Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 43 nº 3 - May / June of 2010
Vol. 43 nº 3 - May / June of 2010
|
CASE REPORT
|
|
Computed tomography and magnetic resonance imaging findings of os styloideum in a symptomatic athlete |
|
|
Autho(rs): André Francisco Gomes, Vinícius Chissini Paganella, Mateus Chissini Paganella, Caroline Schwartz Henkin, Giana Giostri |
|
|
Keywords: Os styloideum, Bone marrow edema, Magnetic resonance imaging |
|
|
Abstract:
ITitular Members of Colégio Brasileiro de Radiologia e Diagnóstico por Imagem (CBR), MDs, Radiologists, DAPI - Diagnóstico Avançado por Imagem, Curitiba, PR, Brazil
INTRODUCTION Os styloideum is an unmovable accessory ossicle located dorsally on the carpus, that represents an anatomic variant. It is located between the capitate and trapezoid bones, and between the second and third metacarpal bones. The association between the presence of os styloideum and wrist pain is known as carpal boss syndrome(1,2). Imaging methods are critical to achieve a correct diagnosis of this syndrome. In spite of the relevant role played by magnetic resonance imaging (MRI) in the differential diagnosis of symptomatic os styloideum, studies involving the use of this method for this purpose are still scarce in the literature(3,4). The authors present a case of symptomatic os styloideum evaluated with MRI, with a literature review on this finding.
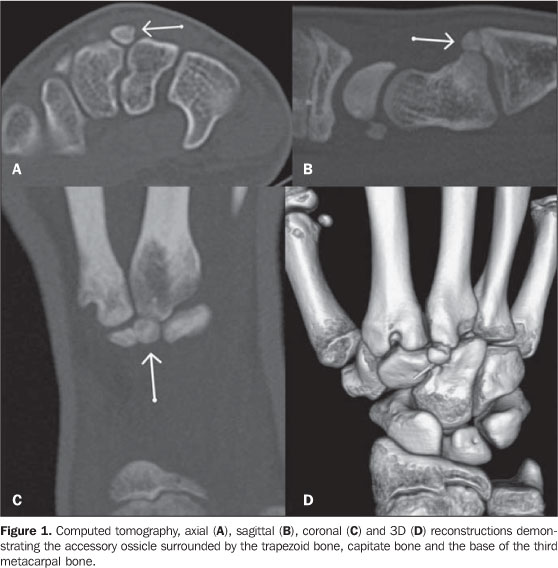
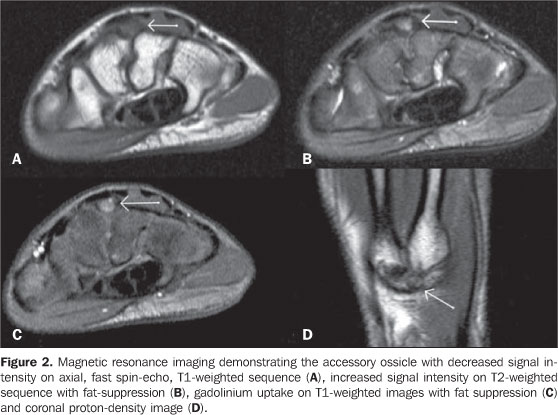
CASE REPORT A 14-year-old, white, female, semiprofessional tennis player coming from Curitiba, PR, Brazil, presented for an orthopedic consultation, complaining of wrist pain for more than one year, with symptoms worsening in the last month. Even with the symptoms exacerbation, the patient kept training, but utilizing the other wrist and experimented the onset of a subtle pain. At clinical-orthopedic examination of the wrists, there was a hard prominence, painful at palpation, on the base of the right third metacarpal bone, with a subtle soft tissue swelling. The patient reported a slight pain at the end of flexion and extension, although without limitation to the joint amplitude. The patient underwent computed tomography (CT) with multiplanar and 3D reconstruction which demonstrated the presence of an os styloideum on the dorsal region of the wrist (Figure 1). At MRI, a decrease in signal intensity on T1-weighted images, increase on T2-weighted images, and os styloideum signal enhancement after intravenous paramagnetic contrast (gadolinium) injection were observed, suggesting the presence of trabecular bone edema (Figure 2).
DISCUSSION Os styloideum, an accessory carpal ossicle, is included in a spectrum of conditions characterized by the presence of a bony protuberance at the base of the second and third metacarpal bones, constituting the carpal boss(5). Among the differential diagnoses, fracture of the base of the second and third metacarpal bones, osteophytes (osteoarthrosis), exostosis, bone and soft tissue neoplasias and cystic bony lesions are highlighted(3,5). According to Conway et al., os styloideum was firstly described in 1725 by Saltzmann(6), but the term carpal boss was proposed by Fiolle in 1931(7). The most plausible explanation for the etiology of os styloideum is based on the persistence of an accessory ossification center that emerges and, in most of cases, tends to disappear during the embryonic development. However, in cases where this abnormality persists, it may interfere with the biomechanics of the carpal joint. This condition may be found isolatedly (2%), fused with the capitates bone (3.5%) or with the trapezoid bone (0.5%), but, in most of times (94%) the os styloideum is fused with the base of the second and third metacarpal bones(3,5). Most of the chronic symptoms associated with the carpal boss may result from a bone degeneration process, inflamed ganglion, bursa or extensor tendon on the bony prominence. On the other hand, in cases of acute symptoms on the dorsal region of the wrist in association with trauma, one should suspect metacarpal base fracture, avulsion of the tendon of the extensor carpi radialis brevis, or os styloideum fracture(3,5). The clinical presentation is variable, with symptoms such as spontaneous pain or pain triggered by excessive use of the joint (racket sports or golf), subcutaneous edema and absence of joint blocking sensation. The pain may be aggravated by focal pressure and forced wrist extension, usually stopping with rest(5). Imaging methods play an essential role in the diagnosis of os styloideum. At radiography, lateral view of the wrist with the hand in flexion, supine at 30-40° and with 20-30° ulnar deviation has been described as the most appropriate one(5,8). However, pathological conditions associated with this accessory ossicle cannot be appropriately assessed with this imaging method. Bone scintigraphy has also been utilized, demonstrating an increase in radiotracer uptake (99mTc MDP) at the ossicle site(1,8). Multiplanar CT with three-dimensional reconstruction is useful in the evaluation of the relationship between the os styloideum and adjacent bones(8). However, in cases of acute, trauma-related pain or persistent pain, MRI is the most accurate imaging method to evaluate the integrity of metacarpal, carpal and accessory bones, as well as the bone marrow, enthesis and regional ligaments(3). In the reported case, the authors observed trabecular edema on the os styloideum, probably resulting from biomechanical changes with repeated traumas. The initial treatment of os styloideum consists of immobilization and administration of anti-inflammatory drugs. In patients with persistent pain, surgical excision, with or without arthrodesis, is usually indicated(1,3,6,8).
REFERENCES 1. Apple JS, Martinez S, Nunley JA. Painful os styloideum: bone scintigraphy in carpe bossu disease. AJR Am J Roentgenol. 1984;142:181-2. [ ] 2. Kalantari BN, Seeger LL, Motamedi K, et al. Accessory ossicles and sesamoid bones: spectrum of pathology and imaging evaluation. Appl Radiol. 2007;36:28-37. [ ] 3. Maquirriain J, Ghisi JP. Acute os styloideum injury in an elite athlete. Skeletal Radiol. 2006;35:394-6. [ ] 4. Zanetti M, Saupe N, Nagy L. Role of MR imaging in chronic wrist pain. Eur Radiol. 2007;17:927-38. [ ] 5. Park MJ, Namdari S, Weiss AP. The carpal boss: review of diagnosis and treatment. J Hand Surg Am. 2008;33:446-9. [ ] 6. Conway WF, Destouet JM, Gilula LA, et al. The carpal boss: an overview of radiographic evaluation. Radiology. 1985;156:29-31. [ ] 7. Fiolle J. Le "carpe bossu". Bull Mem Soc Natl Chir. 1931;57:1687-90. [ ] 8. Karmazyn B, Siddiqui AR. Painfull os styloideum in a child. Pediatr Radiol. 2002;32:370-2. [ ] Received June 25, 2008. * Study developed at Clínica DAPI - Diagnóstico Avançado por Imagem and Hospital Universitário Cajuru, Curitiba, PR, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554