Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 46 nº 6 - Nov. / Dec. of 2013
Vol. 46 nº 6 - Nov. / Dec. of 2013
|
CASE REPORT
|
|
Cardiac tamponade in an infant during contrast infusion through central venous catheter for chest computed tomography |
|
|
Autho(rs): Danilo Felix Daud1; Marcos Menezes Freitas de Campos1; Luciano Augusto de Pádua Fleury Neto2 |
|
|
Keywords: Cardiac tamponade; Radiology; Thoracic surgery. |
|
|
Abstract: INTRODUCTION
Generally, the discussions about complications from central venous catheterization in children concentrate on infectious complications and on the most common mechanical complications such as pneumothorax, hemothorax and venous thrombosis(1). Nonetheless, pericardial effusion has already been reported by international studies, most of them describing cases of neonates submitted to umbilical catheterization(2,3) and or catheterization through other central venous lines(4,5). CASE REPORT The authors report the case of a three-month-old, preterm child admitted to infantintensive care unit, with acute renal failure and sepsis with a probable pulmonary focus. Central venous access was not available and was obtained by the intensivist physician by means of puncture of the right internal jugular vein. Subsequently, the patient was referred to undergo contrast enhanced chest computed tomography. Immediately after iodinated contrast agent infusion (Figure 1), the child presented clinical worsening and was promptly taken back to the intensive care unit. The thoracic surgery team was called. 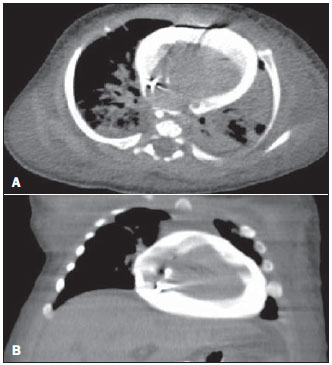 Figure 1. Contrast enhanced chest computed tomography images. A: Axial section presence of contrast in the pericardial sac (effusion) and bilateral pneumonia. B: Coronal reconstruction presence of contrast in the pericardial sac (effusion). Considering the clinical signs of pericardial effusion with cardiac tamponade and consequential cardiac arrest, pericardiocentesis was performed (Marfan puncture) with aspiration of 30 ml hematic fluid and cardiorespiratory resuscitation maneuvers with heart beat recovery. The patient was taken to the surgical center assisted by one of the thoracic surgery team members while another member was already prepared to initiate the thoracotomy. Right lateral thoracotomy was performed once the hypothesis of right atrial perforation by the central venous catheter was raised. The surgical strategy included pericardiotomy and atrial cardiorrhaphy. The child's clinical condition worsened, progressing to death seven days after the procedure due to multiple organs failure. DISCUSSION Pericardial effusion with cardiac tamponade by itself represents a severe problem for any patient. In a frail child admitted to an intensive care unit with other diseases, such a condition is potentially fatal. It may be caused by umbilical catheterization, particularly in neonates(2,3), or other central venous access lines(4,5). The cause and prompt diagnosis of such an event during contrast enhanced chest computed tomography scan make this case rare. No similar case report has been found in the literature. The authors conclude that careful insertion techniques as well as continuous observation of the correct positioning and function of central venous catheters, besides the utilization of good quality materials, are essential to aid in the prevention of severe complications. REFERENCES 1. Askegard-Giesmann JR, Caniano DA, Kenney BD. Rare but serious complications of central line insertion. Semin Pediatr Surg. 2009;18:73-83. 2. Megha M, Jain N, Pillai R. Pericardial tamponade in a newborn following umbilical catheter insertion. Indian Pediatr. 2011;48:404-5. 3. Traen M, Schepens E, Laroche S, et al. Cardiac tamponade and pericardial effusion due to venous umbilical catheterization. Acta Paediatr. 2005;94:626-8. 4. Nowlen TT, Rosenthal GL, Johnson GL, et al. Pericardial effusion and tamponade in infants with central catheters. Pediatrics. 2002;110(1 Pt 1):137-42. 5. Ohki Y, Yoshizawa Y, Watanabe M, et al. Complications of percutaneously inserted central venous catheters in Japanese neonates. Pediatr Int. 2008;50:636-9. 1. MDs, Thoracic Surgeons, Hospital Geral de Palmas, Pal-mas, TO, Brazil 2. MD, Radiologist, Hospital Geral de Palmas, Palmas, TO, Brazil Mailing Address: Dr. Danilo Felix Daud 603 Sul, Alameda 14, Lote 19, Plano Diretor Sul Palmas, TO, Brazil, 77016-374 E-mail: danilodaud@uol.com.br Received November 4, 2012. Accepted after revision April 19, 2013. Study developed at Hospital Geral de Palmas, Palmas, TO, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554