Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 47 nº 1 - Jan. /Feb. of 2014
Vol. 47 nº 1 - Jan. /Feb. of 2014
|
CASE REPORT
|
|
Portal cholangiopathy: case report |
|
|
Autho(rs): Maria Cecilia Almeida Maia1; Aline Pimentel Amaro1; Edmundo Clarindo Oliveira2; José Renan da Cunha Melo3; Marcelo Dias Sanches3; Rogerio Augusto Pinto da Silva1 |
|
|
Keywords: Portal cholangiopathy; Portal biliopathy; Portal hypertension; Portal vein cavernous transformation. |
|
|
Abstract: INTRODUCTION
Portal cholangiopathy is defined as obstruction of the biliary tract in association with engorgement of collateral veins in the hepatic hilum(1). In general, the patients are asymptomatic, but jaundice, cholangitis and biliary lithiasis may be present in 5% to 38% of patients(1-5). In the present report, the authors describe the case of a child with portal thrombosis secondary to blunt abdominal trauma, progressing with portal hypertension and obstructive jaundice caused by portal biliopathy. CASE REPORT In May 2008, at the age of six years and seven months, a male child suffered an accident and had fracture of left lower limb and blunt abdominal trauma, with injury to the right liver lobe (Figure 1), which were conservatively treated. 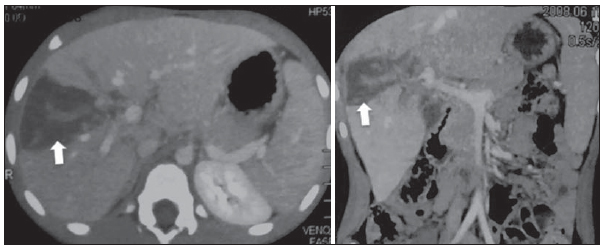 Figure 1. Computed tomography (axial and coronal reconstruction) performed at hospital admission, showing hepatic trauma affecting the right portal branch and the hepatic hilum (arrows). The portal vein and the left portal branch were not injured at that time. In March 2009, the patient presented with splenomegaly. Abdominal ultrasonography revealed total thrombosis of the right portal vein branch and stenosis between the intrahepatic portal vein and the left branch (Figure 2). An unsuccessful attempt was made for dilatation of the stenosis which progressed to total occlusion of the portal vein bifurcation and progressive splenomegaly as well as venous engorgement of collaterals surrounding the portal vein from the head of pancreas to the hepatic hilum. 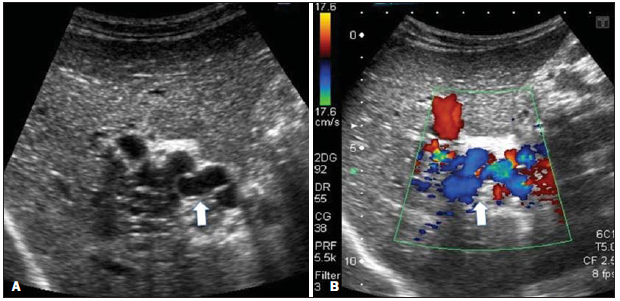 Figure 2. Ultrasonography (A) and color Doppler mapping (B) identifying multiple tortuous periportal veins in the hepatic hilum (arrows) corresponding to cavernous transformation of the portal vein. In December 2010, the patient presented with jaundice, and in January 2011, ultrasonography demonstrated intrahepatic biliary dilatation in association with presence of calibrous periportal veins (Figure 3). 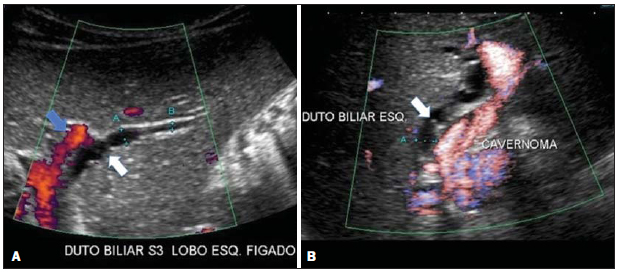 Figure 3. Dilatation of the biliary tract involved by prominent venous collaterals. Dilated left bile duct (white arrows and electronic pakymeters). Distal portion of the left branch of the patent portal vein (blue arrow). Cavernoma refers to tortuous periportal veins in the hepatic hilum. Echo-guided percutaneous puncture of biliary duct and subsequent cholangiography were performed, demonstrating reduction of the choledochal caliber. Later, Doppler US revealed the engorged vein twirled around the biliary drain into the choledochus (Figure 4). 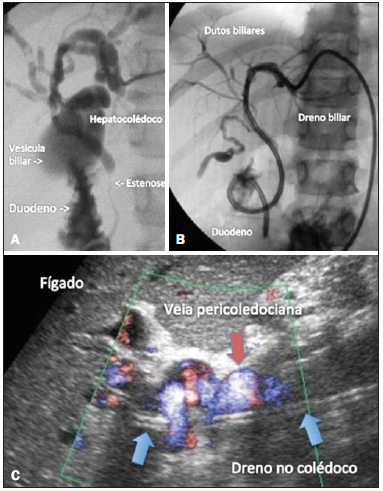 Figure 4. A: Percutaneous cholangiography demonstrating dilatation of the biliary tract up to the common bile duct, with abrupt decrease in the caliber at the level of the middle third of the choledochus. B: Internal-external-type drain percutaneously inserted into the biliary tract. C: Doppler ultrasonography demonstrating pericholedochal vein around the drain (arrow) in the hepatocholedochus. New attempts to dilate the stenosis on March 19, May 21, 2011, and March 10, 2012, with persistence of the extrinsic compression. On July 14, 2012, percutaneous puncture of the spleen for splenic vein catheterization and cannulation of the proximal segment of the portal vein and of the pericholedochal collateral were done, but the attempt was unsuccessful. Angiography demonstrated obstruction of the portal vein after its origin, in association with significant dilatation of pericholedochal veins up to the hepatic hilum, followed by enhancement of many small and thin veins similar to a cloud, with delayed filling of the left portal branch. The anatomy and pressure in the hepatic veins were normal. Several guide wires were utilized in the attempt to recover the lumen of the portal vein or to get the thin veins of the hepatic hilum dilated, but such an attempt was also unsuccessful. Currently, the child remains with an internal-external type biliary drain that is periodically replaced, with assessment by means of cholangiography. DISCUSSION Portal cholangiopathy results from alterations of the biliary tract in the cavernous transformation of the portal vein(6), in association with engorgement of periportal veins around the pancreas, choledochus and hepatogastric ligament(5). As the veins of the epicholedochal plexus (plexus of Saint) and paracholedochal plexus (plexus of Petren) respectively located around and on the wall of the hepatocholedochus are engorged, one may observe its compression also associated with the inflammatory ischemic process which causes areas of fibrosis with consequential biliary tract stenosis which resolve after the management of the portal hypertension(7). In spite of such a condition being frequently observed at imaging methods, the patients, particularly children, are generally asymptomatic, eventually presenting increased levels of hepatic enzymes. In the present case report, the authors describe the set of symptoms of a child with portal biliopathy secondary to portal vein thrombosis, consequential to blunt abdominal trauma, developing with portal hypertension and obstructive jaundice refractory to treatment. The clinical cholangiopathy manifestations can be divided into two groups, as follows: a) those resulting from cholestasis (jaundice and itch); b) those secondary to intrahepatic biliary lithiasis, corresponding to pain in the right hypochondrium, jaundice and fever. Symptoms are most commonly observed in the elderly, particularly in the presence of gallbladder calculi. Morphological alterations most frequently observed at cholangiography include biliary tract dilatation associated with areas of stenosis and angulations, as well as failure in duct filling due to compression by dilated parietal veins projecting towards the lumen(6). Differential diagnosis should include hepatic hilum neoplasia, such as cholangiocarcinoma or metastatic neoplasms, as well as other causes of intrahepatic bile ducts involvement, such as sclerosing cholangitis. The diagnosis is made by imaging methods, particularly color Doppler that is capable of detecting portal thrombosis and bile ducts dilatation. In cases of portal vein fibrosis caused by chronic portal thrombosis, it usually cannot be seen at B-mode, while the collaterals are visualized as serpiginous structures in the hepatic hilum, with venous flow at Doppler. Magnetic resonance imaging also allows the diagnosis of cavernous transformation of the portal vein and biliary dilatation, particularly by means of MR cholangiography. Cholangiography (either retrograde or percutaneous) may be done in cases where the treatment is indicated for dilatation and drainage of the biliary ducts as well as for decompression of portal system. If available, echoendoscopy represents an alternative method, allowing the study of the biliary tract and, depending on the equipment, it allows the utilization of the Doppler technique. As regards treatment, bile duct dilatation is indicated for symptomatic patients and with recurrent cholangitis. Portal decompression should generally be performed before bile ducts dilatation(6). REFERENCES 1. Walser EM, Runyan BR, Heckman MG, et al. Extrahepatic portal biliopathy: proposed etiology on the basis of anatomic and clinical features. Radiology. 2011;258:14653. 2. Dhiman RK, Behera A, Chawla YK, et al. Portal hypertensive biliopathy. Gut. 2007;56:10018. 3. Khuroo MS, Yattoo GN, Zargar SA, et al. Biliary abnormalities associated with extrahepatic portal venous obstruction. Hepatology. 1993;17:80713. 4. Dilawari JB, Chawla YK. Pseudosclerosing cholangitis in extrahepatic portal venous obstruction. Gut. 1992;33:2726. 5. Vibert E, Azoulay D, Aloia T, et al. Therapeutic strategies in symptomatic portal biliopathy. Ann Surg. 2007;246:97104. 6. Gibson JB, Johnston GW, Fulton TT, et al. Extrahepatic portalvenous obstruction. Br J Surg. 1965;52:12939. 7. D'Souza MA, Desai D, Joshi A, et al. Bile duct stricture due to caused by portal biliopathy: treatment with one-stage portal-systemic shunt and biliary bypass. Indian J Gastroenterol. 2009;28:357. 1. MDs, Radiologists at Clínica CEU Diagnósticos, Belo Horizonte, MG, Brazil 2. MD, Hemodynamicist at Clínica CEU Diagnósticos, Belo Horizonte, MG, Brazil 3. PhDs, Professors, Department of Surgery at School of Medicine, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, MG, Brazil Mailing Address: Dra. Maria Cecilia Almeida Maia Rua Oscar Trompowsky, 721/406, Gutierrez Belo Horizonte, MG, Brazil, 30441-055 E-mail: mariaceciliaalmeida@yahoo.com.br Received November 12, 2012. Accepted after revision May 27, 2013. Study developed at Clínica CEU Diagnósticos, Belo Horizonte, MG, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554