Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 1 - Jan. /Feb. of 2007
Vol. 40 nº 1 - Jan. /Feb. of 2007
|
REVIEW ARTICLE
|
|
Imaging diagnosis of nasopharyngeal tumors |
|
|
Autho(rs): Ilka Yamashiro, Ricardo Pires de Souza |
|
|
Keywords: Computed tomography, Nasopharynx, Tumor, Carcinoma |
|
|
Abstract:
IMD, Trainee at Service of Diagnostic Imaging – Hospital Heliópolis Department of Radiology, Master Degree Student in Health Sciences at Hospital Heliópolis
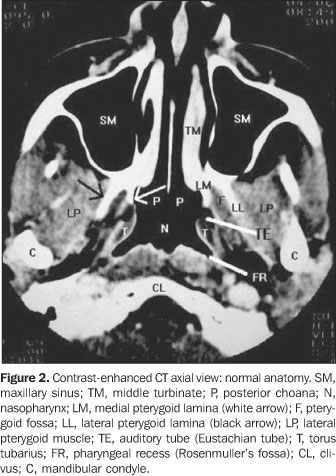
ANATOMICAL SUBSTRATE The nasopharynx is the upper part of the superior aerialtract, and corresponds to the superior end of the pharynx. Itcontains the lateral pharyngeal recess, the torus tubarius andthe pharyngeal tonsil. The nasopharynx is situated at the center of the skull base.The anatomical relations of the nasopharynx include the clivusposteriorly, the posterior nasal cavity anteriorly, and thecarotid spaces laterally. The inferior margin of the nasopharynxis a horizontal plane passing through the hard palate andpalatopharyngeal muscle. Laterally, it is limited by the marginsof the superior constrictor muscle, the pharyngobasilar fasciaand by the parapharyngeal space(1). Its wall isformed by three layers: a mucous lining, a muscular layer and afibrous membrane denominated pharyngobasilar fascia. It is approximately 2.0 cm in anteroposterior diameter andabout 4.0 cm in craniocaudal extent(2). The middle layer of the deep cervical fascia orbuccopharyngeal fascia is characterized by a condensation ofcellular tissue surrounding the lateral and posterior portions ofthe nasopharynx, providing it with a fascial limit as aninterface with the neighboring structures. It is a tender, subtlemembrane, and does not represent a significant barrier toneoplastic or infectious dissemination from the nasopharynx intoadjacent spaces(3,4). Laterally, it covers thepharynx, superiorly inserting into the skull base through thepharyngeal tubercle, with the superior constrictor muscle,pharyngobasilar fascia, and in the posterior margin of the medialpterygoid plate. The structural protrusion and the tissues of the pharyngeal wall give shape to the mucosal lining of the nasopharynx, determining anatomical landmarks utilized in clinical evaluations and interpretation of computed tomography (CT) and magnetic resonance imaging (MRI) cross-sectional slices, as follows: a) torus tubarius – is the most prominent of these structures, corresponding to a projection of the cartilaginous portion of the auditory tube. It is visualized as a protrusion projecting into the lateral wall of the nasopharyngeal cavity, both on CT and MRI; b) pharyngeal ostium of auditory tube – localized antero-inferiorly to the torus tubarius(5). On CT and MRI axial slices, it is observed as a small recess in the nasopharynx lateral wall; c) The salpingopharyngeal fold, a mucosal protrusion determined by the submucosal tract of the salpingopharyngeal muscle forming the anterior limit of the lateral pharyngeal recess; d) the lateral pharyngeal recess, posteriorly located, and extending superiorly to the salpingopharyngeal fold and torus tubarius (Figures 1 and 2). It is the most frequent site of origin for nasopharyngeal squamous cell carcinoma(6). It originates in a subtle mucosal herniation through the Morgagni sinus, a region on the pharyngeal wall where muscular fibers are absent. The degree of distensibility is highly variable. It tends towards being symmetrical, although subtle asymmetries are not uncommon to be found at MRI and CT(7). In youngsters, it presents with less amplitude because of the presence of retropharyngeal lymphoid tissue(8).
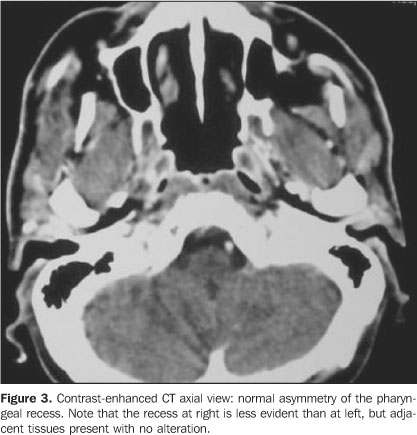
The nasopharynx is formed by: a) A muscular layer formed by the upper, middle and lowerpharyngeal constrictor muscles, pharyngeal levator muscles(palatopharyngeal, stylopharyngeal and salpingopharyngeal),palatoglossus, tensor palati and levator palati, and thepalatopharyngeal muscle; b) a fibrous structure or pharyngobasilar fascia situatedbetween the muscular tunica and mucosa, extending uninterruptedlyfrom the upper to the lower end of the pharynx, absent in theanterior portion, except in the attachment to the larynx where itis circular(1). Cranially, where its externalsurface is not covered by a muscular layer (between the skullbase and the inferolateral portion of the auditory tubecartilage), there is a lateral space denominated Morgagni sinus.It is through this space that the auditory tube and the levatorpalati penetrate into the nasopharynx internal portion. TheMorgagni sinus, because of its anatomical characteristic, is animportant route for the carcinoma dissemination from thenasopharynx towards adjacent spaces like the parapharyngealspace; c) a mucosal membrane or internal tunica lining internally thepharyngobasilar fascia, continuing with the mucosal lining of thenasal cavity and oropharynx. It is formed by ciliatedpseudo-stratified epithelium and chorium with a plenty ofmuciparous glands and lymphoid follicles(9).Abundant lymphoid tissue in the chorium forms a part of thepharyngeal lymphatic ring, a probable site for development ofnon-Hodgkin lymphoma, the most frequent malignant nasopharyngealneoplasm(2,10). Smaller salivary glands arepresent in the sub-mucosa surrounding the auditory tubes, andmight be a focus for benign or malignant nasopharyngeallesions. The knowledge of anatomical variations of this region isimportant to avoid confusion between normal alterations anddisease. Asymmetry of mucosal landmarks, especially the pharyngeal recess asymmetry, is a frequent variation. A decrease in depth of the pharyngeal recess, or even its collapse as a normal finding should be differentiated from disease. The analysis of adjacent, deep planes showing their integrity or symmetry suggests normality (Figure 3). Also, the acquisition of CT images during modified Valsalva maneuver or wide opening of the mouth might be useful. The modified Valsalva maneuver results in a maximum distention of the auditory tube ostium and pharyngeal recess. The wide opening of the mouth distends the pharyngeal recess and increases the auditory tube ostium depth(7).
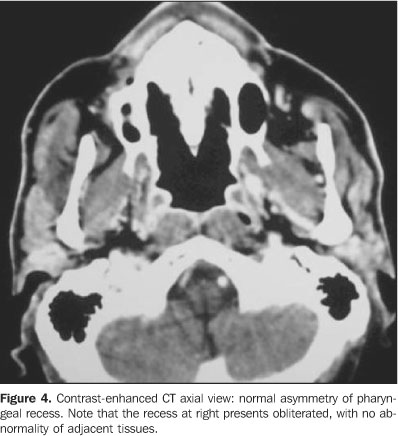
Sometimes, the nasopharyngeal lymphoid tissue may appear likea tumor process. Taking into consideration that its normal limitis the mucosa and sub-mucosa, the extension to deep planes shouldbe considered as an evidence of malignant lesion or an aggressiveinflammatory process(11,12). With the ageing process, there is a decrease in the volume oflymphoid tissues, levator and tensor palati, and constrictormuscles, and an increase of fat tissue. These changes are knownas nasopharyngeal atrophy. On the radiological evaluation, anincrease in size of the lateral pharyngeal recess is observed,with a larger prominence of the torus tubarius and auditory tubeostium. It is important to note that, if the asymmetry found on axial slices is not fully clarified, coronal slices become mandatory, especially in case of alterations in the upper end of the lateral recess(13) (Figure 4).
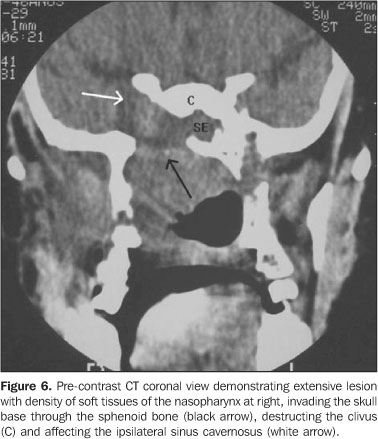
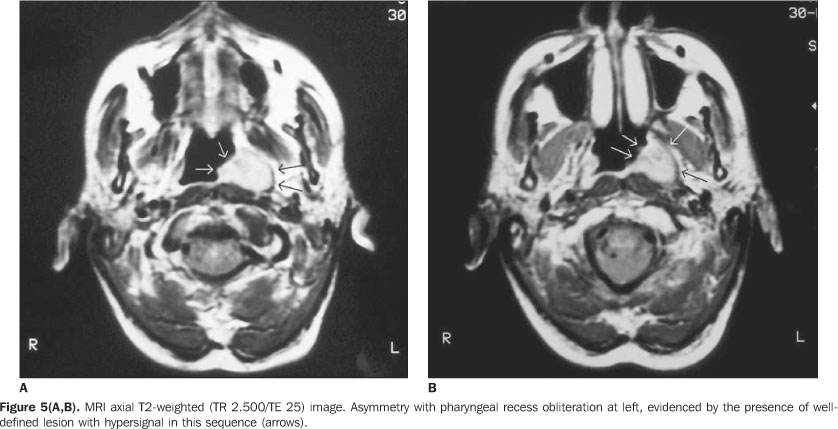
LOCAL STAGING OF NASOPHARYNGEAL CARCINOMAS Squamous cell carcinoma accounts for approximately 70% to 98%of all malignant nasopharyngeal neoplasms. Lymphomas account forabout 20% of cases, and the remaining 10% result from an array oflesions, including adenocarcinomas, cystic adenoid carcinomas,rhabdomyosarcomas, etc. Nasopharyngeal squamous cell carcinoma isa relatively rare type of cancer, accounting for 0.25% ofmalignant neoplasms in the North America, however presents a highincidence among Asians, particularly in the Southeast Asia,accounting for up to 18% of all malignancies inChina(2). It tends to affect younger age groupsthan other lesions of the upper respiratory-digestive tract, withhigher prevalence in men than inwomen(14). Risk factors for development of nasopharyngeal carcinomainclude those for oropharinx carcinoma, like nitrosamine (presentin food seasonings) and polycyclic hydrocarbons consumption,chronic tobacco and alcohol consumption, precarious conditions oflife, repeated sinonasal infections. Additionally, there is astrong association with Epstein-Barr virus, particularly inSoutheast Asia, where the affected population usually is youngerwhen compared with the Caucasianpopulation(2). The World Health Organization has updated the histologicalclassification of nasopharyngeal carcinomas, dividing them intotwo large subtypes: 1 – squamous cell carcinoma, and 2 –non-keratinized carcinoma. The non-keratinized carcinoma subtype is still subdividedinto: subtype I – differentiated (2a) and II – undifferentiated(2b). The term lymphoepithelioma also is utilized to designatethese two subtypes of tumors. These new nomenclatures 2a and 2bcorrespond, respectively, to 2 and 3 types in the formerclassification(2). The latest one,undifferentiated subtype of non-keratinized, seems to be moreclosely related to the presence of Epstein-Barr virus, resultingin the development of cancer in younger patients, by a stillunknown mechanism(15–17). Yet, the presence ofthe viral genome (Epstein-Barr virus) in metastatic lymph nodesmight suggest a nasopharyngeal carcinoma as primarysite(18). The site of origin varies. Most common sites are the lateral nasopharyngeal walls, most frequently the lateral pharyngeal recess. Frequently the torus tubarius is involved(14,19,20) (Figures 5A and 5B). The nasopharyngeal carcinoma clinical manifestation depends onthe size, localization and tumor dissemination route. Usually,small lesions are asymptomatic, but serous otitis media,headache, nasal obstruction, epistaxis, "throat ache", trismus,and proptosis may be present, depending on the degree ofinvolvement of neighbor structures and the size of thelesion(2). Other less frequent symptoms may bepresent: hemotympanum, periauricular mass, plugged ear sensation,barotrauma, polyp inside the inner ear, and sudden,neurosensorial hearing loss(21). Specific anatomical routes through which the tumordisseminates to the skull base or intracranial regions, as wellas the lymph node or distant metastatic dissemination are foundon CT and MRI images. Nasopharyngeal carcinoma is one of few head and neck tumorswhich do not present any relationship between the tumor size andthe presence of lymph node metastasis, and this is due to thewide drainage plexus present in the region. About 90% of casespresent with lymph node metastasis at the moment of diagnosis,and 50% of them already present bilateraldisease(17). The primary drainage site is to retropharyngeal lymph nodes,but, since in the adulthood these lymph nodes may presentobliteration by inflammatory/infectious processes occurred in thechildhood, they may not be involved. Other preferential drainagesites are the II, III, and, occasionally, Vlevels(2). Distant metastasis may affect the lungs, sketeleton, liver,and, occasionally, the choroid plexus(17). Usually, nasopharyngeal carcinomas disseminate through themucosa and sub-mucosa alongside muscular clusters, and in theirorigins and insertions, adjacent to fat planes surrounding themuscles, along the vascular/nervous bundles, and through theforamens created for the normal passage of these structures. Somestructures, like the auditory tube cartilaginous portion andpharyngobasilar fascia, demonstrate higher resistance against thetumor invasion(2, 19,22,23). The perineural dissemination is the most insidious form oftumor dissemination, and its presence is extremely important forthe prognosis and therapeutical planning. The nerve of thepterygoid canal represents the main nasopharyngeal carcinomaperineural dissemination route. Perineural dissemination shouldbe suspected in case of abnormal enlargement or enhancement ofthe nerve with obliteration of fatplanes(24). The nasopharyngeal carcinoma frequently originates in thelateral pharyngeal recess region. On CT images, asymmetry,blurring or obliterations are usually seen, and may be associatedwith an increase of the levatorpalati(6,19,25). When the tumor surpasses the pharyngobasilar fascia, itinvades the parapharyngeal space; according to Hoe, this occursin 65% of nasopharyngeal carcinomas(14,25).Sham and Choy have found 85% involvement of thisregion(26). From the parapharyngeal space, thetumor may extend superiorly, anteriorly, laterally orposteriorly. The superior extension of the nasopharyngeal carcinoma is the most frequent route of direct dissemination (48%)(19,25). Intracranial extension may occur by direct destruction of the skull base or by extension towards the sinus cavernosum via the foramen lacerum or foramen ovale. The superior extension of the tumor is visualized as an infiltration of sphenoid sinus with opacification or presence of fluid and bone destruction. Most usually, areas of bone destruction in the skull base are the clivus, the foramen lacerum and the middle cranial fossa, around the sphenoid sinus floor and foramen jugularis (Figure 6).
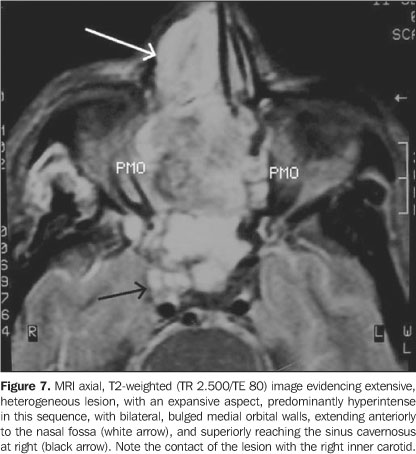
The tumor dissemination via foramen lacerum occurs perivascularly, through the carotid artery, resulting in erosion of the carotid canal (Figure 7). The dissemination via foramen ovale is perineural, resulting in erosion of the sphenoid base. A less common dissemination route towards the middle cranial fossa is the perineural route, via foramen rotundum(14,27). It is important to note that the invasion of the skull base occurs irrespective of the size of the tumor, ranging from subtle erosion to extensive bone destruction. Other concomitant findings in cranial invasion include predominant involvement of base cisterns, of sinus cavernosum, associated with palsy of the affected cranial pairs(2,17).
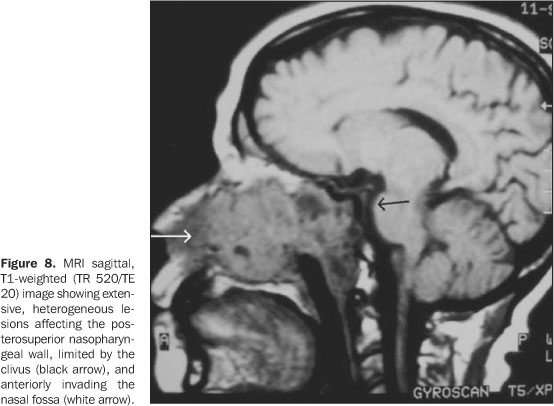
Low et al. have reported the involvement of thecerebellopontine angles by these carcinomas, highlighting boththe diagnostic and therapeutic difficulties of this disease,since the evaluated patients presented with advanced disease or apreviously treated tumor recurrence(28). Disease recurrence should be suspected if the patient presentsapparently inexplicable neurological symptoms like neurosensorialhearing loss, sonitus or facial palsy(28). The posterior extension is the second most frequent direct dissemination route (40%)(14). A mass anterior to the prevertebral muscles is observed in cases where a tumor extends towards the retropharyngeal space. In this localization, there are retropharyngeal lymph nodes e it may be difficult to differentiate lymph node involvement from direct extension by the tumor. The prevertebral space infiltration is identified as a mass posterior to prevertebral muscles, and occurs in 14% of cases (Figure 8).
In cases with anterolateral extension, an invasion of themasticator space, including the infratemporal fossa, may occur(14%). Inferiorly, carcinomas invade the oropharynx through thelateral walls of the pharynx, anterior and posterior tonsillarpillars. Since this type of dissemination is usually submucosal,it may be clinically occult. In such cases, CT and MRI might beuseful for detecting this type of dissemination or identifyingsuspect areas, indicating the biopsy of the region. As already mentioned, these tumors may be small andinfiltrative, causing, or not, a mass effect; in these cases, fatplanes obliteration and loss of definition of muscular marginsconstitute extremely useful diagnostic findings, andcontrast-enhanced (gadolinium) MRI with fat suppression has shownto be superior to CT in soft tissues evaluation, both in deep andsuperficial nasopharyngeal regions, besides being able to clearlydifferentiate lymphoid tissue frommusculature(17,19). This is a very importantaspect, since the most relevant prognostic factor innasopharyngeal carcinoma is the depth and degree of infiltrationinto neighboring structures, and not the tumorsize(29). On the other hand, CT is superior toMRI in demonstrating subtle involvement of bone structures in theskull base(6,30). Both methods play an essential and complementary role in thestaging and treatment of patients with nasopharyngeal cancers.PET - positron emission tomographic scanning, however, is a moreappropriate method to assess recurrent tumors and very smalllymph node metastasis(2,17). Considering that imaging methods do not allow the definition of the histological type of the lesion — a significant aspect, since the prognosis is different for the distinct cellular types —, the only alternative, for the radiologist is precisely mapping the invaded sites, helping the clinician/surgeon in the correct staging of the lesion (Table 1) (Figure 9).
Typically, squamous cell carcinomas present an attenuation coefficient similar to that of muscles, and do not show significant enhancement after intravenous contrast agent administration at CT. At MRI, these tumors present a signal of intermediary intensity in all the sequences. Tumor/tissue interfaces are better demonstrated by MRI, while a subtle bone destruction is better demonstrated by CT. Neoplastic extension through the foramens lacerum and ovale is better evaluated by MRI. The utilization of intravenous paramagnetic contrast agents (gadolinium) is advantageous in MRI studies, since the intense tumor enhancement allows a better lesion definition, avoiding extent underestimation, a frequent phenomenon in non-contrast enhanced margins as a function of the presence of edema and perilesional inflammatory process(31,32) (Figures 10A and 10B). For a complete staging, it is also necessary to study the lymph node involvement present in approximately 90% of patients at the moment of the diagnosis. Retropharyngeal lymph nodes usually are firstly affected, but may present normal features, in case of obliteration by previous inflammatory processes. The following are those of levels II and III, and, occasionally, those in levels I and V may be involved(2) (Table 2).
Generally, the therapy of choice for nasopharyngeal carcinomasis radiotherapy. For this reason, imaging methods are sosignificant for the tumor mapping with the purpose ofradiotherapy planning(33). However, the post-therapy evaluation, both by CT and MRI,presents a low sensitivity — about 45% to 67% for CT, and56% for MRI —, and low specificity — about 64% to 70%for CT, and 78 to 83% for MRI(34).
REFERENCES 1. Parker GD, Harnsberger HR, Jacobs JM. The pharyngeal mucosal space. Semin Ultrasound CT MR 1990;11:460–475. [ ] 2. Mukerji SK. Pharynx. In: Som PM, Curtin HD, editors. Head and neck imaging. 4th ed. St. Louis: Mosby, 2003;1470–1484. [ ] 3. Silver AJ, Mawad ME, Hilal SK, Sane P, Ganti SR. Computed tomography of the nasopharynx and related spaces. Part II: Pathology. Radiology 1983;147:733–738. [ ] 4. Last RJ. Anatomy regional and applied. 6th ed. London: Churchill Livingstone, 1978. [ ] 5. Testut L, Latarjet A. Aparato de la digestión. In: Testut L, Latarjet A. Tratado de anatomía humana 8ª ed. Barcelona-Buenos Aires: Salvat Editores, 1944;112–133. [ ] 6. Braun IF. MRI of the nasopharynx. Radiol Clin North Am 1989;27:315–330. [ ] 7. Mancuso AA, Bohman L, Hanafee W, Maxwell D. Computed tomography of the nasopharynx: normal and variants of normal. Radiology 1980; 137(1 Pt 1):113–121. [ ] 8. Khoo FY, Kanagasuntheram R, Chia KB. Variations of the lateral recesses of the nasopharynx. Arch Otolaryngol 1967;86:456–462. [ ] 9. Cormack DH. Ham's Histology. 9th ed. Philadelphia: JB Lippincott, 1987. [ ] 10. Harnsberger HR. Handbooks in radiology: head and neck imaging. Chicago: Mosby-Year Book, 1990. [ ] 11. Muraki AS, Mancuso AA, Harnsberger HR, Johnson LP, Meads GB. CT of the oropharynx, tongue base, and floor of the mouth: normal anatomy and range of variations, and applications in staging carcinoma. Radiology 1983;148:725–731. [ ] 12. Olsen WL, Jeffrey RB Jr, Sooy CD, Lynch MA, Dillon WP. Lesions of the head and neck in patients with AIDS: CT and MR findings. AJR Am J Roentgenol 1988;151:785–790. [ ] 13. Lingermar RE, Shellhamer RH. Benign neoplasms of the nasopharynx. In: Cummings CW, Fredrickson JM, Harker LA, et al, editors. Otolaryngology – head and neck surgery. St. Louis: Mosby, 1986;1269. [ ] 14. Fu KK. Treatment of tumor of nasopharynx. In: Thauley SE, Ponje WR, Batsakis JG, Lindeberg RD, editors. Comprehensive management of head and neck tumors. Philadelphia: WB Saunders, 1987;30:649–683. [ ] 15. Nicholls JM, Agathanggelou A, Fung K, Zeng X, Niedobitek G. The association of squamous cell carcinomas of the nasopharynx with Epstein-Barr virus shows geographical variation reminiscent of Burkitt's lymphoma. J Pathol 1997;183:164–168. [ ] 16. Zhang XS, Wang HH, Hu LF, et al. V-val subtype of Epstein-Barr virus nuclear antigen 1 preferentially exists in biopsies of nasopharyngeal carcinoma. Cancer Lett 2004;211:11–18. [ ] 17. Weber AL, al-Arayedh S, Rashid A. Nasopharynx: clinical, pathologic, and radiologic assessment. Neuroimaging Clin N Am 2003;13:465–483. [ ] 18. Macdonald MR, Freeman JL, Hui MF, et al. Role of Epstein-Barr virus in fine-needle aspirates of metastatic neck nodes in the diagnosis of nasopharyngeal carcinoma. Head Neck 1995;17: 487–493. [ ] 19. Hoe JWM. Computed tomography of nasopharyngeal carcinoma. A review of CT appearances in 56 patients. Eur J Radiol 1989;9:83–90. [ ] 20. Su CY, Hsu SP, Lui CC. Computed tomography, magnetic resonance imaging and electromyographic studies of tensor veli palatini muscles in patients with nasopharyngeal carcinoma. Laryngoscope 1993;103:673–678. [ ] 21. Low WK, Goh YH. Uncommon otological manifestations of nasopharyngeal carcinoma. J Laryngol Otol 1999;113:558–560. [ ] 22. Miura T, Hirabuki N, Nishiyama K, et al. Computed tomographic findings of nasopharyngeal carcinoma with skull base and intracranial involvement. Cancer 1990;65:29–37. [ ] 23. Hoover LA, Hanafee WN. Differential diagnosis of nasopharyngeal tumors by computed tomography scanning. Arch Otolaryngol 1983;109:43–47. [ ] 24. Pandolfo I, Bandino A, Longo M, Faranda C. Perineural spread of nasopharyngeal carcinoma: radiological and CT demonstration. Eur J Radiol 1988;8:231–235. [ ] 25. Hoe J. CT of nasopharyngeal carcinoma: significance of widening of the preoccipital soft tissue on axial scans. AJR Am J Roentgenol 1989;153: 867–872. [ ] 26. Sham JST, Choy D. Prognostic value of paranasopharyngeal extension of nasopharyngeal carcinoma on local control and short-term survival. Head Neck 1991;13:298–310. [ ] 27. Teresi LM, Lufkin RB, Vinuela F, et al. MR imaging of the nasopharynx and floor of the middle cranial fossa. Part II. Malignant tumors. Radiology 1987;164:817–821. [ ] 28. Low WK, Fong KW, Chong VF. Cerebellopontine angle involvement by nasopharyngeal carcinoma. Am J Otol 2000;21:871–876. [ ] 29. Sakata K, Hareyama M, Tamakawa M, et al. Prognostic factors of nasopharynx tumors investigated by MR imaging and the value of MR imaging in the newly published TNM staging. Int J Radiat Oncol Biol Phys 1999;43:273–278. [ ] 30. Dillion WP, Mills CM, Kjos B, DeGroot J, Brant-Zawadzki M. Magnetic resonance imaging of the nasopharynx. Radiology 1984;152:731–738. [ ] 31. Souza RP, Rapoport A. O valor da tomografia computadorizada e da ressonância magnética na avaliação do espaço parafaríngeo. Parte II: tumores e pseudotumores. Rev Imagem 1994;16:7–24. [ ] 32. Phillips CD, Gay SB, Newton RL, Levine PA. Gadolinium-enhanced MRI of tumors of the head and neck. Head Neck 1990;12:308–315. [ ] 33. Chong VF, Fan YF, Mukherji SK. Carcinoma of the nasopharynx. Semin Ultrasound CT MR 1998;19:449–462. [ ] 34. Chong VF, Fan YF. Detection of recurrent nasopharyngeal carcinoma: MR imaging versus CT. Radiology 1997;202:463–470. [ ]
Received October 28, 2004.
* Study developed at Service of Diagnostic Imaging – Hospital Heliópolis Department of Radiology, São Paulo, SP, Brazil. |
|

{kind=link}
{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554