Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 48 nº 3 - May / June of 2015
Vol. 48 nº 3 - May / June of 2015
|
LETTER TO THE EDITOR
|
|
Gastric Kaposi's sarcoma |
|
|
Autho(rs): Veluma Lopes Teixeira; Pedro José de Santana Júnior; Kim-Ir-Sen Santos Teixeira; Daniella Carneiro; Marise Moreira; Gabriela Moura Paula |
|
|
Dear Editor,
A male, 29-year-old, homosexual patient presenting with history of 20 kg-weight loss, asthenia, nausea and stomach pain for three months in association with appearance of skin lesions in upper limbs and scrotal sac. Human immunodeficiency virus (HIV) serology was positive. Double contrast radiological study of the stomach (Figure 1A) demonstrated polypoid lesions. At abdominal computed tomography (Figures 1B and 1C), solid, polypoid nodular masses were observed on the gastric submucosa with endoluminal component and early contrast-enhancement. High digestive endoscopy (Figure 1D) demonstrated erythematous lesions, some of them being violaceous, polypoid and flat, with a normal gastric submucosa. On that occasion, biopsy of the skin lesions and of the lesions in the stomach revealed atypical vascular lesion, and the anatomopathological and immunohistochemical analyses confirmed the diagnosis of Kaposi's sarcoma. 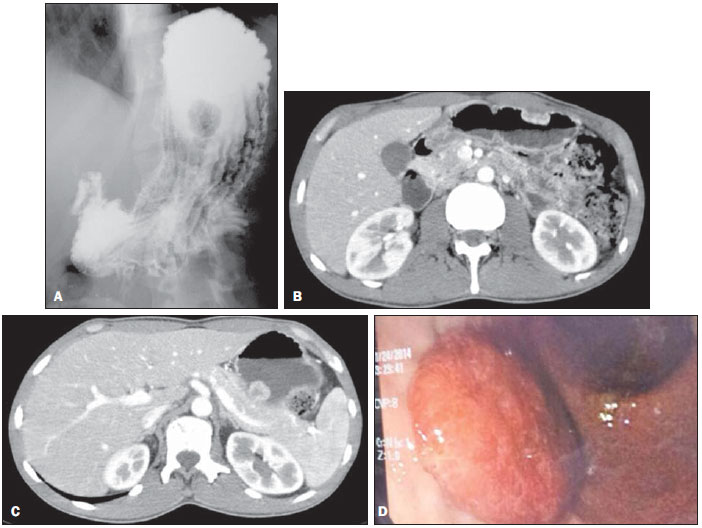 Figure 1. A: Radiographic image of esophagus, stomach and duodenum shows polypoid filling defect. B,C: Abdominal CT arterial phase shows subepithelial hypervascular polypoid lesions. D: High digestive endoscopy shows the corresponding reddish polypoid lesion. The compromise of the gastrointestinal tract by Kaposi's sarcoma is the most common form of disseminated disease, observed in up to 50% of patients. The disease can involve from the oropharynx to the rectum, and the duodenum is most frequently affected, followed by the stomach, esophagus and colon(1,2). Kaposi's sarcoma is about 300 times more common in AIDS patients than in those with other immunodeficiency types, and generally occurs in the setting of CD4 count below 150-200 cells/mm3(1). The diagnosis is made by means of digestive endoscopy and biopsy. The classical endoscopic finding is represented by subepithelial, reddish, ulcerative or non-ulcerative lesions(3). Barium studies characterize polypoid lesions with smooth contour with sizes ranging from few millimeters to 3 cm. Larger lesions may ulcerate, giving the lesion a "bullseye" or "target" pattern(4). Computed tomography detects subepithelial polypoid lesions or irregular thickening of gastric folds, which after intravenous contrast injection show hypervascular behavior, with a more marked enhancement than that of the adjacent mucosa in the arterial phase due to the intense vascularization of the tumor. Additionally, peripancreatic lymph node enlargement may be observed in the porta hepatis, mesenterium and retroperitoneum in up 80% of cases(1,3). Kaposi's sarcoma with visceral involvement is frequently associated with poor prognosis. The treatment includes antiretroviral therapy, radiotherapy, and chemotherapy(5). The authors conclude that Kaposi's sarcoma should be considered in the differential diagnosis of hypervascular submucosal lesions, particularly in AIDS patients. REFERENCES 1. Restrepo CS, Martinez S, Lemos JA, et al. Imaging manifestations of Kaposi sarcoma. Radiographics. 2006;26:116985. 2. Arora M, Goldberg EM. Kaposi sarcoma involving the gastrointestinal tract. Gastroenterol Hepatol. 2010;6:45962. 3. Lee NK, Kim S, Kim GH, et al. Hypervascular subepithelial gastrointestinal masses: CT-pathologic correlation. Radiographics. 2010;30:191534. 4. Rose HS, Balthazar EJ, Megibow AL, et al. Alimentary tract involvement in Kaposi sarcoma: radiographic and endoscopic findings in 25 homosexual men. AJR Am J Roentgenol. 1982;139:6616. 5. Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:28994. Hospital das Clínicas da Universidade Federal de Goiás (UFG), Goiânia, GO, Brazil Mailing Address: Dr. Pedro José de Santana Júnior Departamento de Radiologia Avenida Primeira Avenida, s/nº, Setor Leste Universitário Goiânia, GO, Brazil, 74605-020 E-mail: pedrojosesantanajr@hotmail.com |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554