Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 4 - July / Aug. of 2009
Vol. 42 nº 4 - July / Aug. of 2009
|
WHICH IS YOUR DIAGNOSIS?
|
|
Qual o seu diagnóstico? |
|
|
Autho(rs): Pedro José de Santana Júnior, Kim-Ir-Sen Santos Teixeira, Pedro Paulo Teixeira e Silva Torres, Renato Tavares Daher, Patrícia Karla Vilarinho Santana, Ana Caroline Vieira Aurione |
|
|
IMD, Resident, Department of Radiology and Diagnostic Imaging — Hospital das Clínicas da Universidade Federal de Goiás (UFG), Goiânia, GO, Brazil
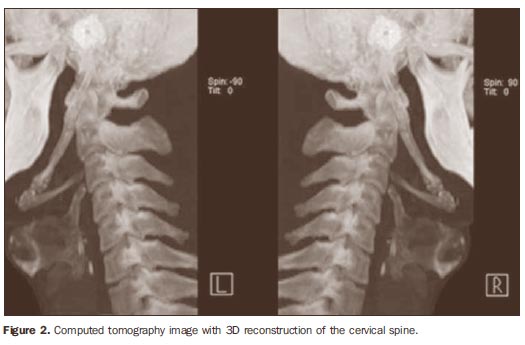
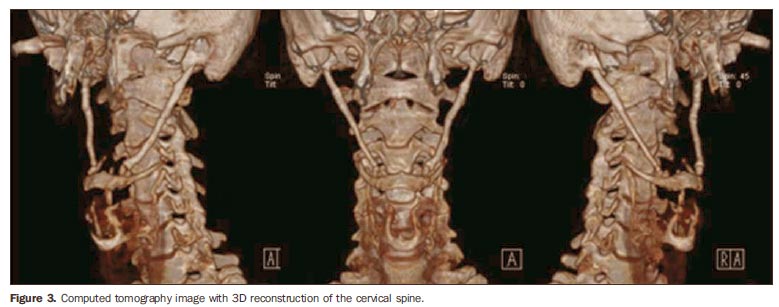
A male, 41-year-old patient, agricultural worker, complaining of pain in the right shoulder and in the whole cervical region besides facial pain in the region of the temporomandibular joint. At clinical examination, a hardened bulging mass was felt at palpation of the right anterior pillar of the tonsillar fossa in association with limited mouth opening. The patient underwent radiography and multidetector computed tomography of the skull base. Images description Figures 1, 2 and 3. Bilateral stylohyoid ligament calcification.
Diagnosis: Eagle syndrome.
COMMENTS Eagle syndrome corresponds to a set of symptoms including recurrent facial and cervical pain (with or without irradiating to the ear or mastoid region), dysphagia, sensation of a foreign body in the throat, sialorrhea, glossalgia, dysphonia, recurrent headache, carotidynia, vertigo, visual perturbation and restricted neck motion. This disease was first described in 1937 by the otolaryngologist Watt W. Eagle, and is directly associated with the styloid process elongation or stylohyoid ligament calcification. Incidence is higher in women, at the fourth decade of life, with no preference for unilateral or bilateral presentation(1). The temporal bone styloid process corresponds to an osseous projection measuring approximately 25 mm in length, located posteriorly to the pharynx, between the internal and external carotid arteries. The set formed by the styloid process, stylohyoid ligament and the small horn of the hyoid bone corresponds to the stylohyoid complex or apparatus whose embryological origin is the Reichert's cartilage of the second brachial arch(2). The etiology of the styloid apophysis elongation (> 30 mm) still remains unknown. There are several theories explain the etiopathology of the disease such as idiopathic, congenital alteration resulting from the persistence of one of the precursory cartilages, or ossification of the styloid ligament(3). Most patients with elongated styloid process are asymptomatic, and the diagnosis can only be achieved through imaging studies. The incidence of this abnormality in the general population ranges between 4% and 28%, and only 4% to 10.3% of the patients in this group are symptomatic(2). Differential diagnoses for Eagle syndrome include: cervical arthritis, temporomandibular joint disorders, otitis, mastoiditis, sialadenitis, sialolithiasis, esophageal diverticulosis, temporal arteritis, myofascial pain, chronic pharyngotonsillitis, unerupted or impacted third molar, hemicrania, histamine headache, pharynx tumor, tumor in the base of the tongue, trigeminal neuralgia, glossopharyngeal, upper laryngeal and sphenopalatine tumors(1). Elongated styloid apophysis is suspected through clinical examination with palpation of the tonsillar fossa, and evidenced by imaging methods on facial, lateral, anteroposterior and oblique views. Computed tomography is the method of choice for this evaluation. Considering the variable degree of calcification and variability in the stylohyoid complex presentations, some authors have developed a radiographic classification system describing the stylohyoid complex as elongated, pseudoarticulated or segmented, the second one corresponding to the computed tomography images shown in the present case. Computed tomography plays a critical role in the diagnosis of Eagle syndrome for allowing images acquisition in the axial, sagittal and coronal planes, as well as multiplanar and 3D reconstructions. Thus, this method demonstrates not only bone structures and calcified components - likewise radiographic studies -, but also their relationship with the other adjacent structures, overcoming the conventional radiology limitations(3). Although the surgical therapy (styloid apophysis resection) is more effective, in the present case a conservative management was adopted, utilizing anti-inflammatory drugs, with a good outcome till the present moment(4,5). The presentation of a case like this is important because of the scarcity of similar reports in the radiological literature, in spite of the dental and otolaryngological literature. Considering that Eagle syndrome is included in the spectrum of differential diagnoses of several cervicofacial diseases, the knowledge about this entity is critical for a correct diagnosis and consequent therapeutic approach(5).
REFERENCES 1. Savranlar A, Uzun L, Uður MB, et al. Three-dimensional CT of Eagle's syndrome. Diagn Interv Radiol. 2005;11:206-9. [ ] 2. Chiang KH, Chang PY, Chou ASB, et al. Eagle's syndrome with 3-D reconstructed CT: two cases report. Chin J Radiol. 2004;29:353-7. [ ] 3. Sá ACD, Zardo M, Paes Junior AJO, et al. Alongamento do processo estilóide (síndrome de Eagle): relato de dois casos. Radiol Bras. 2004; 37:385-7. [ ] 4. Tiago RSL, Marques Filho MF, Maia CAS, et al. Síndrome de Eagle: avaliação do tratamento cirúrgico. Rev Bras Otorrinolaringol. 2002;68:196-201. [ ] 5. Murtagh RD, Caracciolo JT, Fernandez G. CT findings associated with Eagle syndrome. AJNR Am J Neuroradiol. 2001;22:1401-2. [ ] Study developed at Departamento de Radiologia e Diagnóstico por Imagem do Hospital das Clínicas da Universidade Federal de Goiás (UFG), Goiânia, GO, Brazil. |
|


{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554