Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 4 - July / Aug. of 2009
Vol. 42 nº 4 - July / Aug. of 2009
|
ORIGINAL ARTICLE
|
|
Gastroesophageal reflux: a comparative study of receptiveness and sensitivity of upper gastrointestinal series and ultrasonography |
|
|
Autho(rs): Makoto Sakate, Guilherme Lopes Silveira, Bruno Paulino de Muzio, Hudson Teigao Junior, Jorge Guilherme Okanobo Ozaki, Marcelo Dimas Spadim, Roberto Cesar Teixeira Dantas, Nilton Carlos Machado |
|
|
Keywords: Gastroesophageal reflux, Intraabdominal esophagus, Ultrasonography, Contrast-enhanced study |
|
|
Abstract:
IPhD, Assistant Professor of the Discipline of Radiodiagnosis, Department of Tropical Diseases and Imaging Diagnosis - Faculdade de Medicina de Botucatu da Universidade Estadual Paulista (FMB-Unesp), Botucatu, SP, Brazil
INTRODUCTION Gastroesophageal reflux (GER) is the involuntary passage of the gastric content backwards up into the esophagus. It is a relevant and relatively frequent finding in infants(1,2). In neonates, this disorder may be physiological in nature and, in most of cases, self-limited and benign(3). Esophageal reflux occurs because of a defect and/or immaturity of the lower esophageal sphincter(4,5). The integrity of this functional valvular system is important to avoid the gastric content reflux, considering that the intraabdominal pressure is higher than the intrathoracic pressure. The refluxed material is rapidly returned into the stomach by the secondary esophageal peristaltic waves(6,7). The gastric content reflux degree may range from mild to severe, and the frequency is variable. In most of cases, the gastroesophageal reflux is mild, transitory, bringing no consequence in particular. However, persistent episodes should be considered as pathologic(8,9). The traditional method for studying GER is the upper gastrointestinal series (UGIS) with barium and, most recently, intraabdominal esophagus ultrasonography (IEUS)(10,11). Similarly to UGIS, IEUS allows a safe, noninvasive evaluation of structural anatomic details and can identify several pathologic processes, including GER, in real time(12) and without ionizing radiation. The present study is aimed at comparing the receptiveness (cooperation) and sensitivity of UGIS in relation to IEUS in pediatric patients with suspicion of GER.
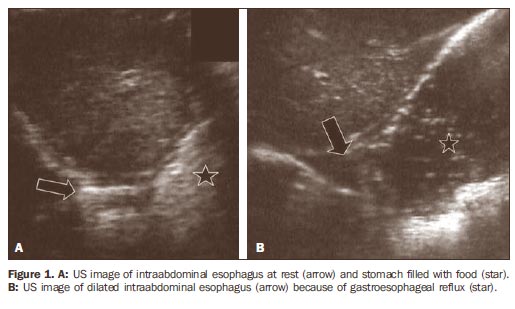
MATERIALS AND METHODS The research project was presented and received the approval from the Committee for Ethics in Research of the Institution were the study was developed. A term of free and informed consent was signed by the parents of the patients, who had received information on the study methodology. The present study included 42 pediatric patients with suspicion of GER, as follows: 26 boys with ages ranging between 1 and 120 months (mean, 33.64 ± 34.33 months), and 16 girls between 2 and 113 months (mean, 31.02 ± 35.56 months). All the patients were previously submitted to UGIS in accordance with the protocol of the service of radiodiagnosis, and an additional examination form being filled out. In the present study the additional examination form included the following data: name, age, sex, weight, height, number of reflux episodes observed, time of intermittent observation with five-minute radioscopy after barium repletion, besides an indication of the behavior of the patient as follows: cooperative (c), partially cooperative (pc), excited during examination (ede), and very difficult patient (vdp). The UGIS technique utilized corresponded to the protocol of the unit of radiology consisting of: after four-hour fast, the patient was placed on the examination table of the x-ray equipment in right lateral decubitus position. During the ingestion of diluted barium through a baby bottle, three radiographic views of the esophagus were obtained (initial phase, during and after ingestion). Subsequently contrast-enhanced images were acquired from the stomach and duodenal arch. Once a complete repletion of the stomach was achieved, the patient was placed in horizontal dorsal decubitus and a five-minute intermittent radioscopy was performed in an attempt to observe and recording the GER. After the UGIS, all the patients were referred to the ultrasonography department. The US equipment utilized was a Logiq 400 (General Electric Medical Systems; Milwaukee, USA), with 2-5 MHz semiconvex transducer. After approximately one-week interval, IEUS was performed by a single sonographist who did not know the results of the previous UGIS. The examination was performed at morning, after breakfast with breast milk, infant formula or yogurt (for the older children) for GER study. The patients were placed in horizontal dorsal decubitus, with their head slightly raised. The IEUS was performed with the transducer placed on the left region of the xiphoid appendix(13) for identifying the intraabdominal esophagus. Real-time continuous observation was developed along five minutes. Similarly to the UGIS form, a IEUS form was filled out with the following data: age, sex, weight, height, GER presence or absence, number of GER episodes and behavior of the patients during examination. The study was recorded on a videotape for later, detailed analysis of the local anatomic conditions (Figure 1).
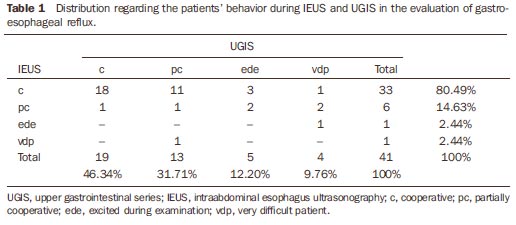
Data of both UGIS and IEUS were statistically analyzed for evaluation of intermethod agreement by means of the chi-square test (χ2), and according to the confidence interval for agreement ratio(14). RESULTS In the comparative study considering sex and age of the 42 children submitted to diagnostic imaging for GER, the statistical analysis by the χ2 test suggests that there is no evidence of association between the patients cooperation both for the UGIS (p = 0.98745) and the IEUS (p = 0.3966) techniques. However, in the classification of the patients' behavior during examination, the UGIS technique presented < 50% of cooperation, while 80.49% of the children cooperated with the IEUS. Practically, all the children who cooperated in the UGIS also did it with the IEUS (94.74%). Among the 22 children who were noncooperative during UGIS, 68.18% cooperated with the IEUS technique (Table 1).
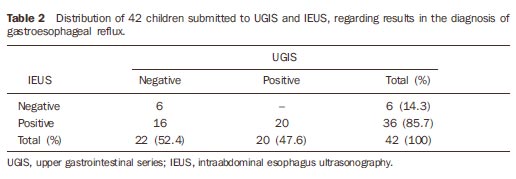
Statistically, one can conclude that there is a difference between the UGIS and IEUS technique in terms of rates corresponding to the different levels of cooperation (McNemar's test: U2 = 12.25; p = 0.0005). In terms of cooperation, both techniques are positively associated (χ2 = 4.578; p = 0.0324). As regards the diagnostic results of both techniques (UGIS and IEUS), IEUS was significantly superior to UGIS (Tables 2 and 3).
Statistically, one can conclude that there is a difference in the rate of positive results for GER between the UGIS (47.6%) and IEUS (85.7%) techniques (McNemar's test: U2 = 16.0; p = 0.00006). In terms of diagnosis for gastroesophageal reflux, both techniques are positively associated (χ2 = 6.3636; p = 0.01165).
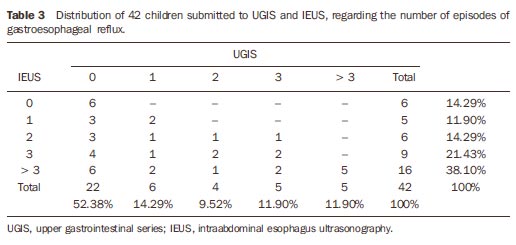
DISCUSSION Gastroesophageal reflux is a well known entity frequently found in pediatric patients. Several methods are available for evaluation of this condition in children: 24hour esophageal pH test, radioisotope scintigraphy and UGIS, the latter being the method most frequently utilized to confirm the presence of GER and mainly for ruling out obstructive diseases such as vascular compression, congenital esophageal stenosis, among others(15,16). Esophageal pH test is performed with the placement of an electrode in the terminal region of the esophagus for 24-hour continuous recording of the ph values in this region(17). Because of this method characteristics, it is considered as an invasive study. Scintigraphy is performed in the suspicion of GER, after swallowing of a food bolus mixed with a radioactive substance. An increase in the uptake, by the esophageal region, of the radiation coming from the gastric region during a given time, means that GER has occurred(16). This method requires the utilization of radioactive material and highly expensive equipment, so its utilization as a routine study is unfeasible. UGIS is performed with an ionizing radiation source (x-rays) both during and after barium ingestion. Intermittent observation of the stomach fundus filled with barium is performed with radioscopy for detecting the contrast medium reflux from the stomach backwards up to the esophagus(10). Currently, the comparative study of IEUS and UGIS has demonstrated that IEUS presents a higher sensitivity in the diagnosis of GER(9,17) and in the evaluation of the intraabdominal esophagus, with a reduction of the exposure to ionizing radiation for these patients(11,18). However, the determination of reflux degree as well as the evaluation of the intrathoracic esophagus cannot be performed with this method(18,19). The determination of the GER degree could be done with IEUS, although not as specifically as the UGIS does, by means of a comparative study between these two techniques. The GER degree obtained at UGIS for each patient would be compared with the diameter and the time of opening of the intraabdominal esophagus during the GER observed at the IEUS(20,21) in the same patient. After this analysis the GER degree could be inferred only with IEUS. The intrathoracic esophagus could be indirectly evaluated with the utilization of the "esophageal time"(18), that allows the determination of the typical esophageal 2 31 1 1 -614.29% transit time for a liquid or pasty food from the moment of deglutition up to its passage through the intraabdominal esophagus. Most of times, the association of "esophageal time" and IEUS could evaluate the UGIS, upper gastrointestinal series; IEUS, intraabdominal esophagus ultrasonography. intrathoracic esophagus and, indirectly, the GER in the majority of cases, especially in centers where only ultrasonography units are available. In the presence of obstructive diseases of the intrathoracic esophagus, such as vascular compression, dysphagia and odynophagia will be observed during food ingestion, and with increase in the esophageal time at IEUS. Different practitioners performed the UGIS (physicians, residents in radiodiagnosis) and IEUS (a physicians-sonographist), which may imply more or less empathy with the children. Even so, it is suggested that IEUS is performed in cases where gastroeshophageal reflux is not detected by UGIS, considering that more than half (52.4%) of diagnoses by UGIS are negative and, on the other hand, more than 80% of the patients are diagnosed as positive by IEUS. The discrepancy between the diagnoses with the two methods becomes evident in cases of reflux > 3, where the rates achieve 11.9% and 38%, respectively for UGIS and IEUS, similarly to the results reported by Milward(11). However, the authors could not find in the literature, similar studies evaluating and comparing the patients' receptiveness (cooperation) with these two diagnostic modalities. Probable limiting factors for UGIS are: examination room illumination, number of outsiders in the room, presence of equipment unfamiliar to the child, ingestion of substances with unpleasant flavor (barium), and movement in the room. Additionally, one must consider the utilization of an appropriate dose-area product of ionizing radiation(22), but exposing young, growing patients, whose probability of interaction with radiation is higher. Positive aspects related to the IEUS technique are: calm environment, equipment with less frightening appearance with a TV-like display, half-light, ingestion of a substance with pleasant flavor (infant formula or yogurt) and few persons in the room. Additionally, there are other advantages of ultrasonography: low-cost, noninvasiveness, short examination time, and the functioning of the organ and adjacent structures is not affected (both at short- and long-term). The examination can be repeated as many times as necessary in even more physiological circumstances, in realtime, allowing the evaluation of normal anatomic structural details or identification of local pathological processes.
CONCLUSION The comparative study of the sensitivity and children receptiveness (cooperation) in relation to the IEUS, with gastric repletion (breast milk, infant formula or yogurt), and UGIS with barium, in the evaluation of GER, has demonstrated the following aspects: first, a higher level of cooperation from the patients at IEUS as compared with UGIS in the evaluation of GER; secondly, IEUS demonstrated higher sensitivity in the diagnosis of GER; thirdly, the present study suggests that, most of times, IEUS can substitute UGIS for indirectly evaluating the intrathoracic esophagus and GER, especially in centers where only ultrasonography is available.
REFERENCES 1. Costa L, Campobasso P. Gastroesophageal reflux. Pediatr Med Chir. 1999;21(5 Suppl):33-52. [ ] 2. Naik DR, Bolia A, Moore DJ. Comparison of barium swallow and ultrasound in diagnosis of gastro-oesophageal reflux in children. Br Med J (Clin Res Ed). 1985;290:1943-5. [ ] 3. Balistreri WF, Farrell MK. Gastroesophageal reflux in infants. N Engl J Med. 1983;309:790-2. [ ] 4. Gomes H, Lallemand A, Lallemand P. Ultrasound of the gastroesophageal junction. Pediatr Radiol. 1993;23:94-9. [ ] 5. Boix-Ochoa J, Canals J. Maturation of the lower esophagus. J Pediatr Surg. 1976;11:749-56. [ ] 6. Boix-Ochoa J. The physiologic approach to the management of gastric esophageal reflux. J Pediatr Surg. 1986;21:1032-9. [ ] 7. DeMeester TR, Wernly JA, Bryant GH, et al. Clinical and in vitro analysis of determinants of gastroesophageal competence. A study of the principles of antireflux surgery. Am J Surg. 1979; 137:39-46. [ ] 8. Costa CD, Zomignan HP, Rocha JIP, et al. Refluxo gastroesofágico em pediatria: estudo radiológico. Pediat (S Paulo). 1986;8:136-40. [ ] 9. Swischuk LE. Alimentary tract. In: Swischuk LE, editor. Imaging of the newborn, infant and young child. 3rd ed. Baltimore: Williams & Wilkins; 1989. p. 353-69. [ ] 10. Meschan I, Ott D. Oropharynx, laryngopharynx, and esophagus. In: Meschan I, editor. Roentgen signs in diagnostic imaging: abdomen. 2nd ed. Philadelphia: WB Saunders; 1984. p. 487-560. [ ] 11. Milward CMMO. A ultrassonografia como método diagnóstico do refluxo gastroesofágico no paciente pediátrico. Radiol Bras. 2004;37:230. [ ] 12. Mádi-Szabó L, Kocsis G. Examination of gastroesophageal reflux by transabdominal ultrasound: can a slow, trickling form of reflux be responsible for reflux esophagitis? Can J Gastroenterol. 2000; 14:588-92. [ ] 13. Cerri GG. Vísceras ocas. In: Rocha DC, Cerri GG, Prando A, et al. Ultrassonografia abdominal. São Paulo: Sarvier; 1988. p. 169-86. [ ] 14. Zar JH. Biostatistical analysis. 3rd ed. New Jersey: Prentice-Hall; 1996. [ ] 15. Gomes H, Menanteau B. Gastro-esophageal reflux: comparative study between sonography and pH monitoring. Pediatr Radiol. 1991;21:168-74. [ ] 16. González Fernández F, Argûelles Martin F, Rodriguez de Quesada B, et al. Gastroesophageal scintigraphy: a useful screening test for GE reflux. J Pediatr Gastroenterol Nutr. 1987;6:217-9. [ ] 17. Schindlbeck NE, Heinrich C, König A, et al. Optimal thresholds, sensitivity, and specificity of long-term pH-metry for the detection of gastroesophageal reflux disease. Gastroenterology. 1987; 93:85-90. [ ] 18. Sakate M, Teixeira AS, Yamashita S, et al. Um novo método de avaliação do "tempo esofágico" com ultra-sonografia por abordagem externa. Radiol Bras. 2008;41:309-12. [ ] 19. Westra SJ, Derkx HH, Taminiau JA. Symptomatic gastroesophageal reflux: diagnosis with ultrasound. J Pediatr Gastroenterol Nutr. 1994;19: 58-64. [ ] 20. Lynch CS, Chammas MC, Mansur LL, et al. Biomecânica ultra-sonográfica da deglutição: estudo preliminar. Radiol Bras. 2008;41:241-4. [ ] 21. Spadotto AA, Gatto AR, Cola PC, et al. Software para análise quantitativa da deglutição. Radiol Bras. 2008;41:25-8. [ ] 22. Costa MMB, Canevaro LV, Azevedo ACP, et al. Valores típicos do "produto dose-área" (DAP) obtidos durante o estudo videofluoroscópico da deglutição. Radiol Bras. 2003;36:17-20. [ ] Received September 26, 2008. * Study developed at the Center of Diagnostic Imaging — Hospital das Clínicas da Faculdade de Medicina de Botucatu da Universidade Estadual Paulista (FMB-Unesp), Botucatu, SP, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554