Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 47 nº 3 - May / June of 2014
Vol. 47 nº 3 - May / June of 2014
|
ORIGINAL ARTICLE
|
|
SUS in nuclear medicine in Brazil: analysis and comparison of data provided by Datasus and CNEN |
|
|
Autho(rs): Lorena Pozzo1; George Coura Filho2; João Alberto Osso Júnior3; Peterson Lima Squair4 |
|
|
Keywords: SUS; Nuclear medicine; Gamma camera. |
|
|
Abstract: INTRODUCTION
Created in 1988 by the Constitution of the Federative Republic of Brazil, the Unified Health System (SUS) is under constant improvement. It is a health system whose principle is based on access universality, equity and integral care(1). The system is understood as being a single system as it follows the same fundamentals and organizational principles throughout the entire Brazilian territory under the responsibility of autonomous government spheres at federal, State and municipal levels. It comprises units, services and actions with a common purpose. The SUS follows principles of regionalization and hierarchization, i.e., the services must be organized at crescent levels of technological complexity, within a delimited geographic area, and with the definition of the targeted population. It also follows the principles of resolubility, decentralization, citizens' participation and complementarity with the private sector. As regards the latter, the Brazilian Constitution defines that the private sector can become a part of SUS, as agreed and contracted, provided that SUS rules and regulations are followed by such entities. Additionally, among the private services, preference must be given to philanthropic and nonprofit entities. It is important to remember that according to Law No. 8.080 dated 1990, Chapter 2, Article26, Paragraph 4 establishes that "owners, managers and directors of contracted services are forbidden to serve in leadership or commissioned positions at SUS". In order to meet the above mentioned principles, for the decentralization of healthcare activities and feasibility of social control on the utilization of available resources, the Informatics on Health Department - Datasus was created. In 2011 it became a part of the Secretary of Strategic and Participative Management of the Health Ministry. The Outpatient Data System of Datasus (SIA/SUS) is a computer system whose forms are mandatorily filled out and input by all managers with public or private services under their responsibility. The SIA/SUS comprises data on the number of outpatient procedures that were performed under SUS coverage, either at the public or at the private network. The outpatient procedures are structured into groups, subgroups and organization levels. In their processing, other databanks are utilized such as the case of the National Register of Health Services (CNES), besides the SIA/SUS Procedures Table(2). The data from CNES, created by the Ordinance MS/SAS 376, dated October 3, 2000, comprise the knowledge on the health services with information such as physical area, human resources, equipment, hospital and outpatient services. It covers all hospitals in the country, as well as all outpatient services either connected or not connected with SUS. The CNES is one of the databases utilized by the SIA and by the Hospital Data System (SIH), and the responsibility for including services by means of the Health Service Registration Form (FCES), data updating and maintenance lies with the State or municipal managers. It is even possible to investigate the number of connections of an individual health professional with SUS-accredited health services. Nuclear medicine Nuclear medicine is a medical specialty whose main characteristic is the utilization of unsealed ionizing radiation sources. Those must be linked to molecules of biological interest, composing substances called radiopharmaceuticals which are administered to patients for diagnostic or therapeutic purposes. If the utilized radionuclide is an emitter of electromagnetic radiation (gamma) or positrons, it is possible to map the distribution of the material within the patient's body with an external detector called gamma camera or a positron emission tomography (PET) apparatus. If the utilized radionuclide is a beta particle emitter, such as 131I, it is possible to perform specific therapies for many types of tumors. In some cases it is also possible do detect the braking radiation of such particles in order to compose an image acquired with a gamma camera for therapy followup, for example. A multi- and interdisciplinary team including physicians, technologists or biomedical technicians, medical physicists, radiopharmacists and a nursing team trained for working with unsealed radiation sources is required for the application of such a technique. Nuclear medicine procedures, as well as magnetic resonance imaging and x-ray computed tomography, are classified by SUS as high-complexity procedures, i.e, procedures involving high technology and high costs. The unified table of procedures comprises only 50 outpatient procedures based on the utilization of 99mTc and primary radioisotopes (131I, 67Ga, 201Tl) sources. However, the specialty currently utilizes positron emitters with very short half-lives, such as 18F, besides particle emitting radioisotopes such as 177Lu for therapeutic purposes, which are not yet contemplated by SUS1. The utilization of [18F]FDG for some types of diseases within SUS is under public consultation as the present article is being reviewed. Thus, nuclear medicine practiced within SUS is quite more restricted than that practiced in the complementary healthcare network or even at private institutions. Table 1 shows a list of the radiopharmaceuticals produced by Instituto de Pesquisas Energéticas e Nucleares (IPEN/CNEN-SP) and respective applications. IPEN is a State institution responsible for the implementation and dissemination of nuclear medicine in the country, as it developed and has been producing the main products utilized by the specialty since 1959(3,4). The last column shows the products currently utilized in procedures supported by SUS. It is important to highlight that there are procedures supported by SUS which are rarely or never performed, such as pancreatic scintigraphy and determination of red blood cell survival time (with radioisotopes). 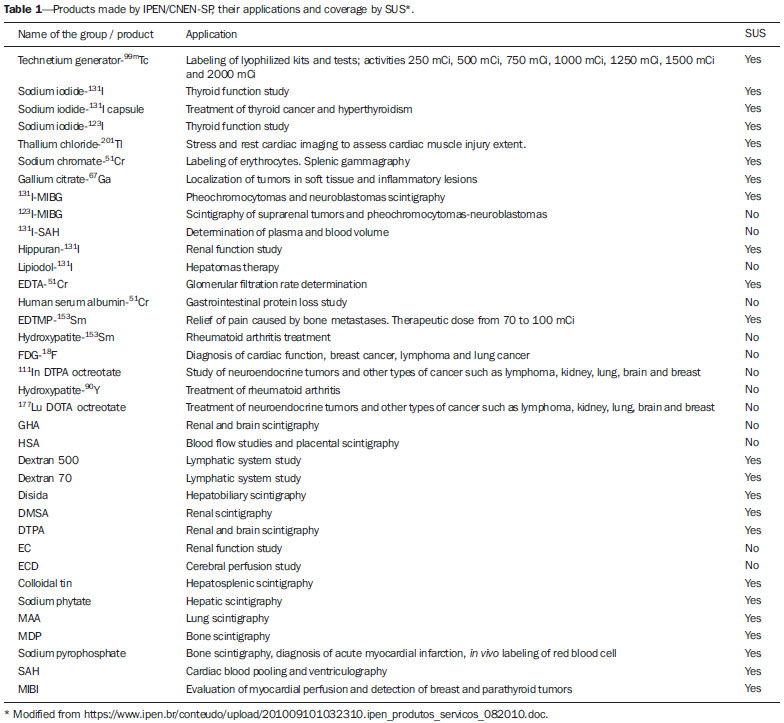 The present study is aimed at mapping the access to SUS by those patients who require outpatient nuclear medicine high-complexity diagnostic procedures throughout the entire national territory and by regions. The authors aimed at analyzing most of the available data in order to depict a more complete scenario of the specialty. Then, data regarding number of specific apparatuses (gamma cameras), outsourcing of procedures and most performed procedures, for example, were analyzed. The hospital procedures which require hospital admission were not analyzed, as a different investigation method would be required. Considering that radiopharmaceuticals are utilized in nuclear medicine procedures, the institutions that perform such procedures must be licensed by Comissão Nacional de Energia Nuclear (CNEN). Thus, the present study also aimed at verifying the correspondence between data obtained from Datasus and those made available by CNEN (www.cnen.gov.br). MATERIALS AND METHODS Data on the number of existing gamma cameras were obtained at CNESnet(5). The investigation was carried out by State, for all municipalities within field 1- Imaging diagnosis apparatuses, code 01 - gamma cameras. The search returns the CNES number, the name of the health service, the city where it is located and the number of apparatuses in operation. The number of outpatient procedures carried out and approved by SUS in the period of January through December 2008 was evaluated and after that, the same evaluation was made for 2009, 2010, 2011 and 2012 per State and per region. An investigation on the administrative instances (private, federal, State or municipal) responsible for such procedures was also carried out. Also, the distribution of such procedures was also investigated with respect to type of service provider: federal institution, State institution, municipal institution, private for-profit organization, for-profit services operating under SIMPLES tax regime, non-profit private services, philanthropic service with valid CNES registration. A search was made on code 151 nuclear medicine specialized service offered by several centers either SUS or outsourced. The search was made for outpatient in vivo nuclear medicine procedures, per State, and subsequently grouped for the entire country. Thus, it was possible to compare such result on a State by State basis, with the list of authorized CNEN services (<www.cnen.gov.br>, March 2013). Such services are licensed for operations and can currently purchase radiopharmaceuticals for nuclear medicine. RESULTS According to the investigation regarding apparatuses, there would be 875 gamma cameras in Brazil, 834 of those currently in operation. Such a figure does not match reality, as a finer analysis shows that only 49.7% of the apparatuses currently in utilization (415) are located at nuclear medicine services. The other 50.3% are located, according to Datasus, at dental or radiology clinics which do not perform nuclear medicine procedures. Such an analysis is possible as Datasus provides access to data regarding each one of the listed health services. Among the entities that operate their own nuclear medicine service, and therefore certainly have gamma cameras, 74.2% are private while only 6.3% are public. In 2012, 392,264 outpatient nuclear medicine procedures were performed by SUS. Amongst the 50 types of procedures covered by SUS, 7 correspond to 92.1% of the performed procedures, as follows: rest-stress myocardial scintigraphy (a minimum of three views), whole-body bone scintigraphy either with or without blood flow images, renal scintigraphy/renography (qualitative and/or quantitative), renal dynamic study with or without diuretics, thyroid scintigraphy with or without uptake, whole-body scintigraphy. Figure 1 shows the regional distribution of such procedures throughout the national territory. There is a noticeable concentration in the most developed and more densely populated Southeastern region, followed by the Northeastern and Southern regions. Although the Southern region is in the third position in absolute figures, its procedures/1,000 inhabitants ratio is higher than that of the Northeastern region. 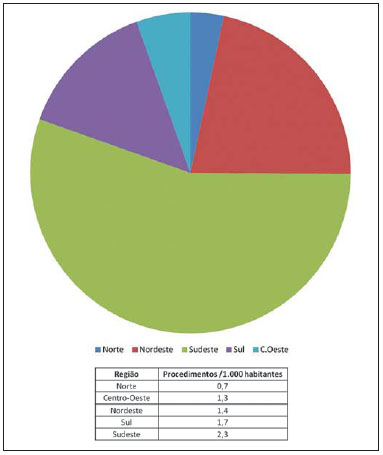 Figure 1. Regional distribution of the seven nuclear medicine procedures most performed by SUS and procedures/1,000 inhabitants ratio. In the investigated period, from 2008 to 2012, the number of outpatient procedures performed by SUS increased by 26.5%. However such a growth was not uniform, with 48.0% in the Northern region, 40% in the Mid-western region, and with the Southeastern region demonstrating the lowest growth (21.4%). The growth was not constant either along those years. Between 2009 and 2010, a growth of 8.2% was observed, and between 2010 and 2011 it was 9.3%. It is interesting to observe that between 2008 and 2009 the growth was 1.4%, despite the worldwide shortage of 99Mo/99mTc generators, the main radioactive diagnostic agent utilized in nuclear medicine. Amongst all nuclear medicine outpatient procedures supported by SUS, 82% were performed at private institutions (Figure 2). Such a distribution is similar to the distribution of other high complexity imaging diagnosis procedures, such as magnetic resonance imaging and x-ray computed tomography. However in those two specific cases, according to the data from Datasus, private services are responsible for 74.0% and 54.0% of the procedures, respectively. Table 2 shows that private services are responsible for practically all the procedures performed in the Northern region, closely followed by the Northeastern region. It is important to highlight that the Mid-western region presents with 78.5% of the outpatient procedures production at private services supported by SUS, closely matching the Southeastern region, with 78.0%. However, a more careful analysis reveals that the Federal District, where only public services perform diagnostic procedures for SUS, is accountable for such a value. In the States of Mato Grosso, Mato Grosso do Sul and Goiás, such procedures are exclusively performed by private services. 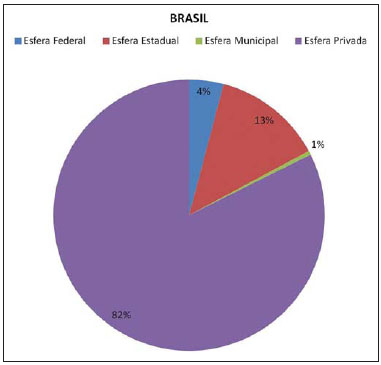 Figure 2. National outpatient procedures production by SUS per administrative instance in 2012. 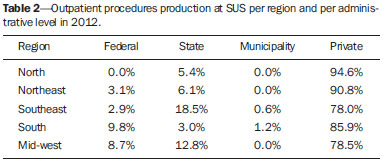 The private services are divided into: for profit private services; for profit private services operating under SIMPLES regime; non-profit private services; philanthropic services with a valid CNES. According to Table 3, there is a great variation among the regions as regards types of services providers responsible for such diagnostic procedures. In the Midwestern region, practically all the patients requiring diagnostic procedures (93.8%) are referred to for profit private services, followed by the Northern region (77.4%). The Southeastern region is the region that gets closer to the intent to prioritize non-profit services. The Southern and Northeastern regions present a more balanced division between for profit and non-profit services. 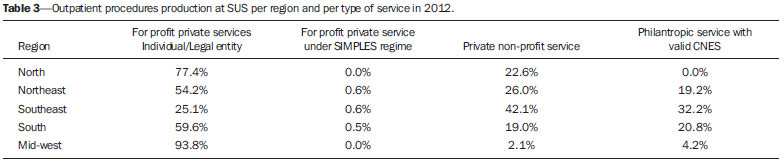 As the contribution of the different types of services providers between 2008 and 2012 is analyzed, it is observed that the only modality that consistently grew was that of private for profit services (Figure 3). The contribution of private nonprofit services in 2012 should be highlighted. Rio Grande do Sul and São Paulo are the main contributors to such an increase: in 2011 there were respectively 126 and 2,491 procedures performed by services in those States, and in 2012 there were 7,611 and 66,413 procedures, characterizing approximately a 60-fold and a 26-fold increase, respectively. 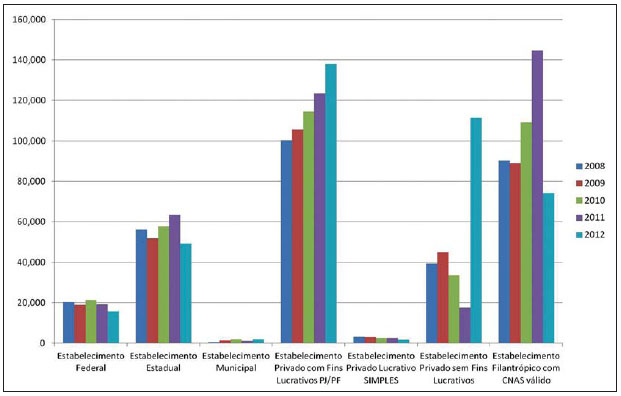 Figure 3. Contribution of the different types of service providers to specialized outpatient in vivo nuclear medicine service in the period between 2008 and 2012. According to the CNES databank, there are 776 services performing specialized in vivo nuclear medicine procedures, 79.3% private and 20.7% public belonging to one of the three levels of the public sector, with a predominance of federal and State levels, primarily in more developed States such as São Paulo. The private entities have their own services in 70.0% of the cases. The others utilize outsourced services. The situation is the opposite in the case of public entities: less than 30% of them have their own services, and more than 70.0% of the nuclear medicine procedures are performed by outsourced private services (Table 4). In total, 61.3% of the offered services are provided by themselves, while 38.0% are outsourced. 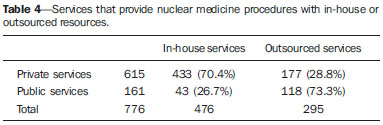 As the number of entities offering their own nuclear medicine services with the list of services accredited by CNEN, one observes a discrepancy of 13.4%, i.e., 64 out of the 476 private services that perform outpatient procedures paid by SUS are not authorized by CNEN to receive radioactive materials and, therefore, could not provide diagnostic nuclear medicine services. Table 5 shows the situation per State and per region. The CNEN authorization is given to services to purchase halflife radioactive materials for studies such as in vivo 99mTc imaging, for therapies utilizing 153Sm, for example, and for positron emitters (PET) imaging, the latter not being supported by SUS. Thus, sometimes, in some States, the number of services authorized by CNEN can be higher than that listed by Datasus. However, the cases where the opposite occurs - a number of services authorized by CNEN smaller than that listed by SUS -, deserve attention. Such is the case in the Northeastern, Southeastern and Southern regions, led by the latter. Santa Catarina is the State with the highest number of services not authorized by CNEN, in spite of being listed by SUS, with 17 services, followed by Rio Grande do Sul with 14, and by Minas Gerais with 12 services. 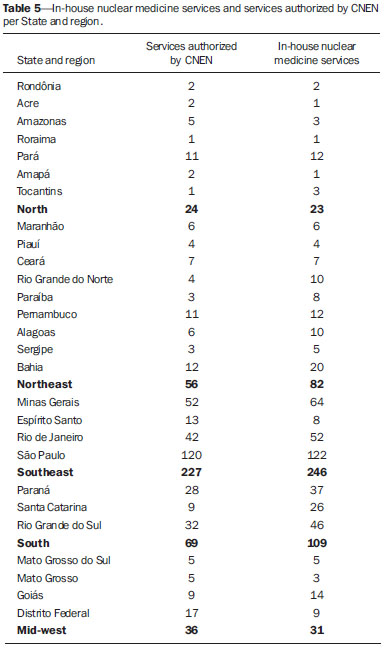 Datasus does not provide fields to be filled out neither with the name of the technical manager nor the name of the radiological protection supervisor. The presence of those two professionals is mandatory as per the CNEN - NN 3.05 Regulation(6). DISCUSSION Although the filling-out of the SUS forms is mandatory for acknowledgement and payment of the procedures performed by the public network and by the partnering private network, not all fields are filled-out with reliable information. Such is the case of the information on number of gamma cameras that is important to depict the current scenario with reliable prospects on the reality of nuclear medicine procedures available to the Brazilian population by means of SUS. Such information was previously utilized by Freitas et al.(7) for the State of São Paulo. However the limitations found by the present study had not been identified. The present study demonstrates that it is possible to generate estimates based on other data provided by CNES. According to a market investigation carried out in 2009 by BizAcumen(8), in 2010 there were approximately 1,850 gamma cameras in The United States of America, a number 4.5 times the estimated number for Brazil in 2012. A way to verify such values would be comparing them with those at the CNEN database, since the installation and use of nuclear medicine imaging equipment must be notified to CNEN by the health service. The present study demonstrates that, actually, the public nuclear medicine is practiced at private services. It is a high complexity specialty which involves multidisciplinary personnel and knowledge, differently from other modalities so classified by SUS, such as magnetic resonance imaging and radiology. Additionally, due to the fact that such services utilize unsealed radiation sources, they should report to CNEN in order to obtain their operation licenses. Because of such characteristics, the cost to maintain a nuclear medicine service is higher than that of a radiology service equipped with computed tomography and magnetic resonance imaging apparatuses. Perhaps for such a reason, the portion of procedures performed at private services is even greater than those two other specialties. The proportion increases in determined States such as Mato Grosso do Sul, where all nuclear medicine diagnostic procedures are carried out at private services. As the partnering private network is not obliged to meet the entire demand from SUS, part of the population may not receive care, for the benefit of the privately supported patients. Thus, the offering of nuclear medicine procedures performed by public services should be increased, starting by the States where the private services perform higher percentages of the procedures. Despite the great number of procedures performed at philanthropic services, there is no consistence in their growth over the years. In 2012, that number was considerably reduced, while the number of procedures performed at nonprofit private organizations, which were decreasing since 2009, actually presented a noticeable increase in that period. Such a fact should be further studied in other instances. Cardiac perfusion scintigraphy is the main performed procedure, corresponding to 54% of the total. It is expected that almost all such procedures be performed by means of single photon emission computed tomography (SPECT), although SUS pays the same value both for tomographic and planar procedures. Such a difference, which leads to different diagnostic quality, cannot be verified by data supplied by Datasus. Bone scintigraphy corresponds to 25% of all procedures. A great part of such studies must be based on whole-body scans and not only on planar acquisitions. Such data cannot be retrieved from Datasus either. It is important to highlight that patients submitted to those two procedures benefit considerably when the procedures are performed in hybrid SPECT/CT apparatuses. With those apparatuses, it is possible to simultaneously obtain functional data provided by nuclear medicine, and anatomical data provided by CT, so the approach to be adopted and the total cost of the treatment could be optimized. The simultaneous acquisition of functional and anatomical data is not covered by SUS. That is an important point to be evaluated as one considers a unified public system, but that is not yet a reality for SUS. One should also consider the aging of the population, leading to ever increasing number of cases of heart disease and cancer in general. There is an ever increasing need for reviewing the utilization of SUS's resources, considering that the early diagnosis of such and other diseases could be done by means of the nuclear medicine technology, particularly by means of hybrid SPECT/CT and PET/CT equipment. The present study was not aimed at investigating the utilization of PET or PET/CT, as there are no available data at Datasus on the utilization of such methods. But, although SUS does not cover PET procedures and hybrid PET/CT methods either yet, they should be promptly considered in the context of the increasing demand for oncology services as previously discussed. Currently, Brazil utilizes approximately 450 Ci of 99mTc per week that come from 99Mo/99mTc generators supplied by IPEN/CNEN-SP. Brazil does not produce the required 99Mo and imports such material from Argentina, South Africa and Canada. However there is an ongoing effort applied on the project of building the Brazilian Multipurpose Reactor (RMB)(9). Such a reactor will produce 1,000 Ci of 99Mo per week. The Brazilian Ministry of Science, Technology and Innovation estimates a considerable development of nuclear medicine in the country. Such investment may be increased by joint efforts with the Ministry of Health towards stimulating the growth of the specialty in the public network, as the private sector demonstrates to be very efficient in meeting its own demand as well as part of the demand from SUS, as demonstrated by the present study. The discrepancy between the number of nuclear medicine services enrolled at SUS and those accredited and licensed by CNEN indicates the need for placing efforts to unify the data. It is very important to remind that the CNEN's authorization is based upon principles of radiological protection which must be in force at the enrolled institutions, in order to guarantee the safe utilization of unsealed radiation sources in nuclear medicine. Thus, it would be interesting that institutions enrolled at SUS only receive the payment for their services provided that they are authorized by CNEN to utilize radioactive materials in the specified quantities. Also, it is important that the mandatory SUS forms include fields to be filled out with the name of the professional in charge of radiological protection supervision at the institution and with the function of responsible technical manager. Finally, it is important to highlight that the inclusion of a given clinic or nuclear medicine service in the list of institutions authorized by CNEN depends upon the initiative of the managers of such clinics or services. CNEN is accountable for the licensing and enforcement of its standards. The input of data to Datasus is done by the health managers at municipal, State and federal levels. Such managers are responsible for the accuracy in the presentation of those data. For that reason, a modification must be directly made in the forms in order to mandatorily reflect the data contained in the CNEN lists. CONCLUSION Datasus provides a wealth of information for investigations on the reality of nuclear medicine in Brazil. However it is still necessary to include some fields to be filled out, such as the case of the name of radiological protection supervisor. The present study strongly indicates the need for integration with the CNEN database. It is necessary to make those professionals responsible for filling out the forms at dental clinics aware that "gamma camera" imaging apparatuses are not utilized in their specialty. Also, a greater awareness by those professionals responsible for filling out the forms at nuclear medicine services is necessary in order to keep their data on the number of gamma cameras always updated. With those values it is possible to make better estimations on the effective utilization of such apparatuses in the country. The present study has quantitatively demonstrated the reality that the nuclear medicine practiced by/for SUS actually occurs in the private sphere, but in an even greater proportion than imaging diagnosis procedures of equal complexity. Additionally it has also indicated points requiring further investigations as the type of service providers. Also it has also included a geographical mapping of smaller or greater necessities in terms of development of the specialty in the public sector, depending on the State. REFERENCES 1. Brasil. Ministério da Saúde. Secretaria Nacional de Assistência à Saúde. ABC do SUS - Doutrinas e princípios. [acessado em 11 de março de 2013]. Disponível em: http://biblioteca.planejamento.gov.br/biblioteca-tematica-1/textos/saude-epidemias-xcampanhas-dados-descobertas/texto-17-abc-do-sus-doutrinas-e-principios.pdf. 2. Brasil. Ministério da Saúde. Conselho Nacional de Secretários de Saúde. Assistência de média e alta complexidade no SUS. Coleção Progestores - Para entender a gestão do SUS. [acessado em 20 de fevereiro de 2013]. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/colec_progestores_livro9.pdf 3. Instituto de Pesquisas Energéticas e Nucleares. Centro de Radiofarmácia - Quem somos. [acessado em 10 de março de 2013]. Disponível em: https://www.ipen.br/sitio/?idm=113. 4. Gordon AMPL. Instituto de Pesquisas Energéticas e Nucleares - (1956-2000): um estudo de caso à luz da história da ciência, da tecnologia e da cultura brasileira. [Tese de doutorado]. São Paulo, SP: Universidade de São Paulo. [acessado em 1º de dezembro de 2010]. Disponível em: http://www.ipen.br/biblioteca/teses/11602.pdf. 5. Brasil. Ministério da Saúde. CNESNet. Cadastro Nacional de Estabelecimentos de Saúde. [acessado em 20 de fevereiro de 2013]. Disponível em: http://cnes.datasus.gov.br/. 6. Brasil. Ministério da Ciência, Tecnologia e Inovação. Comissão Nacional de Energia Nuclear. CNEN NN 3.05 - Requisitos de radioproteção e segurança para serviços de medicina nuclear. [acessado em 10 de março de 2013]. Disponível em: http://www.cnen.gov.br/seguranca/normas/pdf/Nrm305.pdf. 7. Freitas MB, Yoshimura EM. Levantamento da distribuição de equipamentos de diagnóstico por imagem e da frequência de exames radiológicos no Estado de São Paulo. Radiol Bras. 2005;38:347-54. 8. ReportLinker. Nuclear medicine - A global update of market trends - opportunities. BizAcumen. 2009. PR Newswire Association LLC, New York, USA. [acessado em 11 de março de 2013]. Disponível em: http://www.reportlinker.com/p0164233/Nuclear-Medicine-A-Global-Update-of-Market-Trends-Opportunities.html. 9. Perrota JA, Obadia IJ. The RMB project development status. [acessado em 20 de março de 2013]. Disponível em: http://www-pub.iaea.org/MTCD/Publications/PDF/P1575_CD_web/datasets/papers/C6%20Perrotta.pdf. 1. PhD, Researcher at the Radiopharmacy Center of Instituto de Pesquisas Energéticas e Nucleares (IPEN/CNEN-SP), São Paulo, SP, Brazil 2. Specialization in Nuclear and Legal Medicine, MD, Physician I at Instituto do Câncer do Estado de São Paulo Octavio Frias de Oliveira (Icesp), São Paulo, SP, Brazil 3. PhD, Manager - Management of Research and Development, Radiopharmacy Center of Instituto de Pesquisas Energéticas e Nucleares (IPEN/CNEN-SP), São Paulo, SP, Brazil 4. Master, Technologist at Radiopharmacy Center of Instituto de Pesquisas Energéticas e Nucleares (IPEN/CNEN-SP), São Paulo, SP, Brazil Mailing Address: Dra. Lorena Pozzo Rua Cotoxó, 424, ap. 83, Vila Pompéia São Paulo, SP, Brazil, 05021-000 E-mail: lorena.pozzo@ipen.br Received September 4, 2013. Accepted after revision January 10, 2014. Study developed at Instituto de Pesquisas Energéticas e Nucleares (IPEN/CNEN-SP), São Paulo, SP, Brazil. 1 The Federal Government Science, Technology and Strategic Inputs Secreariat published the decision of incorporating PET/CT procedures into the SUS list in April/2014. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554