Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 4 - July / Aug. of 2009
Vol. 42 nº 4 - July / Aug. of 2009
|
CASE REPORT
|
|
Erdheim-Chester disease: a two-case report |
|
|
Autho(rs): Fernando Fernandez Hexsel, Letícia Frigo Canazaro, Mariana Capoani, Paula Musa Aguiar, Eiji Suwa, Antonio Carlos Maciel |
|
|
Keywords: Erdheim-Chester disease, Radiography, Computed tomography |
|
|
Abstract:
IMDs, Radiologists, Unit of Radiology - Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, RS, Brazil
INTRODUCTION Erdheim-Chester disease is a rare form of non-Langerhans-cell histiocytosis, firstly described by Jakob Erdheim and William Chester in 1930(1). The etiology of this disease still remains unknown. Histologically, it is characterized by a diffuse infiltration by foamy histiocytes of the tissues involved, causing a local xanthomatous or xanthogranulomatous reaction(2). The disease affects multiple organ systems, commonly involving bones, central nervous system, eyes, lungs, mediastinum, kidneys and retroperitoneum, the prognosis depending on the extent of visceral involvement(3,4). The authors present two cases with typical clinical presentation and findings, discussing clinical, radiological and propedeutic aspects.
CASES REPORT Case 1 - A female, white, 43-year-old patient was admitted for investigation of an abdominal mass, anemia, leukocytosis, thrombocytosis and pain in the lower limbs. The initial chest radiography demonstrated an increase in heart volume and thickening of horizontal and oblique fissures of the right lung. Lower limbs radiography demonstrated symmetrical sclerosis predominating in the tibial diaphyses. Chest and abdominal computed tomography demonstrated thickening of interlobular septa in the pulmonary apices, lesions presenting soft tissues density adjacent to the descending thoracic aorta and an infiltrative lesion involving a significant extent of the abdominal aorta and internal iliac vessels, including the renal vessels and affecting both renal sinuses with a consequential, moderate hydronephrosis, continuing as an extensive, expansive mesenteric mass, with complete involvement of vessels in this region. During the hospital stay, the patient complained of decrease in visual acuity, and orbital computed tomography was performed and demonstrated bilateral tumescent lesions almost completely infiltrating the intraconal fat. Biopsy of the right retrobulbar tumescent lesion demonstrated xanthogranuloma. A subsequent immunohistochemical study demonstrated positive results for CD68 (PG-M1) and CD1a (MTB1 negative), compatible with the diagnosis of Erdheim-Chester disease. Corticosteroid therapy was introduced and the patients is currently undergoing outpatient follow-up. Case 2 - A female, white, 37-year-old patient attended the hospital complaining of polyuria, polydipsia, and pain in the lower limbs. Upper and lower limbs radiographies demonstrated medullary osteosclerosis and areas of symmetrical cortical hyperostosis. Later during the hospital stay, the patient presented exophthalmos and decrease in visual acuity. Orbital computed tomography was bilaterally performed, and identified masses obliterating the intraconal fat planes involving the optic nerves with anterior displacement of both ocular globes. Biopsy of the conjunctival mass demonstrated accumulation of foamy histiocytes and lymphocytic infiltrate whose immunohistochemical study resulted negative for S-100 protein. Chest computed tomography demonstrated aortic dissection with thrombosis and ulceration, bilateral pleural effusion or thickening, calcified lymphatic ganglia in the pulmonary hilum, subdiaphragmatic calcification and/or calcification in the right hepatic lobe, and a significant enlargement of both adrenal glands. The patient underwent corticosteroid therapy and radiotherapy of the orbital lesions followed by chemotherapy. Currently, she is under outpatient follow-up.
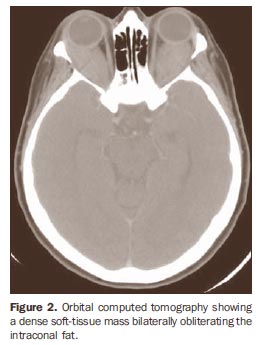
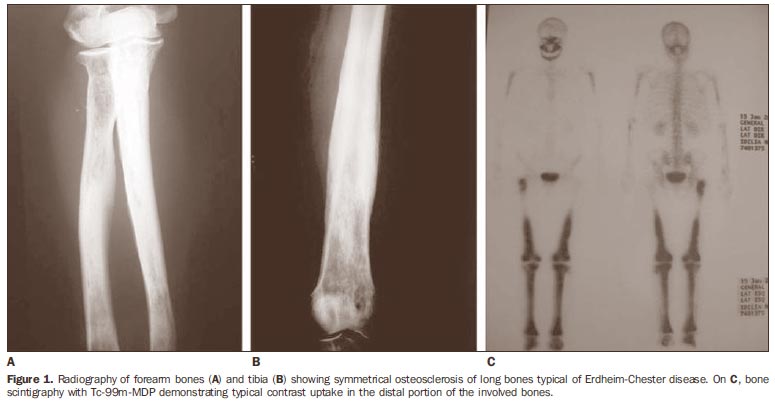
DISCUSSION Most commonly, Erdheim-Chester disease occurs after the fourth decade of life, with a subtle male prevalence. The disease pathogenesis is still to be elucidated, but it seems there be tropism of histiocytes to connective, fat and perivascular tissues, with an infiltrative pattern and local fibrosis(5). Bone pain associated with progressive weakness, particularly in the lower limbs, is the most frequent symptom of Erdheim-Chester disease. Also, the patient frequently presents fever, weight loss, exophthalmos, dyspnea and signs of neurological involvement, such as diabetes insipidus(4,6). The diagnosis is based on radiological and pathological findings. Bone involvement present in both cases presently reported consists of symmetric sclerosis of long tubular bones, predominating in metaphysis and diaphysis of lower limbs. This is the radiological abnormality most frequently reported in the literature (60% of cases)(4-8) (Figure 1). As for pulmonary findings, both radiography and computed tomography demonstrate fissural thickening and interlobular septa thickening, besides pleural effusion, centrolobular nodules, interstitial reticular opacities, and at computed tomography multifocal areas of ground-glass attenuation(4,8). Erdheim-Chester disease presents a tropism of histiocytes to connective, fat and perivascular tissues. This involvement may extend to the whole aorta, with invasion of the retroperitoneum and mediastinum, leading to severe complications such as cardiac failure, tamponade and renal failure. Hepatic, pancreatic and mesenteric involvement is extremely rare(5). The ocular involvement observed in both case 1 and 2 may be uni- or bilateral and is seen at images as intraorbital masses or retrobulbar tumors (Figure 2).
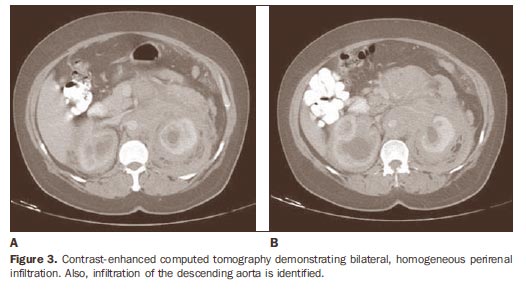
At computed tomography, retroperitoneal involvement is visualized as soft tissues masses, for example in the psoas muscle, with fat stranding, which would explain the clinical signs of renal failure and arterial hypertension resulting from the development of hydronephrosis(3,4). Renal/perirenal involvement is observed in 29% of patients in a 59-case series where computed tomography demonstrated hypoattenuated homogeneous perirenal tissue infiltration with poor contrast uptake(4). The "hairy" or "onion peel" kidney appearance observed in these two patients is due to the symmetrical and bilateral infiltration of both the posterior pararenal and perirenal spaces highly suggestive of the diagnosis. The extension to the renal sinuses may lead to urinary tract obstruction (Figure 3).
A consensus on the management of Erdheim-Chester disease is still to be reached, but data in the literature report promising results with the utilization of corticosteroids, immunosuppressive drugs such as cyclophosphamide, chemotherapy and radiotherapy. The prognosis will depend on the extent of visceral involvement at the moment of the diagnosis(3,4).
REFERENCES 1. Wright R, Hermann R, Parisi J. Neurological manifestations of Erdheim-Chester disease. J Neurol Neurosurg Psychiatry. 1999;66:72-5. [ ] 2. Haroche J, Amoura Z, Dion E, et al. Cardiovascular involvement, an overlooked feature of Erdheim-Chester disease: report of 6 new cases and a literature review. Medicine (Baltimore). 2004;83:371-92. [ ] 3. Haroche J, Amoura Z, Wechsler B, et al. Erdheim- Chester disease. Presse Med. 2007;36(Pt 11): 1663-8. [ ] 4. Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D, et al. Erdheim-Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine (Baltimore). 1996;75:157-69. [ ] 5. Dion E, Graef C, Haroche J, et al. Imaging of thoracoabdominal involvement in Erdheim-Chester disease. AJR Am J Roentgenol. 2004; 183:1253-60. [ ] 6. Boissel N, Wechsler B, Leblond V. Treatment of refractory Erdheim-Chester disease with double autologous hematopoietic stem-cell transplantation. Ann Intern Med. 2001;135:844-5. [ ] 7. Gil Marculeta R, Domínguez Echávarri PD, Cano Rafart D, et al. Radiologic diagnosis of Erdheim- Chester disease. A case report. Radiologia. 2006; 48:317-20. [ ] 8. Wittenberg KH, Swensen SJ, Myers JL. Pulmonary involvement with Erdheim-Chester disease: radiographic and CT findings. AJR Am J Roentgenol. 2000;174:1327-31. [ ] Received October 19, 2007. * Study developed at the Unit of Radiology - Santa Casa de Misericórdia de Porto Alegre, Porto Alegre, RS, Brazil. |
|

{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554