Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 4 - July / Aug. of 2009
Vol. 42 nº 4 - July / Aug. of 2009
|
ORIGINAL ARTICLE
|
|
Volumetric assessment of neointimal hyperplasia in iliac arteries after metal stent implantation |
|
|
Autho(rs): Samuel Martins Moreira, Antonio Massamitsu Kambara, Sergio Ajzen, José de Ribamar Costa Junior |
|
|
Keywords: Stent, Iliac artery, Interventional ultrasonography, Hyperplasia |
|
|
Abstract:
IAssistant Physician, Universidade Federal de São Paulo/ Escola Paulista de Medicina (Unifesp/EPM), São Paulo, SP, Brazil
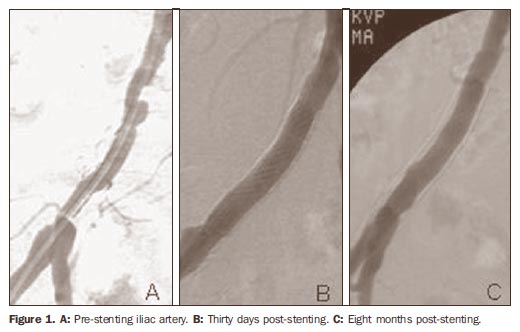
INTRODUCTION Percutaneous transluminal angioplasty with metal stents for the treatment of occlusive lesions of iliac arteries is a safe and effective procedure(1-3), generally accepted as the first method of choice for treatment in selected cases(4-6). Intra-stent restenosis caused by neointimal hyperplasia has its occurrence peak around the sixth postoperative month (Figure 1), and it has been described in other locations such as the coronary arteries(7-9)although such occurrence has not been reported with the same frequency as in the case of iliac arteries.
In the present study, intravascular ultrasonography (IVUS) was performed to quantify the volume of neointimal hyperplasia in iliac arteries treated with percutaneous transluminal angioplasty and stent, correlating with clinical risk factors such as smoking, arterial hypertension, hyperlipidemia and diabetes mellitus as well as stents material and local arterial characteristics such as type of occlusion.
MATERIALS AND METHODS Between July, 2003 and August, 2005, 60 consecutive patients were submitted to percutaneous transluminal angioplasty and stenting for treatment of occlusive lesions in the iliac arteries. Among these patients, 30 were re-studied with IVUS (In-Vision Gold®; Volcano Therapeutics, Rancho Cordova, USA), 16 of them men (53.3%), with ages ranging from 39 to 78 years (mean, 60.3 years). As regards clinical risk factors, 22 patients had arterial hypertension (73.3%), 18 patients were smokers (62.1%), 20 were hyperlipidemic (66.7%) and nine had diabetes mellitus (30%) (Table 1). According to the Rutherford scale, the patients were classified into categories 2 (moderate claudication), 3 (severe claudication), 4 (ischemic rest pain) and 5 (minor trophic lesion); and regarding arterial involvement by the atheromatous plaque, the TASC I classification was utilized, and the patientswere graded as A, B, and C(4).
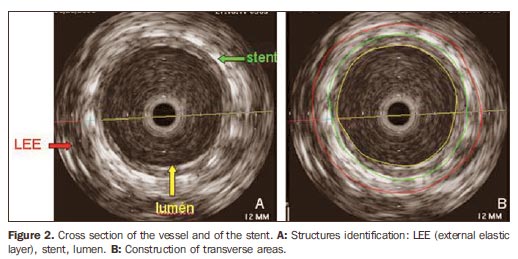
All patients included in the present study underwent the procedure in a cath lab, with 2% lidocaine hydrochloride local anesthetic, without vasoconstrictor. The ipsilateral retrograde femoral approach was preferably utilized, followed by the contralateral femoral approach, and the axillary approach as the last option. Among the enrolled patients, 20 received self-expandable nitinol stents and 10 received balloon stainless steel stents based on criteria established in literature(10). In 24 of the arteries, significant stenosis was present (80%) and in six of the arteries, occlusion was present (20%). Anti-platelet regimen included a loading dose of aspirin (200 mg) at least 2 days prior to the procedure followed by 200 mg/ day indefinitely. Additionally, patients were pretreated with ticlopidine (500 mg) or clopidogrel (75 mg) a day, two days before the intervention and maintained for 30 days(11). The patients were followed up on an outpatient basis at one week, one month, three months, six months and eight months postoperatively, when the IVUS re-studies were then performed. The patients who agreed in participating in the present research, signed a term of free and informed consent and were submitted to the re-study. In a cath lab, with the patient under local anesthesia, a 6F valved introducer was inserted by ipsilateral retrograde femoral approach, and 5000 UI intra-arterial heparin was injected. Next, a 0.014" guidewire was inserted and positioned in the thoracic aorta distally to the stent. Over the guidewire, a catheter with a 20 MHz transducer on its tip, connected to a IVUS module table, reading module of the IVUS, was advanced and positioned distally to the stent location. Then, the catheter was connected to a pullback device (Trak Back II®; Volcano Therapeutics, Rancho Cordova, USA) with a constant 1 mm/s pullback rate. The acquired images were digitized and recorded on a compact disc (CD) and later analyzed in a quantitative analysis laboratory with (the aid of the) a dedicated software (Echoplaque®; Indec Systems, Mountain View, USA). By using the IVUS, it was possible to identify and delimitate the external elastic layer, the stent and the lumen (Figure 2). With these measurements, the vessel, the stent, and lumen areas could be calculated at each millimeter within the stent; subsequently, the volumes calculations were performed with the aid of the software. By subtracting the luminal volume the stent volume, the neointimal hyperplasia volume was determined.
A linear regression model was adjusted to evaluate the correlation between the intrastent occlusion rate, arterial hypertension, smoking, hyperlipidemia, diabetes mellitus, stainless steel, stenosis and occlusion(12,13).
RESULTS All patients underwent follow-up IVUS, and no complication was observed in these patients. Eight stents were implanted in the right common iliac artery, 14 in the left common iliac artery, 5 in the right external iliac artery and 3 in the left external iliac artery. The first report of the TransAtlantic Inter-Society Consensus (TASC I) was utilized to classify the anatomic arterial involvement by the atheromatous plaque, as follows: four were TASC A (13.3%), 15 were TASC B (50%) and 11, TASC C (36.7%). As regard the clinical status of the patients at the time of the percutaneous transluminal angioplasty and stenting, and also with follow-up purposes, the Rutherford scale was utilized. Thus, nine patients (30%) were in category 5 (minor trophic lesion), nine (30%) were in category 4 (rest pain), nine were in category 3 (severe limiting claudication) and three (10%) were in category 2 (moderate claudication) at the time of the percutaneous transluminal angioplasty and stenting. At follow-up, 15 patients (50%) were asymptomatic, 13 presented long distance claudication (Rutherford category 1) and two presented moderate distance claudication. The mean neointimal hyperplasia volume was 766.26 mm3 (minimum of 204 mm3 and maximum of 1774 mm3). The intrastent occlusion rate caused by neointimal hyperplasia ranged from 18% to 47% (mean, 27.4%) (Figure 3).
DISCUSSION Follow-up with IVUS demonstrated that after percutaneous transluminal angioplasty and stenting all patients developed neointimal hyperplasia and that this is a common result from the intravascular treatment. However, neointimal hyperplasia was self-limited and did not cause significant restenosis among the 30 patients participating in the present study, suggesting that in vessels of larger caliber, like iliac artery, only a larger volume hyperplasia could cause restenosis. However, even in cases of significant restenosis, a new catheter balloon or cutting balloon angioplasty can be performed, without the use of a new stent(14). The use of IVUS in the evaluation of intrastent restenosis has shown to be superior to catheter angiography and transcutaneous Doppler ultrasonography with high-frequency transducers, for being able to better identify the structures and also for not underestimating the lumen diameter(15). Neointimal hyperplasia remains as the main cause of failure of endovascular treatment with metallic stents, and much has been done do diminish this response, as follows: the use of heparin stents; the use of anti-ICAM-1 monoclonal antibodies(16), that inhibit the ICAM-1 molecular adhesion, hence neointimal hyperplasia; the use of probucol(17), which accelerates stents endothelialization and reduces the formation of hyperplasia; hyperplasia inhibiting drug-eluting stents(18); and even the oral use of neointimal hyperplasia inhibiting drugs(19). So far, the coating with polytetrafluorethylene (Teflon) has not been able to reduce hyperplasia response(20). Comparative studies between the primary use of stents and utilization of stents in selected cases where catheter balloon angioplasty failed to show good outcomes(21) suggest that stenting should only be used in the iliac arteries, in case of failure of percutaneous transluminal angioplasty with catheter balloon. On the other hand, the type of material utilized in the composition of the stents utilized in the present study - stainless steel and nitinol - did not present differences as far as neointimal hyperplasia is concerned. Causal factors, such as arterial hypertension, diabetes mellitus, smoking and hyperlipidemia were not determinant of statistically significant differences in neointimal hyperplasia and intrastent occlusion, and also no difference was observed in cases of arterial occlusion or stenosis. Thus, the high research costs and the final price of stents are not justifiable for treatment of large caliber arteries such as the iliac ones, even in cases where the patients present a history of diabetes mellitus, arterial hypertension, smoking, hyperlipidemia or complete vessels occlusion.
CONCLUSION The results of the linear regression analysis did not demonstrate statistically significant differences for arterial hypertension, smoking, hyperlipidemia, diabetes mellitus, nitinol, stainless steel, stenosis and occlusion, when correlated with the intrastent occlusion rate in the treatment of atherosclerotic lesions of iliac arteries.
REFERENCES 1. Henry M, Amor M, Ethevenot G, et al. Palmaz stent placement in iliac and femoropopliteal arteries: primary and secondary patency in 310 patients with 2-4 year follow-up. Radiology. 1995;197:167-74. [ ] 2. Bosch JL, Hunink MG. Meta-analysis of the results of percutaneous transluminal angioplasty and stent placement for aortoiliac occlusive disease. Radiology. 1997;204:87-96. [ ] 3. De Roeck A, Hendriks JMH, Delrue F, et al. Longterm results of primary stenting for long and complex iliac artery occlusions. Acta Chir Belg. 2006; 106:187-92. [ ] 4. Management of peripheral arterial disease (PAD). TransAtlantic Inter-Society Consensus (TASC). Section C: acute limb ischaemia. Eur J Vasc Endovasc Surg. 2000;19 Suppl A:S115-43. [ ] 5. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg. 2007;34:411-4. [ ] 6. Bosch JL, Tetteroo E, Mali WP, et al. Iliac arterial occlusive disease: cost-effectiveness analysis of stent placement versus percutaneous transluminal angioplasty. Radiology. 1998;208:641-8. [ ] 7. Roubin GS, King SB 3rd, Douglas JS Jr. Restenosis after percutaneous transluminal coronary angioplasty: the Emory University Hospital experience. Am J Cardiol. 1987;60:39B-43B. [ ] 8. Palmaz JC. Intravascular stents: tissue-stent interactions and design considerations. AJR Am J Roentgenol. 1993;160:613-8. [ ] 9. Caramoni PRA, Yamamoto GI, Zago AJ. Reestenose pós-angioplastia. Fisiopatogenia. Arq Bras Cardiol. 1997;69:141-8. [ ] 10. Leung DA, Spinosa DJ, Hagspiel KD, et al. Selection of stents for treating iliac arterial occlusive disease. J Vasc Interv Radiol. 2003;14(2 Pt 1):137-52. [ ] 11. Leon BM, Baim DS, Popma JJ, et al. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. Stent Anticoagulation Restenosis Study Investigators. N Engl J Med. 1998;339:1665-71. [ ] 12. Siegel S, Castellan NJ Jr. Nonparametric statistics for the behavioral sciences. 2nd ed. New York: McGraw-Hill; 1988. [ ] 13. Neter J, Kutner MH, Nachtsheim CJ, et al. Applied linear statistical models. 4th ed. Chicago: Times Mirror Higher Education Group, Inc.; 1996. [ ] 14. Tsetis D, Belli AM, Morgan R, et al. Preliminary experience with cutting balloon angioplasty for iliac artery in-stent restenosis. J Endovasc Ther. 2008;15:193-202. [ ] 15. Sheikh KH, Davidson CJ, Kisslo KB, et al. Comparison of intravascular ultrasound, external ultrasound and digital angiography for evaluation of peripheral artery dimensions and morphology. Am J Cardiol. 1991;67:817-22. [ ] 16. Kollum M, Hoefer I, Schreiber R, et al. Systemic application of anti-ICAM-1 monoclonal antibodies to prevent restenosis in rabbits: an anti-inflammatory strategy. Coron Artery Dis. 2007;18:117-23. [ ] 17. Tanous D, Bräsen JH, Choy K, et al. Probucol inhibits in-stent thrombosis and neointimal hyperplasia by promoting re-endotelialization. Atherosclerosis. 2006;189:342-9. [ ] 18. Sousa JEMR, Costa MA, Abizaid AC, et al. Lack of neointimal proliferation after implantation of sirolimus-coated stents in human coronary arteries: a quantitative coronary angiography and three-dimensional intravascular ultrasound study. Circulation. 2001;103:192-5. [ ] 19. Waksman R, Pakala R, Baffour R, et al. Optimal dosing and duration of oral everolimus to inhibit in-stent neointimal growth in rabbit iliac arteries. Cardiovasc Revasc Med. 2006;7:179-84. [ ] 20. Dolmatch B, Dong YH, Heeter Z. Evaluation of three polytetrafluoroethylene stent-grafts in a model of neointimal hyperplasia. J Vasc Interv Radiol. 2007;18:527-34. [ ] 21. Klein WM, van der Graaf Y, Seegers J, et al. Dutch iliac stent trial: long-term results in patients randomized for primary or selective stent placement. Radiology. 2005;238:734-44. [ ] Received March 15, 2008. * Study developed at Universidade Federal de São Paulo/Escola Paulista de Medicina (Unifesp/EPM), São Paulo, SP, and Instituto Dante Pazzanese de Cardiologia, São Paulo, SP, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554