Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 47 nº 4 - July / Aug. of 2014
Vol. 47 nº 4 - July / Aug. of 2014
|
ICONOGRAPHIC ESSAY
|
|
Intraventricular mass lesions at magnetic resonance imaging: iconographic essay part 2 |
|
|
Autho(rs): Felipe Damásio de Castro1; Fabiano Reis2; José Guilherme Giocondo Guerra3 |
|
|
Keywords: Neoplasms; Cerebral ventricle neoplasms; Central nervous system; Magnetic resonance imaging. |
|
|
Abstract: INTRODUCTION
Intraventricular tumors represent a subgroup of intracranial lesions with typical and unique features, which can be considered apart from the classical subdivisions into intraand extra-axial tumors(1). Although they are easily visualized, the differential diagnosis among lesions may be difficult without the knowledge of the types of tissues which originate such tumors(2). The ventricles are surrounded by a layer of ependymal cells and a subependymal plate formed by glial cells. Such layers give origin to ependymomas, subependymomas and subependymal giant cell astrocytomas. Such a lining and the septum pellucidum that is located between the corpus callosum and the fornix, separating the lateral ventricles, also give origin to the central neurocytoma, a unique glial neuronal tumor of the ventricular systems(2). The choroid plexus is the most vascularized portion of the ventricular system and produces the cerebrospinal fluid. Primary neoplasms of this tissue are highly vascularized and are commonly associated with hydrocephalus due to increased production of cerebrospinal fluid. Such lesions occur in a benign form, the choroid plexus papilloma, and less frequently in a malignant presentation, the choroid plexus carcinoma. Tumors such as meningiomas and metastases may also occur in this location. Masses are more frequently found in the posterior portion of the lateral ventricles(2), but their location may vary according to the type of tumor. Choroid plexus papillomas occur mainly in children, with predilection for the lateral ventricles in this age range, while in adults it is usually more frequently found in the fourth ventricle. Ependymomas occur more frequently in the posterior fossa in children, and in adults they are generally supratentorial. Many times, inflammatory/infectious lesions are observed within the ventricular system and among them neurocysticercosis is very common in Brazil. Other less frequent conditions, such as histoplasmosis, may also be observed. In the present essay, the authors have gathered images obtained over the past 15 years at the Radiology Service of Hospital de Clínicas Universidade Estadual de Campinas, São Paulo, Brazil. The study was duly approved by the Committee for Ethics in Research of the Institution. RADIOLOGICAL FINDINGS Colloid cyst It is a benign lesion that usually develops in the anterosuperior aspect of the third ventricle, adjacent to the Monro's foramen(1) and is the most common lesion in this region(3). They are rounded-shaped or ovoid lesions, with smooth walls, and may be associated with obstructive hydrocephalus, either intermittent or not. At computed tomography (CT), the cysts may be either iso- or hyperdense, with no contrast uptake, or with peripheral contrast uptake. At magnetic resonance imaging (MRI) (Figure 1) the signal intensity is variable, depending upon the contents of the cyst(3), with hyper-or isosignal on T1-weighted sequences, as compared with the cerebrospinal fluid; and with hypo- to hypersignal on T2-weighted sequences, with mixed signal in some cases(1). 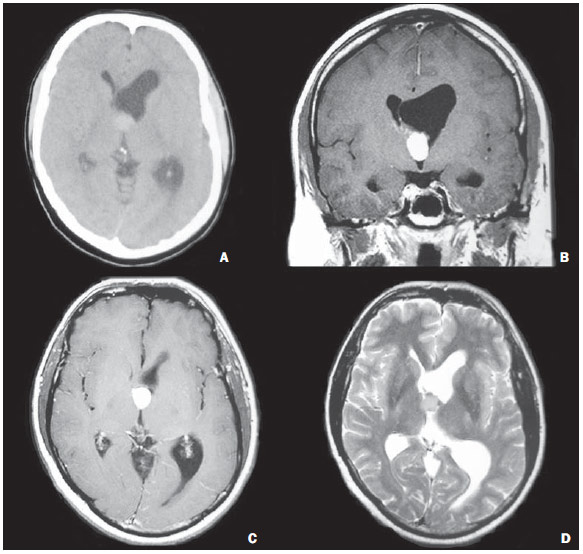 Figure 1. A male, 36-year-old patient. Non contrast-enhanced axial CT image (A) showing spontaneously hyperdense lesion located in the Monro´s foramen and in the anterior portion of the third ventricle, determining left lateral ventricle ectasia. Coronal (B) MRI and contrast-enhanced, axial T1-weighted image (C) demonstrate the presence of a solid lesion with no apparent contrast uptake. On axial T2-weighted images (D) the lesion presents with isosignal. anatomopathological study revealed colloid cyst. Oligodendroglioma Oligodendrogliomas manifest as well defined, round-shaped or ovoid masses involving the cortex or the subcortical white matter. At intraventricular location, they are adjacent to the septum pellucidum and present imaging and pathological features very similar to those of central neurocytoma, and are differentiated only at immunohistochemical study. At CT, they may be hypodense, isodense and even hyperdense. Calcifications are observed in 2091% of cases. Cystic or hemorrhagic degeneration may be found. MRI is superior to CT in the evaluation of tumor extent, and the tumor usually is hypointense in relation to the gray matter on T1-weighted sequences and hyperintense on T2-weighted sequences. Heterogeneity of signal intensity is the rule (Figure 2)(1,2). 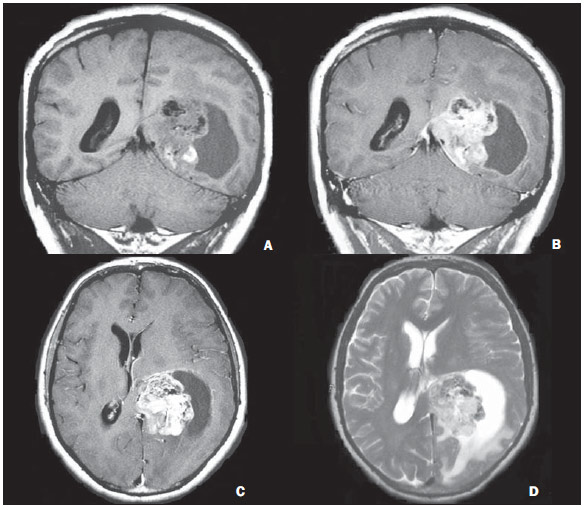 Figure 2. A male, 31-year-old patient. Coronal MRI T1-weighted sequence (A) shows a heterogeneous solid, cystic lesion, with low signal intensity, with some hypersignal foci (hemorrhage) and hyposignal (calcifications) located in the left lateral ventricle. On the contrast-enhanced T1-weighted sequence (B,C) there is intense uptake in the solid portion. On the T2-weighted sequence (D), the lesion presents with hypersignal. There are signs of extension/infiltration of the adjacent encephalic parenchyma. Biopsy revealed oligodendroglioma. Astroblastoma It is a rare tumor, which usually presents as a large peripheral supratentorial tumor. At MRI (Figure 3), they are solid-cystic tumors with a characteristic bubbly feature of the solid component and isosignal on T2-weighted sequences. One observes a mild perilesional hypersignal, disproportionate to the tumor size(4). 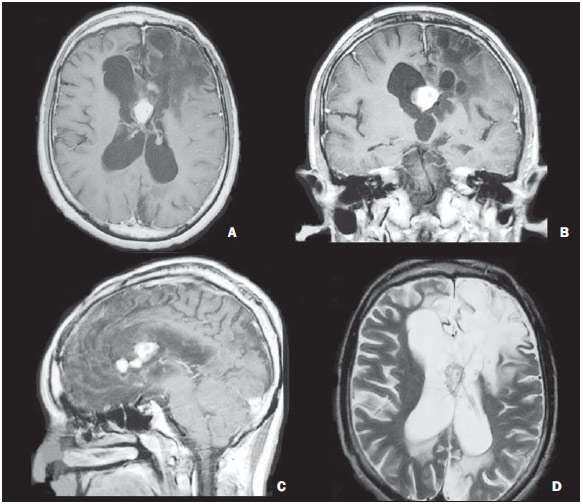 Figure 3. A male, 12-year-old patient. Contrast-enhanced, axial MRI, T1-weighted sequence (A) reveals the presence of a solid lesion, with no sign of necrosis, located in the septum pellucidum with intense contrast uptake (B,C). On the T2-weighted sequence (D), the lesion presents with isosignal and extensive signal change involving the adjacent encephalic parenchyma. In spite of the atypical imaging pattern in relation to that described in the literature, the biopsy revealed astroblastoma. Lipoma Intracranial lipoma is a rare congenital malformation that more commonly occurs in the pericallosal region. At images, they are identified as well defined lobulated lesions, with fat density/intensity, located on the medial line. At CT, such tumors present as lesions with fat density (50 to 100 UH), sometimes with calcifications, mainly the tubulonodular type, with no contrast uptake. At MRI, they present with hypersignal on T1-weighted sequences, with signal intensity drop on T1-weighted sequences with fat suppression, and hyposignal on T2-weighted sequences(5) due to striking chemical shift artifact (Figure 4). 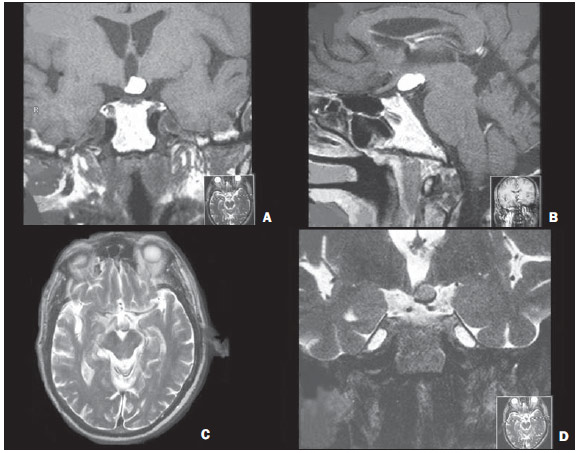 Figure 4. A male, 70-year-old patient. Coronal MRI, T1-weighted sequence (A) shows a solid lesion with hypersignal on T1-weighted sequence, located on the floor of the third ventricle, with no contrast enhancement (B). On axial (C) and coronal (D) T2-weighted sequences, the lesion presents with hyposignal. The imaging findings are compatible with lipoma. Cavernoma Also named cavernous malformation or cavernous angioma, it is a congenital or acquired vascular abnormality that occurs in 0.5% of the general population. More rarely they may be intraventricularly located. Classically, cavernomas are found on T2-weighted images as popcorn ball-like lesions with a hyposignal halo due to hemosiderin deposition. Subacute hemorrhage and blood degradation products produce a hypersignal halo on T1-weightes sequences, a finding that helps in the differentiation from hemorrhagic tumors and other intracranial hemorrhages (Figure 5). At CT, such malformations are seen as hyperdense, well delimited lesions, with calcifications in 40%-60% of the cases, with no contrast uptake(5). 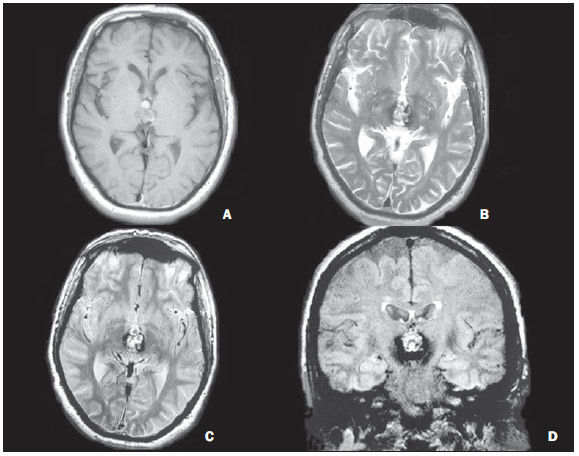 Figure 5. A male, 60-year-old patient. Axial MRI, T1-weighted sequence (A) demonstrates the presence of a heterogeneous solid lesion, with focal areas of globuliform hypersignal located in the third ventricle. On T2-weighted sequence (B) a hyposignal halo is observed surrounding the lesion that is also demonstrated on the DP and FLAIR sequences (C,D). Anatomopathological analysis was not performed but the lesion is a typical cavernoma. Neurocysticercosis Intraventricular neurocysticercosis corresponds to 0.733% of all cases, with a predilection for the fourth ventricle (50%), followed by the lateral ventricles (35%), third ventricle (10%) and aqueduct (5%). It generally causes obstructive hydrocephalus because of ventriculitis caused by ependymal inflammatory response or adhesions(6). Neurocysticercosis is seen at CT as a cystic lesion that is initially isodense in relation to the cerebrospinal fluid, and therefore are not clearly visualized. It may be associated with asymmetries in the ventricular system or ventricular dilatation. On the other hand, at MRI (Figure 6), the cysts are well defined, due to signal intensity subtly different from that of the cerebrospinal fluid at T1- and T2-weighted images. However, the cysts may appear isodense in relation to the cerebrospinal fluid and, in such cases, 3D CISS sequences are very useful in the characterization of the cysts and scolex demonstration(6). Depending upon their dimensions, neurocysticercosis can exert considerable expansile effect on the compartments where the lesions are located. 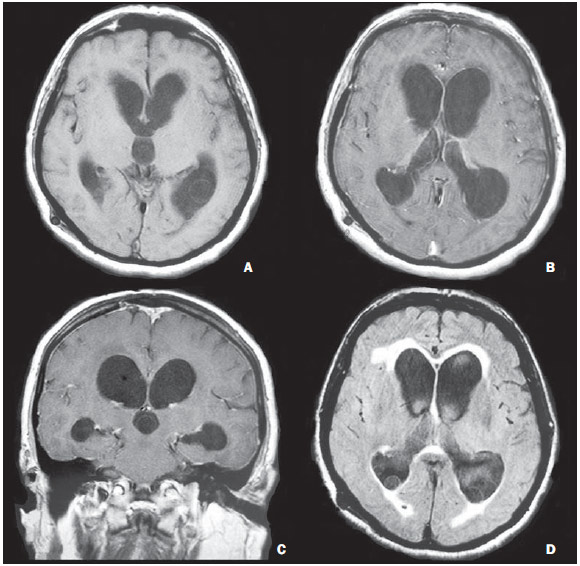 Figure 6. A male, 67-year-old patient. Axial MRI T1-weighted sequence (A) demonstrating the presence of cystic lesions with isosignal in relation to the cerebrospinal fluid, with isointense walls in relation to the brain cortex, with no contrast uptake (B,C), located in the posterior horns and in the third ventricle. The lesions are more clearly identified at axial MRI FLAIR sequence (D). Ventricular derivation is observed. Cerebrospinal fluid analysis was positive for anti-cysticercus antibodies, confirming the diagnosis of neurocysticercosis. Histoplasmosis Disseminated histoplasmosis refers to multiple organs infection by the Histoplasma capsulatum fungus. The most common sites of involvement are the skin, respiratory and intestinal tracts. Central nervous system involvement is a rare complication that generally manifests as meningitis, typically occurring in immunosuppressed patients and in extreme age groups(7). Imaging findings (Figure 7) are nonspecific and the diagnostic hypothesis of histoplasmosis should be raised for patients with signs of meningitis or cerebritis at MRI studies(7). Also, single or multiple granulomas may be found, usually isointense on T1-weighted and hypointense on T2-weighted sequences, with homogeneous enhancement after intravenous contrast medium injection. Granulomas, as in the present case, may be located inside the ventricular system. 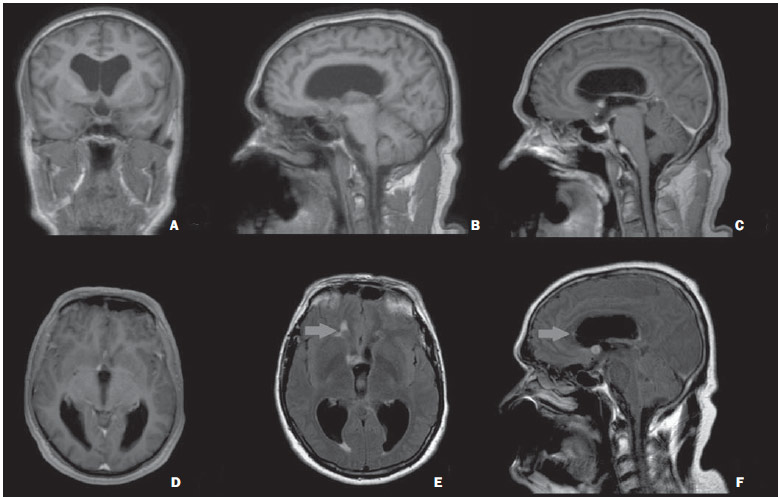 Figure 7. A male, 54-year-old patient. Coronal (A) and sagittal (B) MRI T1-weighted sequence demonstrating the presence of homogeneous, solid nodular lesions with isosignal in relation to the cerebral parenchyma, located in the right Monro's foramen, with intense contrast enhancement (C,D). On the FLAIR sequences, a lesion with similar characteristics is highlighted in the anterior horn of the right lateral ventricle (arrows on E,F). Necropsy revealed histoplasmosis granulomas. CONCLUSION Intraventricular mass lesions have a wide variety of presentations at imaging studies, which may be a consequence of the different types of tissues found in the central nervous system, involved in the development of such lesions. Therefore, the study of the skull, particularly by MRI, plays a relevant role in the attempt to define differential diagnoses based on their location, signal characteristics on the different sequences, as well as in the detection of hemorrhage elements and calcifications. In the present study, the authors have aimed at reviewing the main intraventricular lesions approaching from the most common ones to those more rarely found (particularly those of inflammatory/infectious etiology), which can, however, be included in the differential diagnosis. REFERENCES 1. Leite CC, Sequeiros IM, Lacerda MTC, et al. Tumores intraventriculares: achados à ressonância magnética. Rev Imagem. 2001;23:7385. 2. Koeller KK, Sandberg GD; Armed Forces Institute of Pathology. From the archives of the AFIP. Cerebral intraventricular neoplasms: radiologic-pathologic correlation. Radiographics. 2002;22:1473505. 3. Tien RD. Intraventricular mass lesions of the brain: CT and MR findings. AJR Am J Roentgenol. 1991;157:128390. 4. Port JD, Brat DJ, Burger PC, et al. Astroblastoma: radiologic-pathologic correlation and distinction from ependimoma. AJNR Am J Neuroradiol. 2002;23:2437. 5. Osborn AG. Neuroglial cyst. In: Osborn AG, Salzman KL, Katzman G, et al, editors. Diagnostic imaging brain. 1st ed. Salt Lake City: Amirsys; 2004. p. 720. 6. Kimura-Hayama ET, Higuera JA, Corona-Cedillo R, et al. Neurocysticercosis: radiologic-pathologic correlation. Radiographics. 2010;30:170519. 7. Zalduondo FM, Provenzale JM, Hulette C, et al. Meningitis, vasculitis, and cerebritis caused by CNS histoplasmosis: radiologic-pathologic correlation. AJR Am J Roentgenol. 1996;166:1946. 1. MD, Resident of Radiology and Imaging Diagnosis at Hospital de Clínicas Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil 2. PhD, Docent responsible for the Division of Neuroradiology, Professor, Department of Radiology, Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil 3. Graduate Student of Medicine, School of Medical Sciences, Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil Mailing Address: Dr. Fabiano Reis Faculdade de Ciências Médicas Universidade Estadual de Campinas, Departamento de Radiologia Rua Tessália Vieira de Camargo, 126, Cidade Universitária Zeferino Vaz Campinas, SP, Brazil, 13083-887. Caixa Postal: 6111 E-mail: fdamasiocastro@gmail.com Received March 3, 2013. Accepted after revision September 9, 2013. Study developed at Hospital de Clínicas Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554