Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 4 - July / Aug. of 2012
Vol. 45 nº 4 - July / Aug. of 2012
|
ORIGINAL ARTICLE
|
|
Adherence of a hospital female personnel to a breast cancer prevention program |
|
|
Autho(rs): Adeli Cardoso de Azevedo1; Ellyete de Oliveira Canella2; Maria Célia Resende Djahjah3; Hilton Augusto Koch4 |
|
|
Keywords: Breast cancer; Secondary prevention; Health care; Hospital environment. |
|
|
Abstract: INTRODUCTION
Prevention is an anticipated action based upon the knowledge of the natural history of a disease in order to make its later development unlikely(1). Primary, secondary and tertiary prevention strategies have been utilized with the objective of preventing diseases with early diagnosis and treatment besides minimizing their effects, assuring individuals an appropriate standard of living for health maintenance(2). Thus, the main difference between primary, secondary and tertiary prevention lies in the period of disease progression where one intends to intervene: before the disease onset (primary prevention), after its onset and symptoms have not manifested yet (secondary prevention), or in the presence of symptoms (tertiary prevention)(2). Breast cancer is currently an extremely relevant disease for public health world-wide, leading to discussions on measures to promote its early diagnosis and, consequently, decrease in morbidity and mortality rates(3). The early, presymptomatic diagnosis and treatment of cancers are characteristic of the secondary prevention. Mammography is included in this approach, as an early diagnostic method in breast cancer, capable of detecting non-palpable early-stage lesions, thus allowing a more effective and less aggressive treatment, with better aesthetic results and decreased adverse events(4). Along time, "care" has been considered as a guiding word. However, there is a paradox on account of the single direction that such "care" usually takes, i.e., the mission of the hospital environment is to save lives and recover the health of diseased individuals. It is hardly aimed at promoting and maintaining the health of its workers(5). Much has been said about breast cancer prevention in the social, hospital and ambulatory spheres, by means of public campaigns both of medical societies and nongovernmental organizations. How do women who work in hospital environments behave with respect to their own breast cancer prevention? With that question in mind, the present study was aimed at assessing the adherence of a school hospital female personnel to a breast cancer prevention program, by means of mammography. MATERIALS AND METHODS In 1998, the Program for Women's Health in Preventive Gynecology (PWHPG) was created in the Hospital Universitário Clementino Fraga Filho (HUCFF) of Universidade Federal do Rio de Janeiro (UFRJ), sponsored by the Serviço de Segurança a Saúde do Trabalhador (SESSAT) (Worker's Health and Safety Program), with the support of the hospital administration, with the purpose of providing specialized care for the female workers of the institution. In 2002, 436 female workers of the HUCFF previously enrolled in the Program of SESSAT were asked to participate in semi-structured interviews including objective and subjective questions. The purpose of such interviews was to know the behavior of such workers in relation to health in the work environment and especially with respect to breast cancer prevention. Among the 436 workers, 162 agreed to participate, and made appointments for their interviews, but only 120 have actually attended the appointment. Of the 120 interviewed workers, 29 were excluded for not belonging to the appropriate age group to undergo mammography and for not belonging to the risk group for breast cancer risk group, according to the clinical criteria of the assisting physician. The remaining 91 workers who comprised the study sample, were followed-up in the period from 2000 to 2009. After the interviews, the medical records were verified in order to retrieve data since the year of 2000. The interviewed group was followed-up by means of their mammography reports from of 2000 to 2009, in order to confirm the performance of the mammography studies. The followed-up workers were not covered by a private health plan, and therefore depended upon the Sistema Único de Saúde (SUS) (Brazilian Health System) for treatment. For analysis of the questionnaires the quantitative method was utilized, allowing the coding of the collected data. RESULTS As the professional categories of the 91 respondents, 18 different positions were found, as shown on Table 1. 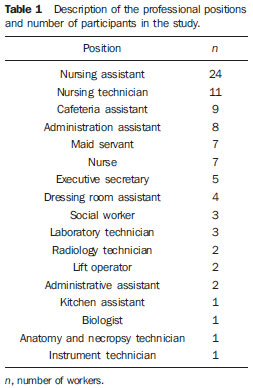 Over the study period, the 91 women underwent a total of 247 mammography studies. The number of mammograms per age range is described on Table 2. 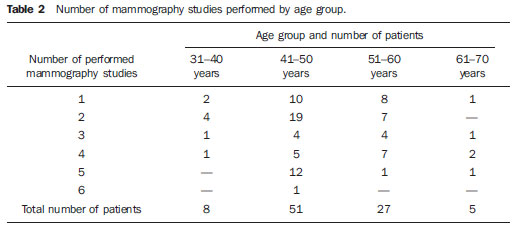 As regards education level, 145 mammograms belonged to workers with primary grade schooling, 55 to workers with high-school grade and 47 to workers with university degrees, totaling 247 mammograms performed during the study period. The highest adherence level was observed among the primary grade schooling workers, corresponding to 59.3%. The adherence among high-school grade workers accounted for 20.8%, while those with university degrees accounted for 19.7%. The number of mammography studies was proportionally similar among the three schooling groups regardless of the schooling level. In the primary grade schooling group, 55 workers underwent 145 mammography studies, corresponding to 2.63 studies/worker on average; 19 workers of the high-school grade group underwent 55 studies (an average of 2.89 studies/worker); and 18 workers of the university degree group underwent 47 studies (an average of 2.89 studies/worker), as shown on Figure 1. 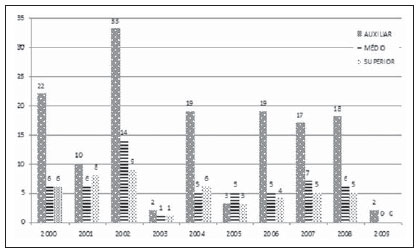 Figure 1. Mammography distribution by schooling level. When asked about the periodicity of mammography studies, 48 workers responded that they underwent the exams periodically, while 43 responded negatively. Among the 48 workers who responded that they underwent the examination periodically, six (12.6%) did so by medical request, 23 (47.9%) did so for understanding the importance of the study, two (4.1%) for presenting familial history of cancer, and 17 (35.4%) for considering mammography as being a routine procedure, with 27 (56.2%) of those 48 workers belonging to the primary grade schooling group, 11 (22.9%) to the high-school grade group, and 10 (20.9%) to the university degree group. The workers who declared to periodically undergo mammography studies reached 52.7% of the study sample and of those individuals, 47.9% undergo mammography studies for understanding its importance, while 35% do it as routine. Figure 2 shows the found data. 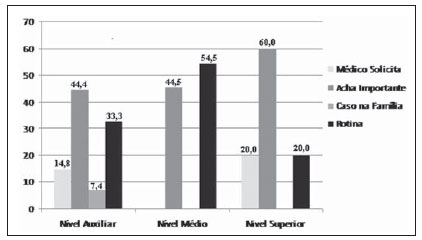 Figure 2. Justification for the performance of mammography study. The reasons for non-compliance with mammography periodicity by 43 workers are shown on Figure 3. The authors have found that 16 (37.3%) of them did not undergo the exam for lack of a doctor's request, nine (20.9%) for being unable to schedule the exams at SUS, eight (18.6%) for being afraid of undergoing the study, 10 (23.2%) for considering the study unnecessary and for not understanding its importance. Among these 43 workers, 27 (62.8%) belonged to the primary grade schooling group, eight (18.6%) to the high-school grade group, and eight (18.6%) to the university degree group. 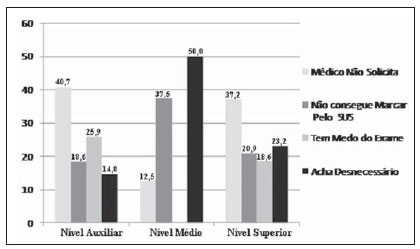 Figure 3. Justification for not undergoing the mammography study. DISCUSSION The participation of 91 (20%) workers out of a total of 436 individuals was obtained in the present study, a percentage that is considerably below the target of 70% established by the Healthy People 2010 document(6). A study developed by Godinho & Koch(7) has revealed that 80% of mammography studies in two investigated centers were not performed because of failures in the process of screening for breast cancer by the assisting physician. Luna & Koch(8), aiming at standardizing mammographic reports, have sent questionnaires and obtained 19.6% participation. The results of such casuistry were the same found in the present study. Ramos et al.(9) have reported the difficulty of a large part of the population in accessing the prevention centers by lack of resources and for the incapacity of SUS to meet the demand with specialized and appropriate support for diagnosis and treatment of neoplasms. The present study contradicts such data, as a satisfactory participation in the performance of mammography studies was not obtained, in spite of the opportunity and ease for the performance of such exams in the hospital environment where such women develop their activities. It is important to highlight that none of the workers participating in the present study was covered by a private health insurance plan. There is also a consensus that the lack of access to health services is one of the most important causative factor of the disease progression(10). The fact that the socioeconomic level is one of the determining factors in the compliance with preventive measures for breast cancer(11) was not conclusive in the present study. As regards schooling, Molina et al.(12) have pointed out as a significant factor the fact that women with more years of schooling would have better opportunities for early diagnosis of breast cancer for being better informed and for having private health insurance coverage. The coverage for mammography reaches 72% in the group with private health insurance coverage, a similar coverage level to that of the North- American female population(13). The results in the present study do not confirm such data, as the highest adherence level was observed among those workers with less years of schooling. With the present study, one can observe that adherence to the program of breast cancer screening was poor in spite of the fact that the studied population actually worked in the same environment where they could be treated, thus facilitating early diagnosis and treatment. Rezende et al.(10) has demonstrated a strong association of the time elapsed between the onset of the disease and the first clinical consultation. The interval between the first consultation and the diagnosis was greater than 6.5 months for half of the women, indicating slowness of the municipality health system(10). The number of workers who mentioned that they did not undergo mammography periodically corresponded to 47.2%, and of those workers, 37.3% reported that the physician was accountable for not requesting the study. The medical recommendation is the strongest predictor in the performance of mammography(14), followed by considering the study as being unnecessary, ignoring its importance (23.2%). Such data corroborate the findings of Godinho & Koch(7). Probably, the habit of not visiting the physician and considering the exam as "unnecessary" result from a failure in the process of patient guidance by the assisting physician. The data reinforce the findings of Koch & Peixoto(15) who found that, in a breast cancer screening program, a high number of the interviewed women had not been previously submitted to mammography, either because the physician had not requested the study or because they considered it as unnecessary at the time of the request. The workers who are unable to schedule mammography at SUS reached 16.6%, even when working at the very institutions where the exams are performed. According to the present results, one observes that the preventive actions have demonstrated to be limited and not compatible with the actual needs of the female population at higher risk levels considering the knowledge of the need to undergo mammography with the proper periodicity. The lack of adherence to periodical screening for a given condition impairs its early detection(16). The absence of studies on the prevention of breast cancer among health professionals was the main stimulus for the present study, showing the analysis at different schooling levels. Negative, positive and significant associations in the performance of mammography may explain the poor adherence to screening programs. CONCLUSION The adherence to the breast cancer screening program by means of mammography was poor. Female workers in a university hospital lack awareness on the prevention of such severe disease, whose detection at early stages increases healing rates and patients survival. The found reasons for the non-adherence were claims of the lack of request by physicians and absence of knowledge on the relevance of the study, even considering the fact that all participants worked in a hospital environment. GENERAL IMPACT AND RELEVANCE Even working in a university hospital with a breast cancer prevention program by means of mammography, the female personnel did not know how important mammography is for the early diagnosis of the disease. The present study demonstrates the importance of information and publicizing, particularly within the very health care institutions. It is clear that it is important to carry out campaigns in the health care institutions, particularly in large hospitals. REFERENCES 1. Leavell S, Clark EG. Medicina preventiva. São Paulo, SP: McGraw Hill; 1976. 2. Thuler LC. Considerações sobre a prevenção do câncer de mama feminino. Rev Bras Cancerol. 2003;49:227-38. 3. [No authors listed]. 16-year mortality from breast cancer in the UK Trial of Early Detection of Breast Cancer. Lancet. 1999;353:1909-14. 4. Sclowitz ML, Menezes AMB, Gigante DP, et al. Condutas na prevenção secundária do câncer de mama e fatores associados. Rev Saúde Pública. 2005;39:340-9. 5. Oliveira CC, Portão RAA, Gomes EB. A outra face da moeda: construção do cuidado de si. Saúde Coletiva: Coletânea. 2007;1(1). 6. Centers for Disease Control and Prevention. Healthy people 2010. [acessado em 5 de julho de 2010]. Disponível em: http://www.cdc.gov/nchs/healthy_people/hp2010.htm 7. Godinho ER, Koch HA. O perfil da mulher que se submete a mamografia em Goiânia - uma contribuição a "Bases Para um Programa de Detecção Precoce do Câncer de Mama". Radiol Bras. 2002;35:139-45. 8. Luna M, Koch HA. Avaliação dos laudos mamográficos: padronização prática de recomendação de conduta para um programa de detecção precoce do câncer de mama por meio da mamografia. Rev Bras Mastologia. 2002;12:7-12. 9. Ramos C, Carvalho JEC, Mangiacavalli MASC. Impacto e (i)mobilização: um estudo sobre campanhas de prevenção ao câncer. Ciênc Saúde Coletiva. 2007;12:1387-96. 10. Rezende MCR, Koch HA, Figueiredo JA, et al. Causas do retardo na confirmação diagnóstica de lesões mamárias em mulheres atendidas em um centro de referência do Sistema Único de Saúde no Rio de Janeiro. Rev Bras Ginecol Obstet. 2009;31:75-81. 11. O'Malley MS, Earp JA, Hawley ST, et al. The association of race/ethnicity, socioeconomic status, and physician recommendation for mammography: who gets the message about breast cancer screening? Am J Public Health. 2001;91:49-54. 12. Molina L, Dalben I, De Luca L, et al. Análise das oportunidades de diagnóstico precoce para as neoplasias malignas de mama. Rev Assoc Med Bras. 2003;49:185-90. 13. Szwarcwald CL, Leal MC, Gouveia GC, et al. Desigualdades socioeconômicas em saúde no Brasil: resultado da Pesquisa Mundial de Saúde, 2003. Rev Bras Saúde Matern Infant. 2005;5(Supl 1):S11-22. 14. Lima-Costa MF, Matos DL. Prevalência e fatores associados à realização da mamografia na faixa etária de 50-69 anos: um estudo baseado na Pesquisa Nacional por Amostra de Domicílios (2003). Cad Saúde Pública. 2007;23:1665-73. 15. Koch HA, Peixoto JE. Bases para um programa de detecção precoce do câncer de mama por meio da mamografia. Radiol Bras. 1998;31:329-37. 16. Canadian Task Force on Preventive Health Care Force [acessado em 2 de fevereiro de 2010]. Disponível em: http://www.canadiantaskforce.ca:80/ 1. Master, Biologist, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. 2. Master, MD, Radiologist at Instituto Nacional de Câncer (INCA), Rio de Janeiro, RJ, Brazil. 3. PhD, Professor, Department of Radiology, School of Medicine, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. 4. Full Professor, Program of Post-Graduation in Medicine (Radiology), School of Medicine, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. Mailing Address: Dra. Adeli Cardoso de Azevedo Rua Sabino Ribeiro, 72, casa 1, Irajá Rio de Janeiro, RJ, Brazil, 1235-360 E-mail: adelisimao@gmail.com Received February 11, 2012. Accepted after revision June 1st, 2012. Study developed at Hospital Universitário Clementino Fraga Filho (HUCFF) - Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554