, determines ophthalmoplegia and proptosis(1,6). Other relevant clinical signs determined by inflammatory alterations and/or vascular congestion include lower and upper eyelid retraction (Figure 1), conjunctival hyperemia and periorbital edema(1,2), as well as sequelae resulting from extraocular muscles hypertrophy, such as visual loss resulting from corneal ulceration secondary to proptosis and optic neuropathy caused by optic nerve compression at the apex of the orbit(1,4,7,8).
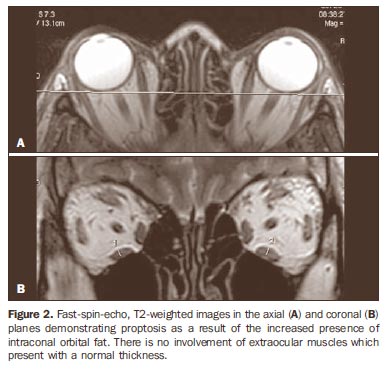
Nearly always, exophthalmia is bilateral and generally relatively symmetrical. The inferior rectus muscle is most frequently involved, followed by the medial rectus, superior rectus and lateral rectus muscles(1,2). The disease diagnosis is based on clinical findings, and imaging methods are indicated in cases where the diagnosis is dubious or in the suspicion of optic neuropathy(2). CT and MRI are useful methods for confirming the diagnosis by visualizing the orbital muscles and fat hypertrophy, and evaluating the critical region of the orbital apex(3). Many times, increased orbital fat volume and resulting proptosis will be observed as the sole imaging finding(3) (Figure 2).
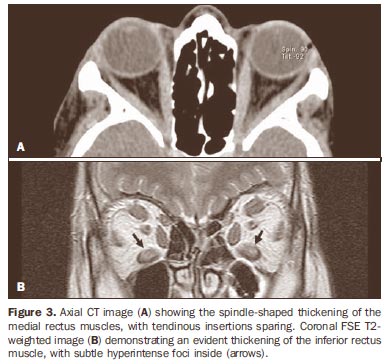
Muscles involvement is typically ventral, sparing the tendinous insertions (Figure 3), in association with other useful finding, i.e., hypodense foci at CT and hyperintense foci on T2-weighted MRI, involving the muscle bellies, probably because of inflammatory infiltrate (Figure 3).
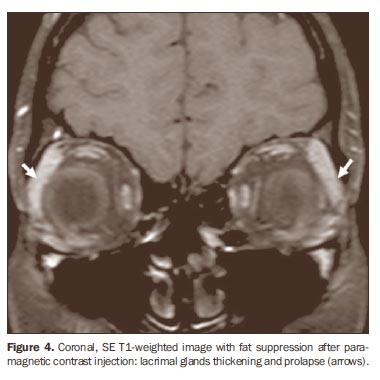
Other imaging findings in the active or inflammatory phase of the disease include lacrimal gland hypertrophy and prolapse (Figure 4), palpebral edema, anterior displacement of the orbital septum. Optic nerve stretching and orbital bone wall remodeling(1,3,9-11).
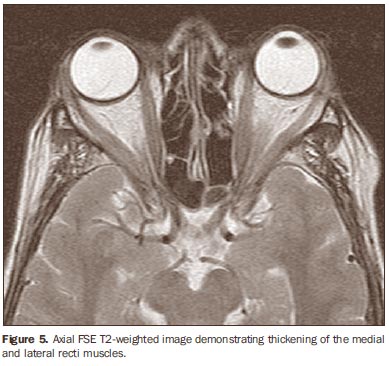
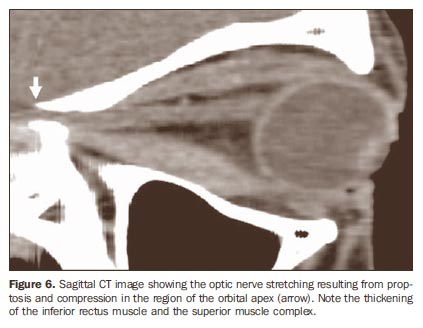
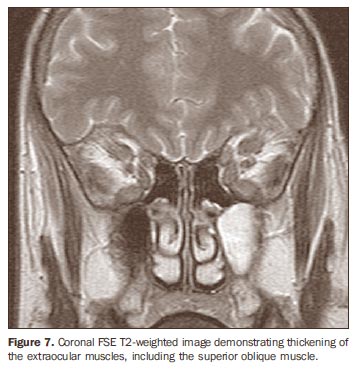
Extraocular muscles thickening can also be observed in other diseases that should be eventually considered in the differential diagnosis; among them, orbital pseudotumor and lymphoproliferative processes. In these cases, unilateral involvement is most frequently observed without sparing the tendinous insertions(12). Additionally, the clinical condition is usually associated with pain. Most rarely, orbital amyloidosis and metastatic neoplastic process can be mentioned, the latter being usually secondary to breast neoplasm, in general with a nodular pattern(12). Axial images are utilized to estimate the proptosis degree, the volumetric increase of the medial and lateral rectus muscles (Figure 5) and the relation between these muscles and the optic nerve. The optic nerve compression at the orbital apex also is best evaluated in the axial plane with the aid of coronal and sagittal images(10) (Figure 6). The coronal plane is best for evaluating the inferior and superior recti muscles and the superior oblique muscle (Figure 7)(7,13).
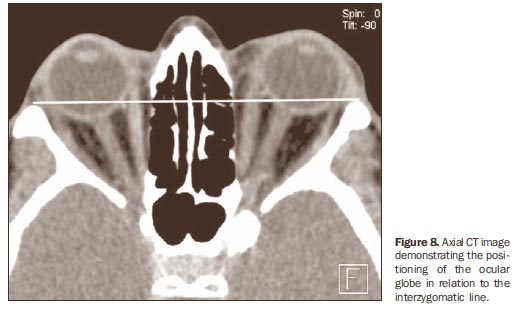
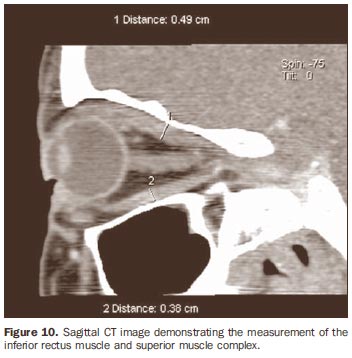
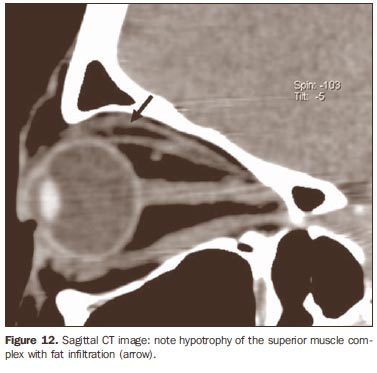
The tomographic images are acquired in the axial and coronal planes, the first one with an approximate angle of -10º to -15º in relation to the orbitomeatal plane, and the latter almost perpendicular to the axial plane. It is important to note that the risk for thyrotoxicosis should be taken into consideration in the utilization of computed tomography with iodinated contrast agents(4). The normal positioning of the ocular globe is determined by a straight line connecting the zygomatic processes, utilizing the median portion of the globe as a reference (interzygomatic line). The measurement of the ocular globe positioning is based on the distance between the interzygomatic line and the posterior margin on the median portion of the ocular globe in the axial plane (Figure 8). The superior rectus muscle and the elevator muscle of the upper eyelid are measured in conjunction, considering that they cannot be easily distinguished from each other, thus comprising the superior muscle group (Figure 9). Vertical diameters of the superior muscle group and inferior rectus muscle can be best obtained in the coronal and sagittal planes (Figure 10). The horizontal diameters of the lateral and medial recti muscles are measured with higher reliability in the axial plane(14) (Table 1).
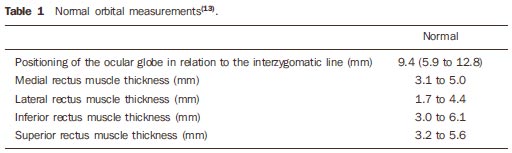
MRI is the best imaging method for evaluating the orbital structures because of its better tissue resolution and absence of ionizing radiation(15). The protocol for examination with MRI in the author´s institution is comprised of spin-echo T1-weighted sequences in the axial and coronal planes, multiechoes T2weighted sequence in the coronal plane, and short time inversion recovery (STIR) sequence in the coronal plane. Paramagnetic contrast-enhanced images are acquired with T1-weighted sequence with fat-suppression in the axial, coronal and sagittal oblique planes(16). Normal extraocular muscles are characterized by low signal intensity on T1-weighted sequences and low to intermediate signal intensity on T2-weighted sequences, with well-defined margins. There is a marked contrast enhancement, related to the great vascular supply to the extraocular muscles (Figure 11)(1).
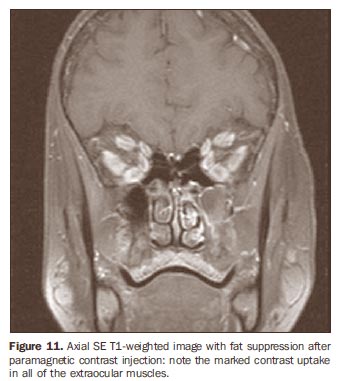
The T1-weighted sequence offers a better contrast resolution for evaluating the region and measurement of the extraocular muscles(17), while the physiopathological condition of these muscles is best evaluated on T2-weighted sequences(16). Because of the capability to evaluate the water contents of tissues by means of long TR-weighted sequences with and without fat-suppression (respectively T2-weighted and STIR), MRI is a useful method for approaching the disease activity, identifying inflammatory and edematous alterations involving the muscles through an increase in the signal intensity on T2weighted sequences, which is critical to achieve a good outcome of the anti-inflammatory treatment whose effectiveness only can be achieve in the active phase of the disease(1,3,5-8,17,18). This information corroborates the MRI's superiority over other imaging methods in the follow-up of the disease progression. Some authors describe a correlation between the pattern of muscle involvement on T2-weighted sequences and the reversibility of diplopia. In cases where the signal intensity was uniformly increased, a better response to the treatment was observed, but, when the signal intensity was heterogeneous, the diplopia tended to be irreversible(19). Hypertrophy of the extraocular muscles is observed and increase in their signal intensity on T2-weighted images indicates the edematous or inflammatory phase of the disease(18). On the other hand, decreased signal intensity of these muscles on T1- and T2-weighted sequences suggests the presence of chronic fibrotic alterations. Hyperintense intramuscular foci on T1- and T2-weighted sequences are suggestive of chronic fat degeneration(1,3,5), which also can be identified at CT through hypoattenuating areas corresponding to fat infiltration (Figure 12). These latest findings indicate chronic, non-congestive phase of the disease with restricted ocular motion secondary to extraocular muscles fibrosis and subsequent loss of elasticity(3) in association with volume decrease in these muscles(5)corresponding to lack of response to the clinical treatment.
Surgical orbital decompression or radiotherapy may be indicated in the setting of compressive optic neuropathy to prevent a significant vision loss(12). The surgical procedure is aimed at achieving orbital enlargement by means of a partial bone removal from one of the four orbital walls, depending on the required decompression degree(20). On images of all the extraocular muscles, the paramagnetic contrast enhancement has shown to be significantly decreased in patients with thyroid ophthalmopathy at the edematous phase, while on T2-weighted images the signal intensity was increased, thus inferring a decrease in the vascular supply in the acute phase of this disease which, in the future, with the development of additional studies and improvement of MRI techniques, will probably allow the prediction of the severity, type of therapy and prognosis for the disease(1).
CONCLUSION Imaging methods (CT and MRI) play a significant role as an aid in the evaluation of patients with endocrine ophthalmopathy, especially those with signs of optic neuropathy, and in the demonstration of the wide spectrum of findings involving the orbital structures, both in the inflammatory and fibrotic phases of the disease. MRI plays the most relevant role in the differentiation of the disease phases, allowing the detection of inflammatory signs indicative of the disease activity, which is important for selecting the patients eligible for anti-inflammatory therapy, with a great influence on the prognosis. Additionally, MRI is the method of choice in the therapeutic follow-up of these patients for evaluating the response translated into reversal of inflammatory signs and consequential development of fibrosis and hypertrophy of extraocular muscles.
REFERENCES 1. Cakirer S, Cakirer D, Basak M, et al. Evaluation of extraocular muscles in the edematous phase of Graves ophthalmopathy on contrast-enhanced fat-suppressed magnetic resonance imaging. J Comput Assist Tomogr. 2004;28:80-6. [ ] 2. El-Kaissi S, Frauman AG, Wall JR. Thyroid-associated ophthalmopathy: a practical guide to classification, natural history and management. Intern Med J. 2004;34:482-91. [ ] 3. Mafee MF. Orbit: embryology, anatomy and pathology. In: Som PM, Curtin HD, editors. Head and neck imaging. 4th ed. St Louis: Mosby; 2003. p. 529-654. [ ] 4. Fung S, Malhotra R, Selva D. Thyroid orbitopathy. Aust Fam Physician. 2003;31:615-20. [ ] 5. Yokoyama N, Nagataki S, Uetani M, et al. Role of magnetic resonance imaging in the assessment of disease activity in thyroid-associated ophthalmopathy. Thyroid. 2002;12:223-7. [ ] 6. Kahaly GJ. Recent developments in Graves' ophthalmopathy imaging. J Endocrinol Invest. 2004; 27:254-8. [ ] 7. Hosten N, Sander B, Cordes M, et al. Graves ophthalmopathy: MR imaging of the orbits. Radiology. 1989;172:759-62. [ ] 8. Mayer EJ, Fox DL, Herdman G, et al. Signal intensity, clinical activity and cross-sectional areas on MRI scans in thyroid eye disease. Eur J Radiol. 2005;56:20-4. [ ] 9. Nugent RA, Belkin RI, Neigel JM, et al. Graves orbitopathy: correlation of CT and clinical findings. Radiology. 1990;177:675-82. [ ] 10. So NMC, Lam WWM, Cheng G, et al. Assessment of optic nerve compression in Graves' ophthalmopathy. The usefulness of a quick T1-weighted sequence. Acta Radiol. 2000;41:559-61. [ ] 11. Rothfus WE, Curtin HD. Extraocular muscle enlargement: a CT review. Radiology. 1984;151: 677-81. [ ] 12. Parmar H, Ibrahim M. Extrathyroidal manifestations of thyroid disease: thyroid ophthalmopathy. Neuroimaging Clin N Am. 2008;18:527-36. [ ] 13. Szucs-Farkas Z, Toth J, Balazs E, et al. Using morphologic parameters of extraocular muscles for diagnosis and follow-up of Graves' ophthalmo pathy: diameters, areas, or volumes? AJR Am J Roentgenol. 2002;179:1005-10. [ ] 14. Ozgen A, Ariyurek M. Normative measurements of orbital structures using CT. AJR Am J Roentgenol. 1998;170:1093-6. [ ] 15. Prummel MF, Gerding MN, Zonnevedl FW, et al. The usefulness of quantitative orbital magnetic resonance imaging in Graves' ophthalmopathy. Clin Endocrinol (Oxf). 2001;54:205-9. [ ] 16. Majos A, Pajak M, Grzelak P, et al. Magnetic resonance evaluation of disease activity in Graves' ophthalmopathy: T2-time and signal intensity of extraocular muscles. Med Sci Monit. 2007;13 Suppl 1:44-8. [ ] 17. Lennerstrand G, Tian S, Isberg B, et al. Magnetic resonance imaging and ultrasound measurements of extraocular muscles in thyroid-associated ophthalmopathy at different stages of the disease. Acta Ophthalmol Scand. 2007;85:192-201. [ ] 18. Ohnishi T, Noguchi S, Murakami N, et al. Extraocular muscles in Graves ophthalmopathy: usefulness of T2 relaxation time measurements. Radiology. 1994;190:857-62. [ ] 19. Aydin K, Güven K, Sencer S, et al. A new MRI method for the quantitative evaluation of extraocular muscle size in thyroid ophthalmopathy. Neuroradiology. 2003;45:184-7. [ ] 20. Goldberg RA. The evolving paradigm of orbital decompression surgery. Arch Ophthalmol. 1998; 116:95-6. [ ] Received November 7, 2008. * Study developed at Axial Centro de Imagem, Belo Horizonte, MG, Brazil. |
|


Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554