Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 4 - July / Aug. of 2007
Vol. 40 nº 4 - July / Aug. of 2007
|
ORIGINAL ARTICLE
|
|
Brachial artery flow-mediated dilatation in women with rheumatoid arthritis |
|
|
Autho(rs): Pedro Teixeira Castro, Carlos Antônio Barbosa Montenegro, Antonio Carlos Pires Carvalho, Jorge Fonte de Rezende Filho, Washington Bianchi, Dante Valdetaro Bianchi, Sandra Pereira Leite |
|
|
Keywords: Rheumatoid arthritis, Endothelial dysfunction, Brachial artery flow-mediated dilatation |
|
|
Abstract:
IFellow Master Degree, Teaching Assistant, Faculdade de Medicina da Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
INTRODUCTION Rheumatoid arthritis is associated with high cardiovascularmorbimortality. Observational studies demonstrate a three to18-year decrease in life expectancy(1) infemale patients with rheumatoid arthritis, with cardiovasculardiseases accounting for 50% of mortality in thesepatients(2). With a higher incidence in women(2–5/1)(3), the relative risk of acutemyocardial infarct in female patients with rheumatoid arthritisis 2.0(4). Cardiovascular diseases in rheumatoid arthritis are associatedwith systemic inflammation and endothelial lesion. Traditionally,sedentarism, high body mass index and dyslipidemia are somecardiovascular risk factors, however they do not fully explainthe increase in cardiovascular diseasesincidence(5). The silent onset ofcardiovascular diseases occurs on arterial walls and progressesthrough well-known mechanisms including endothelial dysfunction,inflammation, plaque formation and vascular remodeling, lateratherosclerotic plaque rupture, andthrombosis(6). Endothelial dysfunction plays an important role in theformation of cardiovascular diseases(7) andcontributes for the atheroma plaque rupture that accounts for 70%of acute myocardial infarcts in asymptomaticpatients(8). The present study was aimed at evaluating theendothelium-dependent function by means of brachial arteryflow-mediated dilatation (FMD) in women with rheumatoidarthritis, comparing them with normal women. Firstly described in 1992, FMD evaluates the endothelialfunction with basis on the production of nitric-oxide released bythe endothelium after ischemic stimulus. This stimulus will causenitric oxide release and arterial dilatation that may be measuredby means of ultrasound(9). Later in the present study, we have compared the endothelialfunction with other method for evaluating inflammation andcardiovascular risk usually utilized in the clinical practice,the C-reactive protein test. FMD was correlated with C-reactiveprotein, age and duration of the disease in patients withrheumatoid arthritis.
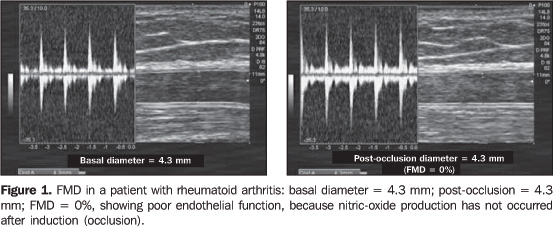
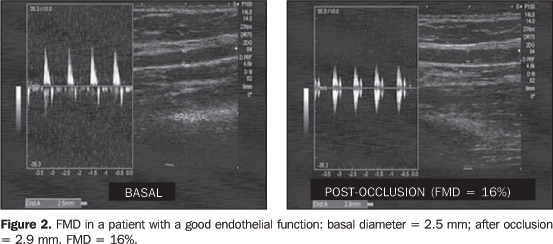
MATERIALS AND METHODS Sixty-eight patients (32 with rheumatoid arthritis and 36 in acontrol group) were examined. Because of the great FMD variationin results described in the literature(10), 36patients (control group) have been included for correlation ofendothelial function in these two groups. The control group hasincluded 36 women in the age range between 20 and 49 years. Allof the patients in this group were normotense, non-tobacco users,non-diabetic, were at menacme, with total cholesterol levels£ 200 mg/dl, and with no familiar history of vasculardiseases. Between March and August/2004, 32 patients diagnosed withrheumatoid arthritis by the Rheumatology Ambulatory at the 39thInfirmary of Santa Casa da Misericórdia do Rio de Janeirowere invited to participate in this study. Only five patients were male. Considering that FMD results areinfluenced by the sex of the patient(11), theauthors decided to exclude the male patients, limiting the studyto the female patients. The remaining 27 female patients withrheumatoid arthritis were selected according to the SociedadeBrasileira de Reumatologia (Brazilian Society of Rheumatology)criteria(12) for the diagnosis of rheumatoidarthritis. With ages between 26 and 71 years, the patients werenon-tobacco users and did not present other autoimmunediseases. Some of the patients were affected by other comorbidities, butthis was not taken into consideration in the present study,because the objective was to evaluate the inflammatory status ofrheumatoid arthritis. Besides, it is already known thatrheumatoid arthritis typically courses with these diseases.Disease intensity, clinical condition and antirheumatic drug usewere not evaluated. FMD is highly influenced by the patient'ssex, height and muscular mass, but not by theage(11). For analyzing the significance of the endothelial functionevaluation in these patients, C-reactive protein and FMD wereseparately compared. All of the patients were simultaneouslysubmitted to FMD and C-reactive protein test. All of the patients have agreed to participate in the presentstudy that was approved by the Committee for Ethics in Researchof our Institution. FMD was performed according to the already describedtechnique(13,14), with the patient in dorsaldecubitus, after rest, in a calm and controlled-temperatureenvironment. Medicines and food ingestion was not restricted,considering that the objective of the study was to evaluate thepatients in their daily habits. The identification of the rightbrachial artery was made with the aid of color Doppler, at 2 to 5cm above the cubital fold. A Toshiba Nemium equipment with a 14MHz, high resolution, B-mode, linear transducer was utilized. Thebrachial artery diameter is measured by calculating the distancebetween the proximal and distal (DI) intima at diastole. Ischemiais induced with pneumatic compression of the brachial artery forfive minutes, and the artery measurement is repeated between 60and 90 seconds after interruption of the compression (D2), in thediastole period, with the aid of pulsatile Doppler. Theendothelium-dependent function is defined by the formula: (D2 – D1)/D1 × 100 (Figures 1 and 2).
The higher is the numeric value of the study, the better isthe endothelial function. The present study has opted for notnumerically comparing the FMD with other studies. This is anoperator- and equipment-dependent method; besides, the numericalanalysis is subject to errors. For routine evaluation of the disease, C-reactive protein wastested after 12-hour fasting, with positive and quantitativeresults, in centesimal values above 0.01mg/dl. For this purpose,the APTEC kit (Selectra-Merck; Darmstadt, Germany) was utilized— with 0.01 mg/dl sensitivity; RV = 0.0–1.0 mg/dl; intrassayCV = 2.9% and interassay CV = 2.9%. Results were recorded on average (± standarddeviation). The difference between parameter for both groups wasevaluated by the Chi-square test. Calculations and statisticalanalyses were performed with the Statistical Package for theSocial Sciences (SPSS) for Windows version 11.0.0 (SPSS, Inc.;Chicago, IL, USA). The difference was considered as statisticallysignificant when p < 0.005.
RESULTS Mean ages varied significantly between groups. It is important to note that the control group was formed by women at menacme, considering that menopause is a risk factor for cardiovascular disease. Ages in the control group ranged between 22 and 42 (mean = 28.9 ± 7.1) years. In the rheumatoid arthritis, the ages ranged between 26 and 76 (mean = 49.9 ± 12.9) years. In this group, ages were significantly (p < 0.000) higher than in the control group (Graph 1).
The control group FMD was 23.24 (± 5.65)%, while in the rheumatoid arthritis was 5.65 (± 9.69)%, with a statistically significant difference (p < 0.000) (Graph 2).
Five patients failed to demonstrate vasodilation, with FMD equal or less than zero. Four of these patients were less than 50 years old, demonstrating that the FMD difference between the groups was not affected by the ages, as per Graph 3 (p = 0.001).
The C-reactive protein test result was 4.8 (± 9.1) mg/land disease duration of 6.2 (± 6.5) years. Correlation ofage, FMD, C-reactive protein and disease duration dig not showany significant result.
DISCUSSION The present study demonstrates that patients with rheumatoidarthritis present endothelial dysfunction, and FMD does notcorrelate with C-reactive protein, patient´s age anddisease duration. Early stages of atherosclerosis are usually found inimmunological and inflammatory diseases where cardiovascularcomplications resulting from the formation and rupture ofatherosclerotic plaques represent a relevant cause ofmorbimortality(15). Endothelial dysfunction is the earliest event in theatheromatous lesions formation, and its evaluation is a promisingtool for estimating coronary prognosis, especially in patientswith chronic inflammation, considering that a persistentdysfunction is a reason for an obscureprognosis(16). Although an ideal method for diagnosing endothelialdysfunction has not been established yet, there are evidencesthat FMD allows an adequate evaluation of the endothelialbehavior and reflects the coronary endothelial function andbehavior(17). Age does not affect the endothelial function evaluation withFMD, so the significant difference in the groups age analysisdoes not affect the data interpretation of age groups. This iscorroborated by the difference between patients with less than 50of age and those in the control group(11). Like the present study, other studies have found a significantendothelial dysfunction in patients with autoimmune diseases bymeans of FMD. The presence of systemic inflammation predisposesto atherosclerosis, affecting the endothelial function anddecreasing the production of nitric oxide by the endothelium.This decrease in the nitric oxide production leads to a smallerarterial dilatation upon induced ischemia. In a study evaluatingthe infliximab therapy in 11 patients with rheumatoid arthritis,once the inflammation decreased, there was an improvement in theFMD(18). In patients treated for rheumatoid arthritis, FMD was relatedto the HLA-DRB1 (human leukocyte antigen histocompatibility gene)and not to the clinical condition of thepatients(19). In a comparison of FMD results inpatients with rheumatoid arthritis with control paired by age andsex, patients with low levels of disease activity havedemonstrated a significant decrease in the endothelialfunction(20); however, one study has not founddifferences between patients with rheumatoid arthritis andcontrol group(14). FMD and C-reactive protein present correlation in healthyindividuals and in those with cardiovascular risk factors. An investigation evaluating seven cardiovascular risk markersin 2,113 subjects has demonstrated inverse correlation betweenFMD and C-reactive protein (the higher is the C-reactive proteinlevel, the lower is the nitric oxide production –FMD)(21). In a study evaluating the endothelium-dependent function inhealthy subjects, the C-reactive protein level has presented acorrelation with the FMD, but has not presented a closed relationbetween both methods in the evaluation of an inflammatory processin patients at low cardiovascular risk(22). In patients with coronary pathology, there was correlationbetween FMD and C-reactive protein in the23). The most surprising data is the non-correlation between FMDand C-reactive protein. The present study demonstrates that, evenin patients treated for rheumatoid arthritis and with normallevels of C-reactive protein, there is presence of systemicinflammation. The persistent and silent, systemic inflammationexposes a clinically managed patient to cardiovascular risk. Nitrate-mediated endothelium-independent vasodilation was notutilized. Sometimes, this control method is utilized to affirmthat the decrease in arterial dilatation is a result from theendothelial dysfunction, and not an arterial smooth muscledysfunction. With disparate results between C-reactive protein and FMD, wehave concluded that there is endothelial dysfunction in womenwith rheumatoid arthritis, and that the C-reactive protein leveldoes not provide an adequate evaluation of the cardiovascularrisk in these patients. Quyyumi(24) affirms that systemicinflammation markers like FMD, carotid media/intimal complex andpulse-wave analysis arise as methods for evaluating theatherosclerosis risk. He recommends the inclusion of thesemethods, including the biochemical ones, in randomized studiesfor screening and diagnosis of cardiovascular risk. Consideringthat a high level of systemic inflammation affects theendothelial function, inflammation markers like FMD may provide abetter evaluation of the cardiovascular risk in patients withrheumatoid arthritis. FMD is a promising method for evaluation ofinflammation(25) in the clinical practice, andmay be extended to patients with rheumatoid arthritis for directmeasurement of vascular physiopathology and preventivetherapeutic response.
REFERENCES 1. Sattar N, McCarey DW, Capell H, McInnes IB. Explaining how "high-grade" systemic inflammation accelerates vascular risk in rheumatoid arthritis. Circulation 2003;108:2957–2963. [ ] 2. DeMaria AN. Relative risk of cardiovascular events in patients with rheumatoid arthritis. Am J Cardiol 2002;89(6A):33D–38D. [ ] 3. Lee DM, Weinblatt ME. Rheumatoid arthritis. Lancet 2001;358:903–911. [ ] 4. Solomon DH, Karlson EW, Rimm EB, et al. Cardiovascular morbidity and mortality in women diagnosed with rheumathoid arthritis. Circulation 2003;107:1303–1307. [ ] 5. Wang L, Feng G. Rheumatoid arthritis increases the risk of coronary heart disease via vascular endothelial injuries. Med Hypotheses 2004;63:442–445. [ ] 6. Cohn JN. Introduction to surrogate markers. Circulation 2004;109(25 Suppl 1):IV-20–21. [ ] 7. Bugiardini R, Manfrini O, Pizzi C, Fontana F, Morgagni G. Endothelial function predicts future development of coronary artery disease: a study of women with chest pain and normal coronary angiograms. Circulation 2004;109:2518–2523. [ ] 8. Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation 2003;108:1664–1672. [ ] 9. Raitakari OT, Celermajer DS. Flow-mediated dilatation. Br J Clin Pharmacol 2000;50:397–404. [ ] 10. Bots ML, Westerink J, Rabelink TJ, de Koning EJ. Assessment of flow-mediated vasodilatation (FMD) of the brachial artery: effects of technical aspects of the FMD measurements on the FMD response. Eur Heart J 2005;26:363–368. [ ] 11. Schroeder S, Enderle MD, Baumbach A, et al. Influence of vessel size, age and body mass index on the flow-mediated dilatation (FMD%) of the brachial artery. Int J Cardiol 2000;76:219–225. [ ] 12. Laurindo IMM, Pinheiro GRC, Ximenes AC, et al. Consenso brasileiro para o diagnóstico e tratamento de artrite reumatóide. Rev Bras Reumatol 2002;42:355–361. [ ] 13. Corretti MC, Anderson TJ, Benjamin EJ, et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol 2002;39:257–265. [ ] 14. Kuscu NK, Kurhan Z, Yildirim Y, Tavli T, Koyuncu F. Detection of endothelial dysfunction in preeclamptic patients by using color Doppler sonography. Arch Gynecol Obstet 2003;268:113–116. [ ] 15. Van Doornum S, McColl G, Jenkins A, Green DJ, Wicks IP. Screening for atherosclerosis in patients with rheumatoid arthritis: comparison of two in vivo tests of vascular function. Arthritis Rheum 2003;48:72–80. [ ] 16. Verma S,Wang CH, Lonn E, et al. Cross-sectional evaluation of brachial artery flow-mediated vasodilation and C-reactive protein in healthy individuals. Eur Heart J 2004;25:1754–1760. [ ] 17. Widlansky ME, Gokce N, Keaney JF, Vita JA. The clinical implications of endothelial dysfunction. J Am Coll Cardiol 2003;42:1149–1160. [ ] 18. Hurlimann D, Forster A, Noll G, et al. Anti-tumor necrosis factor-alpha treatment improves endothelial function in patients with rheumatoid arthritis. Circulation 2002;106:2184–2187. [ ] 19. Gonzalez-Juanatey C, Llorca J, Testa A, Revuelta J, Garcia-Porrua C, Gonzalez-Gay MA. Increased prevalence of severe subclinical atherosclerotic findings in long-term treated rheumatoid arthritis patients without clinically evident atherosclerotic disease. Medicine (Baltimore) 2003;82: 407–413. [ ] 20. Vaudo G, Marchesi S, Gerli R, et al. Endothelial dysfunction in young patients with rheumatoid arthritis and low disease activity. Ann Rheum Dis 2004;63:31–35. [ ] 21. Kathiresan S, Gona P, Larson MG, et al. Cross-sectional relations of multiple biomarkers from distinct biological pathways to brachial artery endothelial function. Circulation 2006;113:938–945. [ ] 22. Williams IL, Chowienczyk PJ, Wheatcroft SB, et al. Effect of fat distribution on endothelial-dependent and endothelial-independent vasodilatation in healthy humans. Diabetes Obes Metab 2006;8: 296–301. [ ] 23. Kang SM, Chung N, Kim JY, et al. Relation of vasodilator response of the brachial artery to inflammatory markers in patients with coronary artery disease. Echocardiography 2002;19:661–667. [ ] 24. Quyyumi AA. Inflamed joints and stiff arteries: is rheumatoid arthritits a cardiovascular risk factor? Circulation 2006;114:1137–1139. [ ] 25. Faulx MD, Wright AT, Hoit BD. Detection of endothelial dysfunction with brachial artery ultrasound scanning. Am Heart J 2003;145:943–951. [ ]
Received September 3, 2006. Accepted after revision February 21, 2007.
* Study developed at Clínica de Ultra-sonografia Botafogo, in conjunction with the 39th Infirmary of Santa Casa da Misericórdia do Rio de Janeiro and Departamento de Radiologia da Faculdade de Medicina da Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554