Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 4 - July / Aug. of 2007
Vol. 40 nº 4 - July / Aug. of 2007
|
CASE REPORT
|
|
External laryngocele: sonographic appearance - a case report |
|
|
Autho(rs): Marco da Cunha Pinho, Publio César Viana, Mauricio Omokawa, Cezar Simões, Eloisa M.M. Santiago Gebrim, Giovanni Guido Cerri, Maria Cristina Chammas |
|
|
Keywords: Laryngocele, Cervical mass, Ultrasonography, Laryngoscopy |
|
|
Abstract:
IMDs, Ex-Residents, Department of Radiology, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HC-FMUSP), São Paulo, SP, Brazil
INTRODUCTION The laryngeal ventricles constitute a recess located betweenthe false vocal cords above and the true vocal cords below. Theanterosuperior aspect of this recess ends in a blind pouch calledlaryngeal saccule that extends upward through the paralaryngealspace, laterally limited by the thyrohyoid cartilage, andmedially by the laryngeal wall(1–3). They varyin size (5–15 mm in length), and typically may be observed in upto 30% of the adult population on routine computed tomography(CT) studies(1). Laryngocele can be defined as an abnormal dilatation orherniation of the laryngeal saccule forming an air sac. When thiscavity is filled with mucus or pus, it is called respectivelylaryngomucocele and laryngopyocele. Laryngoceles are classified into internal, external and mixedor combined. Internal laryngocele is laterally limited by thethyrohyoid cartilage, and medially by the laryngealwall(4). When the hernial sac extends throughthe thyrohyoid membrane, proximal to the entry of the superiorlaryngeal vessels and nerves, it is classified as externallaryngocele. In the mixed or combined laryngocele both theinternal and external components arepresent(4). Some authors classify laryngocelesonly into external and internal, considering the term "mixed" asredundant because external laryngoceles always present anassociated internal component(5,6).Etiopathogenesis of laryngoceles is considered as multifactorial,and is related to the increase in the transglottic pressure, afactor usually present in glassblowers or musicians who play windinstruments(4,7). Typically, the incidence ishigher in white, male individuals, and most frequently isunilateral and combined(4). Laryngoceles appearance at CT and magnetic resonance imaging(MRI) has been already well characterized in theliterature(1–3,8), however few reports havedescribed their features atultrasonography(9,10). The present paperreports the case of a patient referred to the Department ofUltrasonography for cervical evaluation because of a palpablemass, the diagnosis of laryngocele being suggested with basis onsonographic findings.
CASE REPORT A male, 53-year-old patient has been referred to theDepartment of Ultrasonography of Instituto de Radiologia doHospital das Clínicas da Faculdade de Medicina daUniversidade de São Paulo, with a history of a painless,slow-growth cervical mass in the right submandibular region forone year. Additionally, the patient reported a progressivehoarseness developed during the same period. Symptoms likedyspnea or high dysphagia were absent. The mass was submitted tofine needle aspiration biopsy whose specimen was considered asunsatisfactory. Clinically, the patient presented with a soft, painless, compressible mass in the right submandibular region (Figure 1). Also, hoarseness and low vocal intensity were observed.
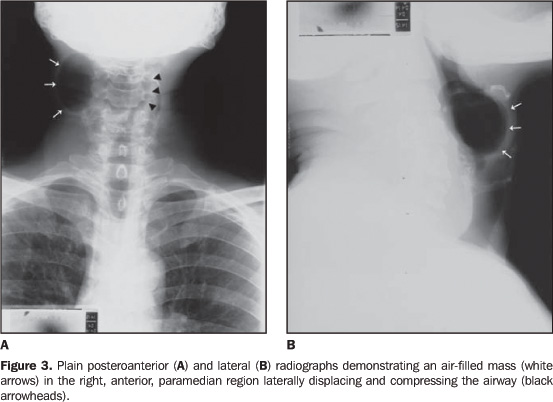
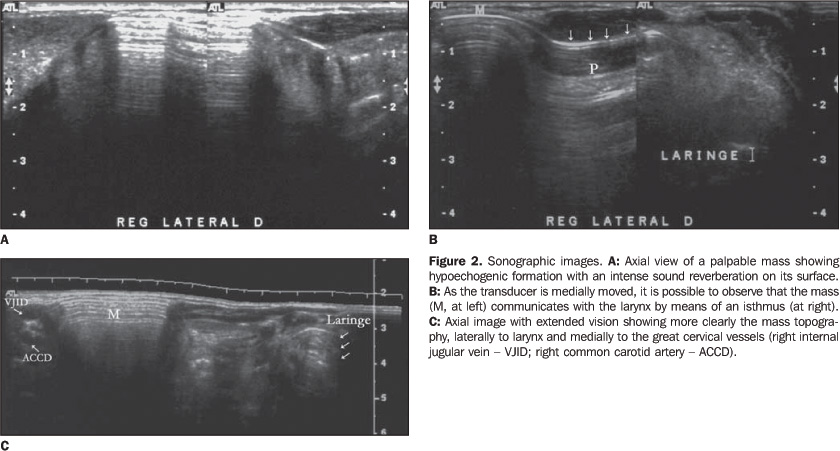
The ultrasound study demonstrated a superficial mass, just below the subcutaneous plane, in the right submandibular paramedian region, medial to the carotid bulb (Figure 2). The mentioned mass presented a surface with an intense soundreflection, and a large posterior reverberation artifact, so itsmeasurement as well as characterization of its deep portion wasdifficult. The described appearance suggested the presence of airwithin the lesion. Later in the study, an equally air-filledconnection was found between the mass and the larynx at the samelevel, suggesting the hypothesis of laryngocele. Plain posteroanterior and lateral radiographs have confirmed the hypothesis of external laryngocele at right (Figure 3).
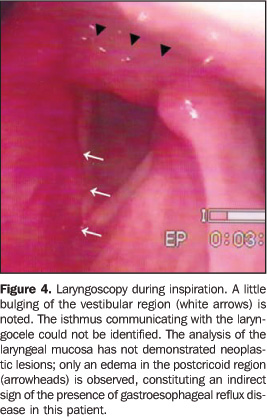
Subsequently, the patient was submitted to laryngoscopy that demonstrated a bulging of the right ventricular recess, without identification of the isthmus communicating with the laryngocele (Figure 4).
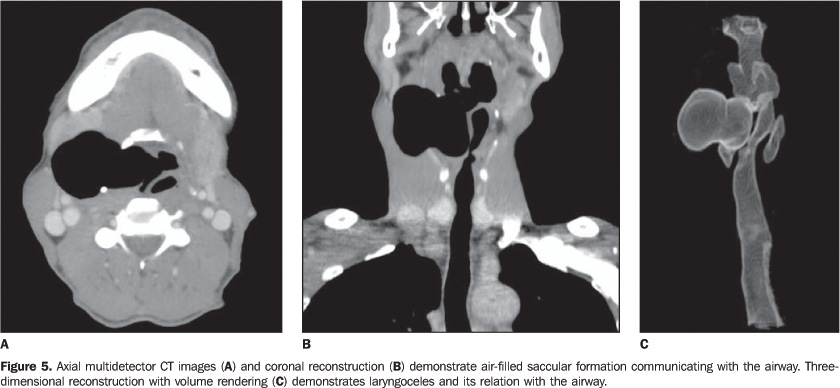
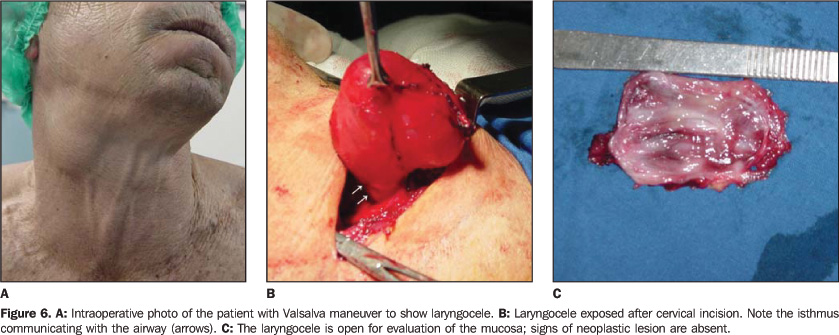
A CT study was requested for surgical planning and investigation of mucous lesions in the larynx, and a large laryngocele was clearly characterized, with no evidence of an obstructive factor (Figure 5). The patient was submitted to surgical intervention that confirmed the imaging findings (Figure 6).
DISCUSSION Laryngoceles etiopathogenesis is still to be determined.However, several theories try to explain the development of thedisease, from congenital predisposition to a multifactorialnature. The congenital theory suggests that in some cases, duringthe normal development of the larynx, between the second andthird gestational months, there is an abnormal growth of thesaccule (long saccule), and this is a predisposing factor for thefuture development of laryngocele. Other authors suggest that thestress caused by a continuous increased intralaryngeal pressureleads to the saccule dilatation and herniation. This theory issupported by the fact that laryngoceles are most frequently foundin musicians who play wind instruments and in patients withchronic respiratory diseases ("chronic coughers"). Although thisis the most accepted theory, some authors postulate that there isan association between congenital predisposition and prolongedexposure to high-pressure within the larynx. The clinical features of this entity are highly variable andnon-specific. Most frequently, it may be asymptomatic, and thediagnosis occurs incidentally during imaging studies for otherreasons or clinical suspicion, for example, staging of laryngealcarcinomas(8,11–13). In summary, symptoms may be divided into compressive, causedby internal laryngoceles, and those symptoms related to the masseffect, like in cases of external laryngoceles. Main complaintsamong patients are hoarseness and cough. On the other hand, somepatients with external laryngoceles report a palpable cervicalmass, and, less frequently, dysphagia and dyspnea, associated ornot with a peculiar professional or pathological history. Inpatients who present with a palpable cervical mass associatedwith inflammation, laryngoceles constitute an importantdifferential diagnosis. Imaging studies play a significant role in the diagnosis ofthis lesion, and many authors suggest that CT is the goldenstandard, with MRI playing an adjuvant role in the diagnosis oflaryngoceles. Ultrasonography is generally utilized for initial evaluationof cervical masses, mainly for differentiating the nature of thelesion as well as defining its contents andlocation(9,10). In the present case, the location, the presence of soundreverberation in the lesion, and the ventricular appendageextending toward the laryngeal wall have suggested thediagnosis. CT, not only suggests the diagnosis, but also may classify thelesion, and directly affect the therapeutic choice. This imagingmethod allows the visualization of the dilated air-filledsaccule, as well as its limits and anatomical relations. Inexternal laryngoceles, it may be observed that the hernial sacpasses through the thyrohyoid membrane, extending superiorly intothe paralaryngeal space. Sometimes, a causal factor, for example,a squamous-cell carcinoma located in the opening of the laryngealventricle, may be found (secondary laryngocele). In these cases,the tumor partially obstructs the communication between thesaccule and the larynx, creating a valve-like mechanism. Also, acystic lesion with soft-tissue attenuation may be observed,suggesting a diagnosis of laryngomucocele or laryngopyocele,depending on the clinical context. MRI is important, particularly in cases where laryngocele isassociated with a larynx squamous-cell carcinoma. This imagingmethod is useful to corroborate the diagnosis, in staging thetumor, for evaluating the disease extent in soft-tissues, as wellas to provide, by means of multiplanar acquisition, a bettersurgical timing planning by otolaryngologists and head and necksurgeons(8,12,14,15). Few reports describe possible appearance of laryngoceles atultrasonography(8,9). The commonestpresentation is a mass with an intense sound reflection,determining a posterior reverberation artifact, suggesting thepresence of air in the paramedian line. Sometimes, it is possibleto demonstrate the isthmus between the mass and the larynx so asto raise the diagnostic hypothesis of laryngocele. Maindifferential diagnoses in these cases, would be Zenker'sdiverticulum or an air-filled abscess. Additionally, a masspresenting hypo- or non-echogenic contents and posterior acousticshadowing may be characterized, defining the cystic nature of thelesion. Differential diagnoses of this mass range fromthyroglossal duct cyst (median line) to dermoid cyst, cystichygroma and abscess or lymphadenomegaly with liquefaction. Boththe patient's clinical condition and age constitute significantfactors when these hypotheses are considered.
REFERENCES 1. Swartz JD, D'Angelo AJ, Harnsberger HR, Zwillenberg S, Marlowe FI. The laryngeal mucocele. Imaging analysis of a rare lesion. Clin Imaging 1990;14:110–115. [ ] 2. Nazaroglu H, Ozates M, Uyar A, Deger E, Simsek M. Laryngopyocele: signs on computed tomography. Eur J Radiol 2000;33:63–65. [ ] 3. Kumar G, Bradley PJ, Wastie ML. Case of the month. What a blow! Laryngocele. Br J Radiol 1998;71:799–800. [ ] 4. Abrahão M, Santos RO, Cervantes O. Tratamento dos tumores benignos da laringe. In: Carvalho MB, organizador. Tratado de cirurgia de cabeça e pescoço e otorrinolaringologia. São Paulo, SP: Ateneu, 2001;905. [ ] 5. Curtin HD. The larynx. In: Som PM, Curtin HD, editors. Head and neck imaging. 4th ed. St. Louis, MO: Mosby, 2003;1595–1699. [ ] 6. Curé J. Laryngocele. In: Hansberger R, Wiggins R, Hudgins P, et al., editors. Diagnostic imaging: head and neck. 1st ed. Salt Lake City, UT: Amyrsys, 2004;III, 3–6. [ ] 7. Sobol SM, Bailey SB. Evaluation and surgical management of tumors of the neck: benign tumors. In: Thawley SE, Panje WR, Batsakis JG, Lindberg RD, editors. Comprehensive management of head and neck tumors. Philadelphia, PA: WB Saunders, 1999;1435–1439. [ ] 8. Harvey RT, Ibrahim H, Yousem DM, Weinstein GS. Radiologic findings in a carcinoma-associated laryngocele. Ann Otol Rhinol Laryngol 1996; 105:405–408. [ ] 9. Youssefzadeh S, Steiner E, Turetschek K, Gritzmann N, Kursten R, Franz P. The sonography of laryngeal cysts. Rofo 1993;159:38–42. [ ] 10. Heppt W, Born IA, Maier H. Use of B-mode sonography in the diagnosis of laryngocele. Laryngorhinootologie 1990;69:378–380. [ ] 11. Helmberger RC, Croker BP, Mancuso AA. Leiomyosarcoma of the larynx presenting as a laryngopyocele. AJNR Am J Neuroradiol 1996; 17:1112–1114. [ ] 12. Glazer HS, Mauro MA, Aronberg DJ, Lee JK, Johnston DE, Sagel SS. Computed tomography of laryngoceles. AJR Am J Roentgenol 1983;140: 549–552. [ ] 13. Celin SE, Johnson J, Curtin H, Barnes L. The association of laryngoceles with squamous cell carcinoma of the larynx. Laryngoscope 1991;101: 529–536. [ ] 14. Ettema SL, Carothers DG, Hoffman HT. Laryngocele resection by combined external and endoscopic laser approach. Ann Otol Rhinol Laryngol 2003;112:361–364. [ ] 15. Martinez Devesa P, Ghufoor K, Lloyd S, Howard D. Endoscopic CO2 laser management of laryngocele. Laryngoscope 2002;112(8 Pt 1):1426–1430. [ ]
Received April 20, 2005. Accepted after revision June 10, 2005.
* Study developed in the Division of Ultrasonography at Instituto de Radiologia do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (InRad/HC-FMUSP), São Paulo, SP, Brazil. |
|


{kind=link}
{kind=link}
{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554