Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 50 nº 5 - Sep. / Oct. of 2017
Vol. 50 nº 5 - Sep. / Oct. of 2017
|
LETTER TO THE EDITOR
|
|
Tersons syndrome: an important differential diagnosis of subarachnoid hemorrhage |
|
|
Autho(rs): Ana Paula Alves Fonseca; Marcos Rosa Júnior |
|
|
Dear Editor,
A 42-year-old female patient presented to the emergency room with severe headache and hypertensive urgency (blood pressure, 220/110 mmHg), progressing to left hemiparesis, right anisocoria, and a decreased level of consciousness, with a Glasgow Coma Scale score of 4. Computed tomography (CT) of the brain showed acute subarachnoid hemorrhage (Fisher grade 4), due to rupture of an aneurysm in the anterior circulation, together with signs of bilateral intraocular hemorrhage (Figure 1). Those findings are consistent with a diagnosis of Tersons syndrome. 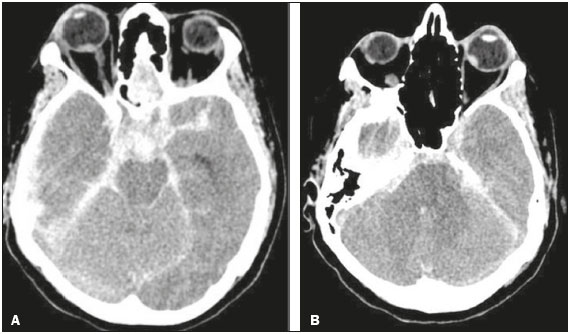 Figure 1. A: CT scan showing signs of subarachnoid hemorrhage and right intraocular hemorrhage, as a spontaneously hyperattenuating focus in the posterior portion of the right globe. B: CT scan showing left intraocular hemorrhage. Tersons syndrome was initially described as vitreous hemorrhage secondary to acute subarachnoid hemorrhage, although recent studies have shown that it can also result from traumatic brain injury or even nontraumatic intracerebral hemorrhage(1). Originally described in 1900 by Albert Terson, the syndrome has an incidence of 2.627.0% in the context of subarachnoid hemorrhage due to a ruptured aneurysm(2-4). Although the etiology of the syndrome is controversial, it has been attributed to a rapid increase in venous or intracranial pressure, which causes rupture of the peripapillary capillaries of the retina or results in compression of the central retinal vein, thus decreasing retinal venous drainage, promoting stasis, and provoking hemorrhage(5). The diagnosis of intraocular hemorrhage is more accurately confirmed by ophthalmoscopy, although CT can suggest it, with an estimated sensitivity of 66%. The changes seen most frequently are retinal thickening and hyperattenuating nodules overlying the optic disc(6). Tersons syndrome most often occurs in patients with severe neurological disease, a Glasgow Coma Scale £ 8, and aneurysmal subarachnoid hemorrhage with a Fisher score ³ 3 at presentation. It is also of note that the rates of morbidity and mortality are high among such patients. In the sample studied by Fountas et al.(7), the mortality was 28.6% among the patients with intraocular hemorrhage, compared with only 2.0% among those without. Tersons syndrome is not an uncommon condition, perhaps being underdiagnosed. Given the prognostic implications of this diagnosis for morbidity and mortality, as well as the potential for secondary ocular lesion, it is of extreme relevance to radiologists and other medical professionals, especially in the context of acute subarachnoid hemorrhage(8) but also in other forms of intracranial hemorrhage. REFERENCES 1. Czorlich P, Skevas C, Knospe V, et al. Terson syndrome in subarachnoid hemorrhage, intracerebral hemorrhage, and traumatic brain injury. Neurosurg Rev. 2015;38:129-36. 2. de Vries-Knoppert W. Vitreous findings in a patient with Terson''s syndrome. Doc Ophthalmol. 1995;90:75-80. 3. Vanderlinden RG, Chisholm LD. Vitreous hemorrhages and sudden increased intracranial pressure. J Neurosurg. 1974;41:167-76. 4. Pobereskin LH. Incidence and outcome of subarachnoid haemorrhage: a retrospective population based study. J Neurol Neurosurg Psychiatry. 2001;70:340-3. 5. Ogawa T, Kitaoaka T, Dake Y, et al. Terson syndrome: a case report suggesting the mechanism of vitreous hemorrhage. Ophthalmology. 2001;108: 1654-6. 6. Avila M, Cialdini AP, Crivelin M, et al. Vitrectomia na síndrome de Terson. Arq Bras Oftalmol. 1997;60:67-71. 7. Fountas KN, Kapsalaki EZ, Lee GP, et al. Terson hemorrhage in patients suffering aneurysmal subarachnoid hemorrhage: predisposing factors and prognostic significance. J Neurosurg. 2008;109:439-44. 8. Wajnberg E. Síndrome de takotsubo após hemorragia subaracnóidea. Radiol Bras. 2012;45:132-4. Hospital Universitário Cassiano Antônio Morais da Universidade Federal do Espírito Santo (HUCAM-UFES), Vitória, ES, Brazil. Mailing address: Dra. Ana Paula Alves Fonseca Rua Major Clarindo Fundão, 110, ap. 604, Praia do Canto Vitória, ES, Brazil, 29055-655 E-mail: anapaf.fonseca@gmail.com |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554