Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 1 - Jan. /Feb. of 2007
Vol. 40 nº 1 - Jan. /Feb. of 2007
|
ORIGINAL ARTICLE
|
|
Analysis of the new classification of bone densitometry reports |
|
|
Autho(rs): Osvaldo Sampaio Netto, Larissa de Oliveira Lima Coutinho, Danielle Cristina de Souza |
|
|
Keywords: Densitometry, Osteoporosis, Spine, Bone density |
|
|
Abstract:
IMD, Nuclear Medicine Specialist, Qualifying in Bone Densitometry, Professor for the Course of Medicine at Universidade Católica de Brasília
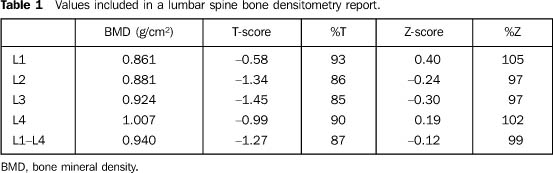
INTRODUCTION Osteoporosis is a condition characterized by low bone mass,capable of resulting in development of bone fractures in theabsence of trauma or caused by a low-impacttrauma(1). Since 1994, dual energy x-ray bone densitometry has beenconsidered by the World Health Organization (WHO) as agolden-standard for diagnosing osteoporosis(2)and so the number of bone densitometry studies has increasedconsiderably. An American survey published in 1992 estimated 1.5 millionosteoporotic fractures per year(3), and if thisprevalence of osteoporotic fractures remains the same until 2025,about a quarter of the whole female population should presentosteoporotic fracture(4). In the interpretation of bone densitometry studies (Table 1), the result may be expressed in bone mineral density value, standard deviation in relation to young adults (T-score), bone mineral density percentage for young adult (%T), standard deviation in relation to people in the same age range (Z-score), mineral bone density percentage for people in the same age range (%Z).
In 1994, WHO defined the criteria currently utilized worldwidein bone densitometry reports, based on standard deviation inrelation to young adult, as follows: a) normal: standard deviation up to –1.00; b) osteopenia: standard deviation ranging between –1,00 and–2.50; c) osteoporosis: standard deviation = –2.50. In an official publication of 2005, the International Societyfor Clinical Densitometry (ISCD) recommends the utilization ofthe T-score and WHO standards only for post-menopausal women andmen with = 50 years of age. In premenopausal women and men withless than 50 years of age, the Z-score utilization is recommendedas follows(5): a) "below the expected range for age": Z-score = –2.00; b) "within the expected range for age": Z-score >–2.00. The present study has been developed considering this new classification for bone densitometry reports, and is aimed at comparing the new normatization of lumbar spine bone densitometry reports proposed by ISCD in 2005, with the WHO classification routinely utilized since 1994.
MATERIALS AND METHODS Two hundred spine bone densitometry studies have been analyzed; 136 of them had been performed in a Lunar® DPX-IQ equipment at Universidade Católica de Brasília, and 64 in a Hologic® QDR4500 equipment of Hospital das Forças Armadas. Inclusion criteria were: female gender, 20 years as theminimum age, and 49 as the maximum, and absence of lumbar spinemorphological changes visualized on densitometric studies. Theexclusion criteria were: women more than 50 years or menopausalwomen. The software MSExcelâ was employed for results analysis.
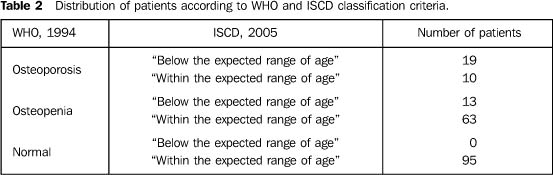
RESULTS Mean age in the 200 densitometric studies analyzed was 32.42± 9.53 years (age range = 20–49 years). Results obtained from the analysis according to the WHOclassification were the following: 29 patients with osteoporosisof the lumbar spine (T-score < –2.50), 76 with osteopenia(T-score < –1.00 and > –2.50), and 95 within normalitylevels (T-score > –1.00). Mean ages were, respectively, 43.3,31.1 and 30.2 years. Once the new ISCD 2005 classification was applied, the resultswere the following: only 32 patients were "below the expectedrange for age" (Z-score < –2.00), and 162 "within theexpected range for age" (Z-score > –2.00). Applying the new classification to the 29 osteoporotic patients (Table 2), 19 of them were "below the expected range for age", and 10 were "within the expected range for age".
In the present study, following the WHO criteria, we had 76 patients with osteopenia (Table 2), 13 of them "below the expected range for age", and 63 "within the expected range for age". All the patients rated as "normal" according the WHO criteria (Table 2) remained in the group "within the expected range for age" in the ISCD classification, as it could be expected.
DISCUSSION In 1994, the WHO normatization played a significant role inthe unification of bone densitometry reports, since, at thattime, the densitometry technique was in its very beginning, andthe studies interpretation was based on different criteria. Withsuch unification, this diagnostic method was diffused, allowing agreat progress in the knowledge of osteoporosis. In the last 12years, the terms osteoporosis and osteopenia became commonknowledge among physicians and patients. The arrival of this newclassification is significant for representing a progress in theinterpretation of this analysis methodology. The terms Z-score and T-score must be understood byphysicians, allowing the correct interpretation of densitometricstudies, and for them to be able to explain their meaning for thepatients. In the last 12 years, T-score was the classificationstandard for bone densitometry reports. Based on this newclassification, the Z-score starts being utilized in patients upto 49 years of age, and the use of the T-score (OMS, 1994)remains restricted to patients aged 50 years or older. The factof following two different classification criteria according tothe patient's age, might complicate the study interpretation,both for the physician and the patient. An issue to be highlighted and addressed on a case-by-casebasis, is the fact of patients aged up to 49 years who hadpreviously undergone bone densitometry studies, and, according tothe WHO criteria, had been considered as osteoporotic, and, on anew study interpreted according to the new criteria, might berated as normal ("within the expected range for age"). In oursurvey, we have found this condition in 34.5% of osteoporoticpatients. It is important to note that ten patients rated asosteoporotic, and probably followed-up and oriented towardsstopping or reverting the disease progression, started beingrated "within the expected range for age", and, consequently,included in the normality group, in spite of the decrease intheir bone mineral density according to the WHO criteria of1994. The fact of using this new classification "within the expectedrange for age", leads to an unconcern about these patients whohad previously been considered with low rates of bone mineraldensity an increased risk of fracture. Notwithstanding, ISCD doesnot present a proposal of conduct and treatment for eachclassification. So, this new classification should be comprehensively known and understood by physicians who request or perform bone densitometry studies, aiming at the correct interpretation, explanation and orientation to the patients.
REFERENCES 1. Kanis JA. Bone density measurements and osteoporosis. J Intern Med 1997;241:173–175. [ ] 2. World Health Organization. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. WHO Technical Report Series, 843. Génève: WHO, 1994. [ ] 3. Gabriel SE, Tosteson AN, Leibson CL, et al. Direct medical costs attributable to osteoporotic fractures. Osteoporos Int 2002;13:323–330. [ ] 4. Cuddihy MT, Gabriel SE, Crowson CS, et al. Osteoporosis intervention following distal forearm fractures: a missed opportunity? Arch Intern Med 2002;162:421–426. [ ] 5. International Society for Clinical Densitometry. The ISCD's official positions (updated 2005). Washington: ISCD, 2005. [ ]
Received January 27, 2006.
* Study developed at Universidade Católica de Brasília, Brasília, DF, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554