Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 48 nº 3 - May / June of 2015
Vol. 48 nº 3 - May / June of 2015
|
LETTER TO THE EDITOR
|
|
Acute post-tonsillectomy negative pressure pulmonary edema |
|
|
Autho(rs): Lais Bastos Pessanha; Adriana Maria Fonseca de Melo; Flavia Silva Braga; Gabriel Antonio de Oliveira; Livia Guidoni de Assis Barbosa; Antonio Roberto Carrareto |
|
|
Dear Editor,
A female, 28-year patient was submitted to tonsillectomy and developed respiratory discomfort immediately after the procedure. At the following day, posteroanterior and lateral chest radiography demonstrated coalescent, poorly defined opacities in both lungs, sparing the periphery and characterizing the so called "butterfly wing" pattern, compatible with a diffuse alveolar process. The cardiac image was normal (Figure 1A). Three days after the procedure, without any use of medication, radiographic images (same views) revealed the opacities disappearance (Figure 1B). 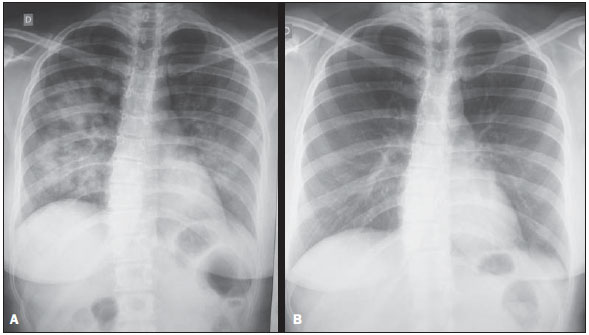 Figure 1. A: Posteroanterior chest radiographic image showing bilateral, coalescent, poorly defined opacities, characterizing the so called "butterfly wing" pattern, which is typical of alveolar process. The cardiac image is normal. These images were acquired on the following day after tonsillectomy. The patient presented with mild dyspnea. B: Posteroanterior chest radiographic image acquired three days after the procedure. Complete resolution of the alveolar process demonstrated on the previous images. Negative pressure pulmonary edema (NPPE) represents a rare occurrence in surgeries (0.094%), most frequently reported in buccomaxillary-facial and oral surgeries due to the probability of upper airway obstruction(1-3). This condition is divided into two classes, namely, type I NPPE caused by upper airway obstruction such as, for example, post-tracheal extubation laryngospasm, epiglotiditis, tracheal cannula obstruction and postoperative vocal cord paralysis(3-6). Type II NPPE occurs after corrective surgical procedures for chronic airway obstruction such as tonsillar hyperplasia, sleep apnea, tumors and acromegaly(7,8). In such cases, the treatment should be aimed at reverting hypoxia and decreasing the pulmonary fluid volume(1-5). The prognosis is good, with recovery at the first 24 hours.(8). Radiographic and chest CT findings of NPPE include interstitial edema progressing to alveolar edema in more severe cases. Generally, regression of symptoms and radiological finding is observed within two or three days(6). Many diseases present with radiological sings of diffuse alveolar process but this is not a specific finding in any of them(9). In the present case, the patient was healthy, with no comorbidity at the immediate postoperative period following upper airway surgery (tonsillectomy), presenting spontaneous resolution in only three days. Despite the nonspecificity of the radiological pattern, the preoperative history of the patient and the prompt resolution allowed for ruling out other causes, and NPPE was the only remaining possible diagnosis. Thus, the authors considered to be unnecessary to proceed with the diagnostic investigation with other imaging methods and laboratory tests. REFERENCES 1. Cascade PN, Alexander GD, Mackie DS. Negative-pressure pulmonary edema after endotracheal intubation. Radiology. 1993;186:671-5. 2. Mamiya H, Ichinohe T, Kaneko Y. Negative pressure pulmonary edema after oral and maxillofacial surgery. Anesth Prog. 2009;56:49-52. 3. Deepika K, Kenaan CA, Barrocas AM, et al. Negative pressure pulmonary edema after acute upper airway obstruction. J Clin Anesth. 1997;9:403-8. 4. Davidson S, Guinn C, Gacharna D. Diagnosis and treatment of negative pressure pulmonary edema in a pediatric patient: a case report. AANA J. 2004;72:3378. 5. Timby J, Reed C, Zeilender S, et al. "Mechanical" causes of pulmonary edema. Chest. 1990;98;9739. 6. Sulek C. Negative-pressure pulmonary edema. In: Gravenstein N, Kirby RR, editors. Complications in anesthesiology. 2nd ed. Philadelphia, PA: Lippincott-Raven; 1996. p. 1917. 7. Hobaika ABS, Lorentz MN. Laringoespasmo. Rev Bras Anestesiol. 2009;59:48795. 8. Albergaria VF, Soares CM, Araújo RM, et al. Edema pulmonar por pressão negativa após hipofisectomia transesfenoidal. Relato de caso. Rev Bras Anestesiol. 2008;58:3916. 9. Felson B. Disseminated interstitial diseases of the lung. Ann Radiol. 1966;9:32545. Universidade Federal do Espírito Santo (UFES), Vitória, ES, Brazil Mailing Address: Dra. Lais Bastos Pessanha Rua Primeiro de Maio, 79, Centro Campos dos Goytacazes, RJ, Brazil, 28035-145 E-mail: laispessanha@hotmail.com |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554