Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 52 nº 4 - July / Aug. of 2019
Vol. 52 nº 4 - July / Aug. of 2019
|
LETTERS TO THE EDITOR
|
|
Primary essential cutis verticis gyrata |
|
|
Autho(rs): Isa Félix Adôrno1; Rômulo Florêncio Tristão Santos2; Thiago Franchi Nunes3; Gabriel Barbosa Sandim4; Edson Marchiori5 |
|
|
Dear Editor,
A 53-year-old woman was admitted to the emergency room with a three-day history of self-reported fever and diffuse headache. She reported no history of surgical interventions. On physical examination, her overall health status was satisfactory. However, a cutaneous mass, rich in sulci but without secretions, was observed in the right parietal region (Figure 1A). Computed tomography of the skull showed right-sided cutaneous thickening in the parietal, temporal, and occipital regions, with diffuse microcalcifications, mimicking the appearance of cerebral gyri. The cranial vault and cerebral parenchyma were unaffected (Figure 1B). Three-dimensional reconstruction provided a better view of the lesion and of its relationship with the cranial vault (Figure 1C). Collectively, those findings were consistent with a diagnosis of cutis verticis gyrata (CVG). Local scalp hygiene resulted in clinical improvement. The patient was discharged to outpatient treatment by the dermatology department of our institution. 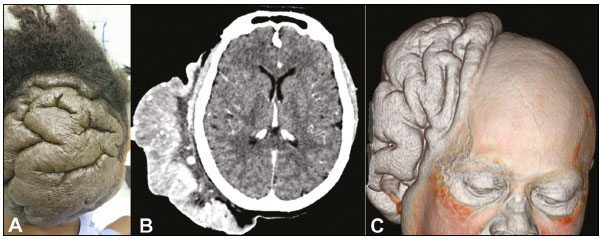 Figure 1. A: Photograph of the occipital region, showing a cerebriform cutaneous mass. B: Contrast-enhanced axial computed tomography of the skull, showing a lesion involving the subcutaneous tissue of the right parietooccipital region, with no signs of communication with the brain. C: Three-dimensional reconstruction providing a better view of the lesion and of its relationship with the cranial vault. CVG is a disease characterized by excessive growth of the skin of the scalp, resulting in the formation of sulci and gyri that resemble those of the cerebral cortex. The etiology of CVG is unknown. It is categorized as primary essential, primary non-essential, or secondary(1,2). The primary non-essential form, which accounts for 0.5% of cases, is associated with neurological manifestations such as microcephaly, intellectual disability, cerebral palsy, and epilepsy, as well as ophthalmological manifestations such as cataracts and blindness(1,3). The primary essential form is not associated with neurological or ophthalmological alterations, presenting only as scalp folds, which mimic the cerebral gyri, and predominantly affects men; it typically appears during or after puberty, 90% of patients being diagnosed after 30 years of age(1,3,4). The secondary form, which can occur at any age, affects men and women with similar frequency; the clinical presentation varies depending on the underlying cause, such causes including cerebriform intradermal nevus, inflammatory dermatoses, endocrine diseases, and genetic syndromes(2,5). Typically, the scalp folds and furrows seen in CVG show a disordered pattern, with an asymmetric distribution. An appropriate investigation includes histopathological analysis to determine the etiology. Although the affected area is asymptomatic, there can be accumulation of secretions, causing odor and itching; therefore, good scalp hygiene is important for symptom relief. When secondary to other etiologies, CVG usually regresses after treatment of the underlying disease, although surgical excision may be necessary in this or any of the forms of presentation(1,4,6). REFERENCES 1. Schenato LK, Gil T, Carvalho LA, et al. Cutis verticis gyrata primária essencial. J Pediatr. 2002;78:7580. 2. Tucci A, Pezzani L, Scuvera G, et al. Is cutis verticis gyrata-intellectual disability syndrome an underdiagnosed condition? A case report and review of 62 cases. Am J Med Genet Part A. 2016;173(A):63846. 3. Chang GY. Cutis verticis gyrata, underrecognized neurocutaneous syndrome. Neurology. 1996;47:5735. 4. Garden JM, Robinson JK. Essential primary cutis verticis gyrata: treatment with the scalp reduction procedure. Arch Dermatol. 1984;120:14803. 5. Dumas P, Chardon VM, Balaguer T, et al. Cutis verticis gyrata primitif essentiel: cas clinique et revue de la littérature. Ann Chir Plast Esthet. 2009;55:2438. 6. Walia R, Bhansali Anil. Cutis verticis gyrata. BJM Case Reports. 2011; 10.1136. 1. Universidade Federal de Mato Grosso do Sul (UFMS), Campo Grande, MS, Brazil; https://orcid.org/0000-0002-2106-1211 2. Universidade Federal de Mato Grosso do Sul (UFMS), Campo Grande, MS, Brazil; https://orcid.org/0000-0002-8679-7369 3. Universidade Federal de Mato Grosso do Sul (UFMS), Campo Grande, MS, Brazil; https://orcid.org/0000-0003-0006-3725 4. Universidade Federal de Mato Grosso do Sul (UFMS), Campo Grande, MS, Brazil; https://orcid.org/0000-0002-8427-1275 5. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil; https://orcid.org/0000-0001-8797-7380 Correspondence: Dr. Thiago Franchi Nunes Avenida Senador Filinto Müller, 355, Vila Ipiranga Campo Grande, MS, Brazil, 79080-190 Email: thiagofranchinunes@ gmail.com Received 12 November 2017 Accepted after revision 11 December 2017 |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554