Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 5 - Sep. / Oct. of 2007
Vol. 40 nº 5 - Sep. / Oct. of 2007
|
REVIEW ARTICLE
|
|
Three-dimensional ultrasound in the assessment of fetal limb volume |
|
|
Autho(rs): Edward Araujo Júnior, Márcio Fragoso Vieira, Luciano Marcondes Machado Nardozza, Hélio Antônio Guimarães Filho, Cláudio Rodrigues Pires, Antonio Fernandes Moron |
|
|
Keywords: Three-dimensional ultrasound, Fetal limbs, Volume |
|
|
Abstract:
Edward Araujo JúniorI; Márcio Fragoso VieiraII; Luciano Marcondes Machado NardozzaIII; Hélio Antônio Guimarães FilhoIV; Cláudio Rodrigues PiresV; Antonio Fernandes MoronVI
INTRODUCTION Fetal growth deviations are significant causes of increase in the rates of perinatal morbidity and mortality. Poor neonatal results may be a consequence of fetal macrosomia (labor traumatism) and intrauterine growth restriction (asphyxia)(1,2). Fetal limbs volume has been associated with the fetal growth and nutritional status(3). Initially, the fetal thigh volume (TVol) and arm volume (AVol) measurements were indirectly performed by means of two-dimensional ultrasound (2D US). However, 2D US cannot provide an accurate measurement of fetal limb volume. The majority of studies on fetal limbs volume evaluation by 2D US calculate the volume based on a cross sectional area in only one cutting plane that may not be the most appropriate, so the calculation is subject to error(4,5). In another study, arm and thigh volumes were assumed as if they were cylindrical(3), which obviously does not correspond to the reality. With the arrival of three-dimensional ultrasonography (3D US), the accuracy of this method for volumetric evaluation of several organs has been demonstrated(6-8). Considering that thigh and arm volumes are parameters that are well established as markers for fetal growth and nutrition, several studies have utilized these limbs volume as a predictor for birth weight, with more reliable results than those from the traditional formulas utilized by 2D US(911). Similar results have been obtained only from the partial limb volume, called "fractional limb volume"(12). Most recently, fetal soft tissue (subcutaneous and muscles) has been evaluated with basis on the factional arm and thigh volumes in an attempt to early detect growth deviations in fetuses at risk of intrauterine growth deviations(13,14). The first study about normality curve of the arm volume utilizing 3D US along pregnancy was published in 2002, while for thigh volume it occurred in 2003, both studies performed by a same group of investigators(15,16). In these studies, as well as in all of the other studies about estimation of fetal limb volume by 3D US, the multiplanar mode was utilized for volume calculation. This technique consists of defining parallel planes of an organ along an axis, while its external delineation is performed on another axis. The intervals between planes are defined by the very operator, with a different area being assigned for each plane. At the end of the process, the structure volume is automatically calculated by a built-in computer(17). Recently, fetal TVol and AVol measured by means of 3D US have been utilized in the prediction of intrauterine growth restriction (IUGR), and have shown to be promising parameters for the diagnosis of this disorder(18,19). The present review is aimed at showing the most up-to-date developments in terms of assessment of fetal limb volume by means of 3D US, such as normality curves during gestation, their relevance in the prediction of birth weight, and, currently, the possibility of intrauterine monitoring of subcutaneous and muscular tissues development, emerging as the most efficient method for early diagnosis of fetal growth deviations that may really contribute for a decrease in the perinatal morbidity and mortality rates.
3D ULTRASOUND AND FETAL ARM VOLUME The first normality curve of fetal arm volume was elaborated by Chang et al.(15). These authors have developed a prospective and cross-sectional study with 206 healthy pregnant women between 20 and 40 gestational weeks. The technique for AVol measurement was based on the multiplanar method, that is to say, a 3D scan of the arm is performed utilizing the plane for humeral measurement as a reference. After that, the cursor is moved at 3.0 intervals on the sagittal axis, and simultaneously the arm is axially delineated. The authors have observed that the fetal AVol is highly correlated with the gestational age (GA), and no statistically significant difference in interobserver error was found. The authors conclude that the normality curve of the fetal AVol assessed by 3D US may serve as a reference for evaluating the fetal growth and nutritional status. The first attempt to establish the accuracy of the AVol assessed by 3D US in the prediction of the birth weight was reported in a study developed by Liang et al.(10). These authors have developed a prospective study with 105 normal pregnant women, calculating the birth weight prediction on the basis of the usual 2D US tables and the fetal AVol, with all of the measurements performed up to 48 hours before the infants delivery. The technique utilized for AVol assessment was the same previously described. The authors have observed that the formula based on the fetal AVol for birth weight prediction was more accurate, considering the lower absolute error and absolute percent error. They conclude that the fetal arm volume assessed by 3D US is accurate for birth weight prediction, although highlighting the need for further casuistics for an actual formula validation. Lee et al.(12) have tried to validate the reliability of the fractional fetal limb volume assessed by 3D US for birth weight prediction. One hundred fetuses were prospectively evaluated by 2D and 3D ultrasonography up to four days before the infants delivery. Fractional fetal limb volumes were based on 50% of the humerus and femur diaphyseal lengths calculated by the multiplanar method through five consecutive scans at the level of the transverse section of the limb. This new model has been compared with the Hadlock formula in 30 fetuses(20). The authors have observed that the new prediction model was more accurate than the Hadlock model, correctly predicting 20 of 30 birth weights to within 5% of the actual weight. They have concluded that this new method is valid for birth weight prediction, highlighting the need for including soft tissue evaluation in the formula for birth weight prediction. The above mentioned authors have reported that the diagnosis of fetal growth deviation should not be based on cross-sectional studies, considering the biological variations and different genetic growth potentials of the fetuses. They have proposed three new growth parameters for an individual growth assessment based on the Rossavik growth model: fractional AVol, arm circumference and humeral diaphysis length(21). The technique for fractional AVol assessment is the same previously described. The authors have observed that up to the 28th gestational week, there is a linear growth of these three parameters, and afterwards, an accelerate deposition of subcutaneous and muscular tissues in fetuses presenting with normal growth rates. They conclude that the fractional fetal AVol can detect early changes in soft tissues; therefore this is an important parameter for early detection of fetal growth deviations(14). Chang et al.(18) have evaluated the efficacy of the fetal AVol measured by 3D US for predicting IUGR. They have performed a cross sectional study of 40 fetuses with IUGR and 442 fetuses without IUGR. Fetal limb volumes were calculated by the multiplanar method. The 10th percentile of the fetal AVol was utilized as the best parameter for prediction of IUGR with 97.5% sensitivity, 92.8% specificity, 54.9% positive predictive value, 99.8% negative predictive value, and 93.1% accuracy. Besides, the AVol has shown to be a better parameter for predicting IUGR than the biparietal diameter (BPD), the occipitofrontal diameter (OFD), the head circumference (HC), the abdominal circumference (AC), the femoral length (FL), and the estimated fetal weight (EFW). They conclude that the fetal AVol measured by 3D US can be utilized for predicting fetal IUGR during the prenatal period.
3D ULTRASOUND AND FETAL THIGH VOLUME Chang et al.(16) have published the first study on normality curve of TVol. They have developed a cross-sectional prospective study with 204 normal pregnant women between the 20th and 40th gestational weeks. For the TVol assessment, the multiplanar mode was utilized, that is to say, a 3D scan of the thigh is performed utilizing the plane for femoral measurement as a reference. After that, the cursor is moved at 3.0 intervals on the sagittal axis, and simultaneously the thigh is axially delineated. The authors have observed that the fetal TVol is highly correlated with the gestational age (GA) and with the following fetal growth parameters: biparietal diameter (BPD), occipitofrontal diameter (OFD), head circumference (HC), abdominal circumference (AC), femoral length (FL), and estimated fetal weight (EFW). They conclude that the fetal TVol is a reliable parameter for evaluation of the fetal growth and nutritional status during pregnancy. Chang et al.(9) have compared the fetal TVol accuracy for birth weight prediction, with other 2D US formulas usually utilized for birth-weight prediction(20,22,23). The authors have analyzed the TVol in 100 fetuses 48 hours before the infants delivery. The technique utilized for TVol assessment is the same previously described. They have observed that the TVol is highly correlated with the birth-weight. Error, percent error, absolute error and absolute percent error in TVol assessment by 3D US were lower than those resulting from the formulas utilized by 2D US. The authors conclude that the fetal TVol is more accurate for birth weight prediction when assessed by means of 3D US than by 2D US. However, they highlight the need for large-scale prospective studies to validate such conclusions. A new technique for TVol assessment by means of 3D US has been proposed by Song et al. for birth weight prediction(11). This technique consists of moving the cursor along the femur at three points (proximal, middle and distal diaphysis), and simultaneously the thigh is manually delineated in the axial plane. These measurements were compared with those performed by means of 2D US(24,25). The authors have evaluated 84 fetuses, and all the infants were delivered within 48 hours after ultrasound examination. They have concluded that the TVol assessed by this method was more accurate than the traditional 2D formulas for birth weight prediction. Also, the short data acquisition time by this method (about two minutes) is mentioned as an advantage, considering that the technique developed by Chang et al.(9) has taken 10 to 15 minutes (Figure 1).
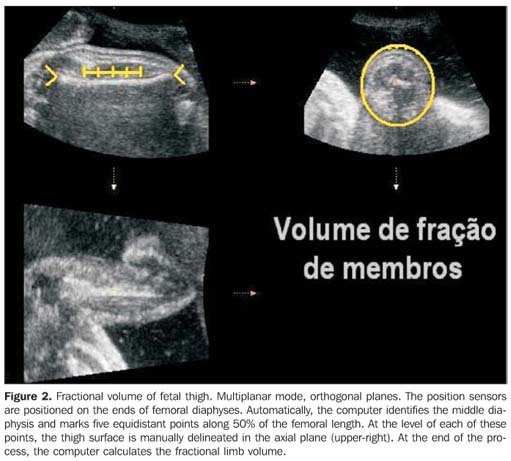
Lee et al.(13) have introduced the fractional fetal TVol as a new parameter for individual assessment of fetal growth based on the Rossavik growth model(21) . Both the casuistic and the method are the same previously described(14). The authors have observed an accelerate deposition of subcutaneous and muscular tissues on the fetal thigh after the 28th gestational week. They conclude that the fractional fetal TVol is a very sensitive marker for soft tissues anomalies, and that these anomalies may characterize an early physiological adaptation that precedes the development of intrauterine growth restriction or macrosomia (Figure 2).
Chang et al.(19) have evaluated the efficacy of the fetal TVol measured by 3D US for predicting IUGR. They have performed a prospective, cross sectional study of 30 fetuses with IUGR and 282 fetuses without IUGR. Volumetric measurements were calculated by the multiplanar method. The 10th percentile of the fetal TVol was utilized as the best parameter for prediction of IUGR with 86.6% sensitivity, 91.1% specificity, 51% positive predictive value, 98.5% negative predictive value, and 90.7% accuracy. They conclude that the fetal TVol measured by 3D US can be utilized for predicting fetal IUGR during the prenatal period.
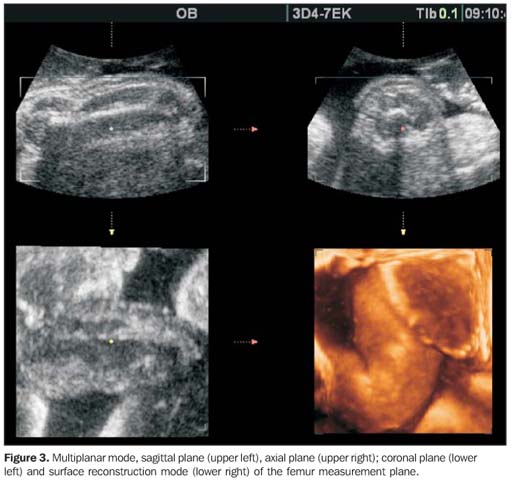
MULTIPLANAR METHOD For demonstrating the multiplanar method, we have utilized the technique developed by Chang et al.(9) for measurement of fetal TVol. The thigh image acquisition is performed during fetal rest, with a Sonoace 8000Live (Medison, Seoul, Korea) with a convex volumetric transducer for automatic scan (C3-7ED) Initially, a real time 2D scan is performed for determining the standard plane of femur measurement that will be considered as the region of interest (ROI). Then, the 3D scan is automatically performed (at a 60º angle, in four seconds). After that, the multiplanar mode is obtained: sagittal plane or A, transverse plane or B, and coronal plane or C (Figure 3).
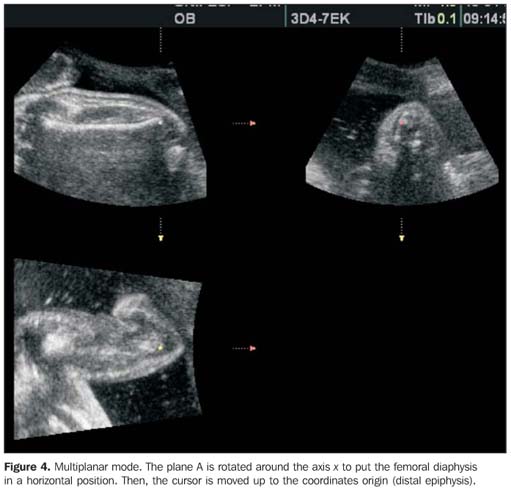
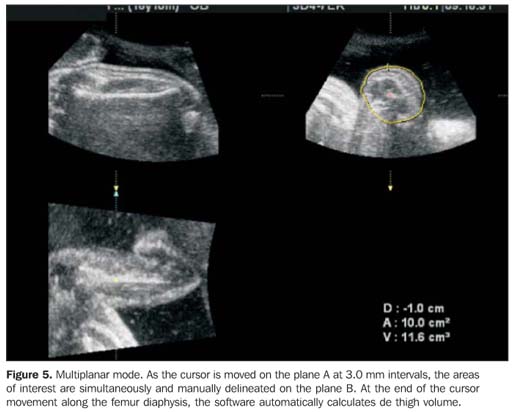
The plane A is selected, and the thigh is rotated around the axis x to put the femoral diaphysis in a horizontal position. The thigh is moved, so the proximal epiphysis is positioned on the coordinates origin (Figure 4). Then, the cursor is moved along the femur diaphysis up to the proximal epiphysis at 3.0 mm intervals. Simultaneously, the B image (transverse plane) is manually delineated as the cursor is moved, and a new area of interest is defined. At the end of the cursor movement, the fetal TVol is automatically calculated by the software (Figure 5). The TVol assessment by this technique takes, on average, 10 minutes.
CONCLUSIONS The arrival of the 3D US has allowed a more accurate volumetric assessment of several fetal organs, for an earlier and more precise diagnosis of fetal growth and developmental deviations. On the other hand, the fetal limb volume assessed by 3D US reflects the intrauterine growth and nutritional status, predicting the fetal birth weight with higher accuracy. In our country, where the incidence fetal growth restriction is high, with poor access to a skilled neonatal assistance, a higher dissemination of this 3D method for fetal limb volume evaluation would be of high relevance for a better support to neonates at risk, contributing definitely to reduce the rates of perinatal morbidity and mortality. However, it is important to note that high costs and poor training make a higher dissemination of the method difficult to occur.
REFERENCES 1. Roth S, Chang TC, Robson S, Spencer JA, Wyatt JS, Stewart AL. The neurodevelopmental outcome of term infants with different intrauterine growth characteristics. Early Hum Dev 1999;55: 39–50. [ ] 2. Dashe JS, McIntire DD, Lucas MJ, Leveno KJ. Effects of symmetric and asymmetric fetal growth on pregnancy outcomes. Obstet Gynecol 2000; 96:321–327. [ ] 3. Jeanty P, Romero R, Hobbins JC. Fetal limb vo lume: a new parameter to assess fetal growth and nutrition. J Ultrasound Med 1985;4:273–282. [ ] 4. Warda A, Deter RL, Duncan G, Hadlock FP. Evaluation of fetal thigh circumference measurements: a comparative ultrasound and anatomical study. J Clin Ultrasound 1986;14:99–103. [ ] 5. Vintzileos AM, Campbell WA, Rodis JF, Bors-Koefoed R, Nochimson DJ. Fetal weight estimation formulas with head, abdominal, femur, and thigh circumference measurements. Am J Obstet Gynecol 1987;157:410–414. [ ] 6. Chang FM, Hsu KF, Ko HC, et al. Fetal heart volume assessment by three-dimensional ultrasound. Ultrasound Obstet Gynecol 1997;9:42–48. [ ] 7. Laudy JAM, Janssen MMM, Struyk PC, Stijnen T, Wallenburg HC, Wladimiroff JW. Fetal liver volume measurement by three-dimensional ultrasonography: a preliminary study. Ultrasound Obstet Gynecol 1998;12:93–96. [ ] 8. Chang CH, Yu CH, Chang FM, Ko HC, Chen HY. Assessment of fetal adrenal gland volume using three-dimensional ultrasound. Ultrasound Med Biol 2002;28:1383–1387. [ ] 9. Chang FM, Liang RI, Ko HC, Yao BL, Chang CH, Yu CH. Three-dimensional ultrasound-assessed fetal thigh volumetry in predicting birth weight. Obstet Gynecol 1997;90:331–339. [ ] 10. Liang RI, Chang FM, Yao BL, Chang CH, Yu CH, Ko HC. Predicting birth weight by fetal upper-arm volume with use of three-dimensional ultrasonography. Am J Obstet Gynecol 1997;177: 632–638. [ ] 11. Song TB, Moore TR, Lee JI, Kim YH, Kim EK. Fetal weight prediction by thigh volume measurement with three-dimensional ultrasonography. Obstet Gynecol 2000;96:157–161. [ ] 12. Lee W, Deter RL, Ebersole JD, Huang R, Blanckaert K, Romero R. Birth weight prediction by three-dimensional ultrasonography: fractional limb volume. J Ultrasound Med 2001;20:1283–1292. [ ] 13. Lee W, Deter RL, McNie B, et al. Individualized growth assessment of fetal soft tissue using fractional thigh volume. Ultrasound Obstet Gynecol 2004;24:766–774. [ ] 14. Lee W, Deter RL, McNie B, et al. The fetal arm: individualized growth assessment in normal pregnancies. J Ultrasound Med 2005;24:817–828. [ ] 15. Chang CH, Yu CH, Chang FM, Ko HC, Chen HY. Assessment of normal fetal upper arm volume by three-dimensional ultrasound. Ultrasound Med Biol 2002;28:859–863. [ ] 16. Chang CH, Yu CH, Chang FM, Ko HC, Chen HY. Three-dimensional ultrasound in the assessment of normal fetal thigh volume. Ultrasound Med Biol 2003;29:361–366. [ ] 17. Riccabona M, Nelson TR, Pretorius DH. Three-dimensional ultrasound: accuracy of distance and volume measurements. Ultrasound Obstet Gynecol 1996;7:429–434. [ ] 18. Chang CH, Yu CH, Ko HC, Chen CL, Chang FM. Fetal upper arm volume in predicting intrauterine growth restriction: a three-dimensional ultrasound study. Ultrasound Med Biol 2005;31: 1435–1439. [ ] 19. Chang CH, Yu CH, Ko HC, Chen CL, Chang FM. The efficacy assessment of thigh volume in predicting intrauterine fetal growth restriction by three-dimensional ultrasound. Ultrasound Med Biol 2005;31:883–887. [ ] 20. Hadlock FP, Harrist RB, Sharman RS, Deter RL, Park SK. Estimation of fetal weight with the use of head, body, and femur measurements – a prospective study. Am J Obstet Gynecol 1985;151: 333–337. [ ] 21. Deter RL, Rossavik IK, Harrist RB, Hadlock FP. Mathematic modeling of fetal growth: development of individual growth curve standards. Obstet Gynecol 1986;68:156–161. [ ] 22. Warsof SL, Gohari P, Berkowitz RL, Hobbins JC. The estimation of fetal weight by computer-assisted analysis. Am J Obstet Gynecol 1977;128: 881–892. [ ] 23. Thurnau GR, Tamura RK, Sabbagha R, et al. A simple estimated fetal weight equation based on real-time ultrasound measurements of fetuses less than thirty-four weeks' gestation. Am J Obstet Gynecol 1983;145:557–561. [ ] 24. Hadlock FP, Harrist RB, Carpenter RJ, Deter RL, Park SK. Sonographic estimation of fetal weight. The value of femur length in addition to head and abdomen measurements. Radiology 1984; 150:535–540. [ ] 25. Shepard MJ, Richards VA, Berkowitz RL, Warsof SL, Hobbins JC. An evaluation of two equations for predicting fetal weight by ultrasound. Am J Obstet Gynecol 1982;142:47–54. [ ]
Received September 5, 2005. Accepted after revision September 22, 2005.
* Study developed at the Unit of 3D Ultrasound, Department of Obstetrics - Universidade Federal de São Paulo/Escola Paulista de Medicina (Unifesp/EPM), São Paulo, SP, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554