Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 6 - Nov. / Dec. of 2012
Vol. 45 nº 6 - Nov. / Dec. of 2012
|
CASE REPORT
|
|
Transcranial sonography findings in Parkinson's disease and essential tremor: cases report |
|
|
Autho(rs): Rita de Cassia Leite Fernandes1; Ana Lucia Zuma de Rosso2; Maurice Borges Vincent3; Paulo Roberto Valle Bahia4; Celia Maria Coelho Resende5; Nordeval Cavalcante Araujo6 |
|
|
Keywords: Transcranial sonography; Parkinson's disease; Essential tremor. |
|
|
Abstract: INTRODUCTION
Parkinson's disease (PD) is characterized by resting tremors, bradykinesia and muscle stiffness. However, the presence of isolated tremor may represent a diagnostic challenge, considering the difficult differentiation between initial signs of PD and essential tremor (ET)(1). The two conditions present distinctive clinical courses - PD is more severe -, as well as distinctive therapeutic approaches. For that reason, neuroimaging studies such as brain computed tomography and magnetic resonance imaging are requested, however without providing a sure diagnosis of neither of the two entities, restricting the role of those imaging methods to that of ruling out causes of secondary parkinsonism, such as hydrocephalus, cerebrovascular disease, etc.(2). Functional neuroimaging, such as positron emission tomography (PET) or single-photon emission tomography (SPECT), might play a relevant role in the differential diagnosis because of their capability of identifying reduced striatal dopaminergic activity; but their high cost and limited availability outside of the large Brazilian research centers make their routine utilization unfeasible(1,2). Research on transcranial sonography (TCS) started in 1995 when investigators observed increased echogenicity at the mesencephalic substantia nigra (SN) site in patients with PD(3). The technique has been studied in several countries, with a high number of publications validating its usefulness in the differential diagnosis of diseases coursing with parkinsonian symptoms, particularly PD and ET(4). TCS is harmless, low-cost, performed with widely available equipment and does not require patient sedation. The greatest limitation of this technique is dependence on the temporal acoustic window to allow the ultrasound waves to overcome the bone barrier and generate two-dimensional images of intracranial structures. This accounts for 10% to 20% of failure of the method to obtain useful diagnostic images(1). Many authors reported key TCS finding in PD patients - expanded area of SN echogenicity > 0.20 cm -, in up to 90% of cases(5). In the Hospital Universitario Clementino Fraga Filho da Universidade Federal do Rio de Janeiro (HUCFF-UFRJ), a study is currently going on about the usefulness of the method for the diagnosis of PD in the Brazilian population. In a pilot study, 88% of the PD patients presented expanded area of SN echogenicity, corroborating the good sensitivity of the method for detecting the disease(6). However, the finding of the marker in individuals within the control group (false-positive results), reduced the technique specificity to approximately 82%. Recent prospective multicentric studies suggest that healthy individuals with expanded SN area measured at TCS present increased risk for developing PD(7), therefore making such echographic change a candidate for a risk marker of the disease(1). With the aim of presenting to the radiologists an example of the application of TCS, the authors present two cases of PD patients and ET patients paired by gender and age, where TCS could provide additional diagnostic information regarding one or the other disease. The present study was approved by the Committee for Ethics in Research of HUCFF-UFRJ. The patients were selected in the Movement Disorders Clinic of the HUCFF as follows: two PD patients diagnosed according to the United Kingdom Brain Bank criteria(8); and two ET patients, diagnosed according to the Movement Disorders Society criteria(9). The scans were performed with an AcusonX300 equipment (Siemens; Erlangen, Germany) with a 1.52.5 MHz phased-array transducer, as the previous described method(4,6). Axial sections were obtained bilaterally by insonating the preauricular region. A hypoechoic, butterfly-shaped image of the mesencephalon (outlined on the figures), surrounded by the hyperechogenic basal cisterns was visualized on the plane parallel to the orbitomeatal line. The hyperechogenic area of the SN visualized on the cerebral peduncle ipsilateral to the insonation region was measured. Values > 0.20 cm2 were considered as being increased, according to the international consensus(4). CASES REPORT Case 1 - A 70-year-old woman with PD for ten years, at Hoehn and Yahr stage II. USTC demonstrated bilaterally increased echogenicity of the mesencephalic SN area (Figure1). The SN area at right measured 0.32 cm2 and, at left, 0.27 cm2.  Figure 1. Transcranial sonography - case 1. Left preauricular insonation in a patient with Parkinson's disease. The hypoechoic butterfly-shaped mesencephalon is outlined at the center of the image, surrounded by the hyperechogenic basal cisterns. The echogenic areas of the substantia nigra in the cerebral peduncle are outlined by dotted lines. (AS, Sylvian aqueduct; FIP, interpeduncular fossa). Case 2 - A 51-year-old man with PD for 9 years, at Hoehn and Yahr stage II. The patient presented important unilateral increase of the SN at ultrasonography: right SN echogenic area with 0.27 cm2 and the left with 0.17 cm2 (Figure 2).  Figure 2. Transcranial sonography - case 2. Right preauricular insonation in a patient with Parkinson's disease. Outlined mesencephalon. The echogenic area of the right substantia nigra is measured (A1 = 0.27 cm2). (SND, right substantia nigra). Case 3 - A 70-year-old woman with ET for 40 years. SN echogenicity area at right measuring 0.12 cm2 and at left, 0.16 cm2 (Figure 3). 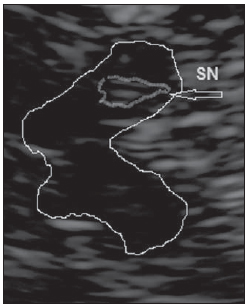 Figure 3. Transcranial sonography - case 3. Right preauricular insonation in a patient with essential tremor. Outlined mesencephalon. The echogenic area of the right substantia nigra is outlined on the cerebral peduncle. (SN, substantia nigra). Case 4 - A 48-year-old man with ET since his youth. The right-sided SN echogenic area measured 0.11 cm2 and the left-sided, 0.10 cm2 (Figure 4). 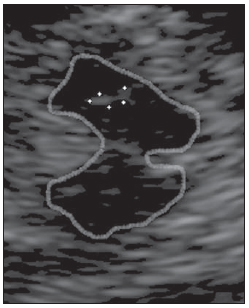 Figure 4. Transcranial sonography - case 4. Left preauricular insonation in a patient with essential tremor. Outlined mesencephalon. The echogenic area of the left substantia nigra is outlined by dotted lines. DISCUSSION The images of the encephalon visualized at TCS provide important morphometric data for the diagnosis of some neurological disorders(4,5). Because of the physical characteristics of the method and the need to overcome the bone barrier, the most appropriate image demonstrates structures located on the midline of the brain stem and basal ganglia(4). Such characteristics make the method suitable for the study of movement disorders whose origin is the dysfunction of such structures. An echogenic SN area > 0.20 cm2, either unilateral or bilaterally, is strongly correlated with PD diagnosis, and is considered as a stable marker since it does not undergo changes with the disease progression(3-5). Unilateral SN enlargement is associated with the side of the symptoms(4). The four described cases correspond to individuals with clinically confirmed diagnosis of both long-lasting PD and ET. The measurement of the echogenic area at the SN site could differentiate the two diseases. Such area was > 0.20 cm2 in the two PD cases (bilaterally in case 1 and unilaterally in case 2), and was normal in the two ET cases (cases 3 and 4). Enlargement of the SN echogenic area may also be found in healthy individuals, in those with atypical parkinsonism (progressive supranuclear palsy, multisystems atrophy, etc.), and even in ET patients, which would contribute to the reduction of the method specificity, besides(5,10). The cause of increased SN echogenicity still remains subject of debate. Considering that such characteristic is present since the onset of the condition and does not change with the disease progression, it must not be caused by neuronal degeneration(4,7). There are evidences that the increased iron content in the SN site might be responsible for the finding(11). CONCLUSION Considering that TCS is an innocuous and low-cost method, providing relevant information to the neurologist, TCS deserves to be further investigated for the diagnosis of movement disorders. The limitations of this method include dependence on the temporal acoustic bone window and low specificity, which would place it in the category of screening methods(10). Some Brazilian studies have already confirmed the validity of TCS findings for the diagnosis of movement disorders among us(6,12). REFERENCES 1. Stern MB, Lang A, Poewe W. Toward a redefinition of Parkinson's disease. Mov Disord. 2012;27:54-60. 2. Doepp F, Plotkin M, Siegel L, et al. Brain parenchyma sonography and (123)I-FP-CIT SPECT in Parkinson's disease and essential tremor. Mov Disord. 2008;23:405-10. 3. Becker G, Seufert J, Bogdahn U, et al. Degeneration of substantia nigra in chronic Parkinson's disease visualized by transcranial color-coded real-time sonography. Neurology. 1995;45:182-4. 4. Walter U, Behnke S, Eyding J, et al. Transcranial brain parenchyma sonography in movement disorders: state of the art. Ultrasound Med Biol. 2007;33:15-25. 5. Vlaar AMM, Bouwmans A, Mess WH, et al. Transcranial duplex in the differential diagnosis of parkinsonian syndromes: a systematic review. J Neurol. 2009;256:530-8. 6. Fernandes RCL, Rosso ALZ, Vincent MB, et al. Transcranial sonography as a diagnostic tool for Parkinson's disease: a pilot study in the city of Rio de Janeiro, Brazil. Arq Neuropsiquiatr. 2011;69:892-5. 7. Berg D, Seppi K, Behnke S, et al. Enlarged substantia nigra hyperechogenicity and risk for Parkinson disease: a 37-month 3-center study of 1847 older persons. Arch Neurol. 2011;68:932-7. 8. Hughes AJ, Daniel SE, Kilford L, et al. Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55:181-4. 9. Deuschl G, Bain P, Brin M. Consensus statement of the Movement Disorders Society on Tremor. Ad Hoc Scientific Committee. Mov Disord. 1998; 13 Suppl 3:2-23. 10. Lauckaitg K, Rastenytg D, Surkieng D, et al. Specificity of transcranial sonography in parkinson spectrum disorders in comparison to degenerative cognitive syndromes. BMC Neurol. 2012;12:12. 11. Berg D, Roggendorf W, Schröder U, et al. Echogenicity of the substantia nigra: association with increased iron content and marker for susceptibility to nigroestriatal injury. Arch Neurol. 2002;59:999-1005. 12. Bor-Seng-Shu E, Fonoff ET, Barbosa ER, et al. Substantia nigra hyperechogenicity in Parkinson's disease. Acta Neurochir (Wien). 2010;152:2085-7. 1. Master, Ministry of Health Physician, Fellow PhD degree, Post-graduation Program in Medical Practice (Concentration area: Neurology), Faculdade de Medicina da Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. 2. PhD, Head of Movement Disorders Clinic, Hospital Universitário Clementino Fraga Filho - Universidade Federal do Rio de Janeiro (HUCFF-UFRJ), Rio de Janeiro, RJ, Brazil. 3. PhD, Assistant Professor, Universidade Federal do Rio de Janeiro (UFRJ), Head of the Neurologic Clinic, Hospital Universitário Clementino Fraga Filho - Universidade Federal do Rio de Janeiro (HUCFF-UFRJ), Rio de Janeiro, RJ, Brazil. 4. PhD, Assistant Professor, Universidade Federal do Rio de Janeiro (UFRJ), Head of the Radiodiagnosis Unit, Hospital Universitário Clementino Fraga Filho - Universidade Federal do Rio de Janeiro (HUCFF-UFRJ), Rio de Janeiro, RJ, Brazil. 5. PhD, Head of the Unit of Ultrasonography, Hospital Universitário Clementino Fraga Filho - Universidade Federal do Rio de Janeiro (HUCFF-UFRJ), Rio de Janeiro, RJ, Brazil. 6. PhD, Associate Professor of Post-graduation in Medical Sciences, Universidade do Estado do Rio de Janeiro (UERJ), Rio de Janeiro, RJ, Brazil. Mailing Address: Dra. Rita C. L. Fernandes Rua Marques de Abrantes, 171/502, Flamengo Rio de Janeiro, RJ, Brazil, 22230060 E-mail: ritafernandes@ufrj.br Received May 30, 2012. Accepted after revision August 8, 2012. * Study conducted at Hospital Universitário Clementino Fraga Filho - Universidade Federal do Rio de Janeiro (HUCFF-UFRJ), Rio de Janeiro, RJ, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554