Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 3 - May / June of 2009
Vol. 42 nº 3 - May / June of 2009
|
CASE REPORT
|
|
Prenatal sonographic diagnosis of fetal cardiac rhabdomyoma: a case report |
|
|
Autho(rs): Hélio Antonio Guimarães Filho, Edward Araujo Junior, Cláudio Rodrigues Pires, Lavoisier Linhares Dias da Costa, Luciano Marcondes Machado Nardozza, Rosiane Mattar |
|
|
Keywords: Prenatal diagnosis, Ultrasonography, Fetal masses, Fetal tumors |
|
|
Abstract:
IPhD, Professor at Centro de Treinamento em Imaginologia (Cetrim), João Pessoa, PB, Brazil
INTRODUCTION Diagnostic imaging studies are frequently performed during the gestation to evaluate fetal diseases(1). Cardiac tumors constitute a rare condition, affecting 0.17-28/10,000 of the general population, according to necropsy studies(2). Recently, an increase has been observed in diagnoses of these tumors during the prenatal period, as result of the contribution of fetal echocardiography(3,4). Depending on the intracardiac localization of the tumor, the disease may progress with severe arrhythmias, congestive heart failure, hydrops, and not rarely, with fetal death(5). In the present study, the authors report a case of a fetus in the third gestational trimester presenting a bulky intracardiac mass diagnosed by means of prenatal echocardiography.
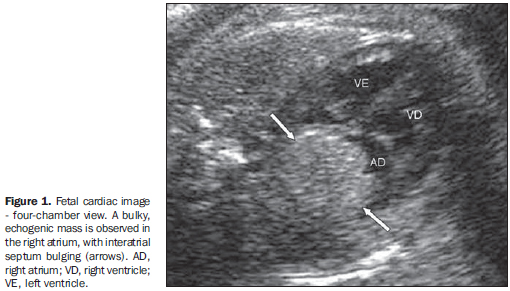
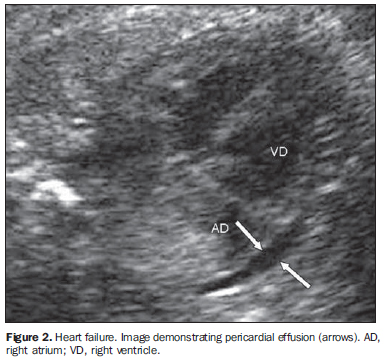
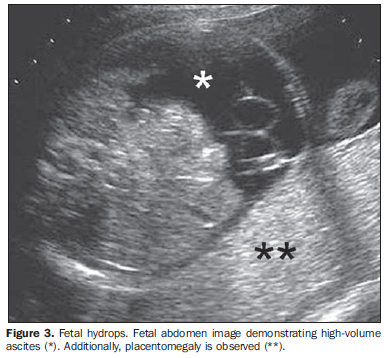
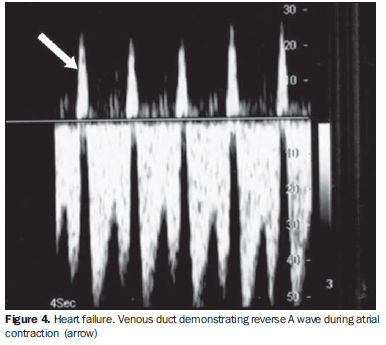
CASE REPORT A 23-year-old, secundigravida, nulliparous patient at her 31st gestational week was referred to the institution to be submitted to sonographic morphological study for cardiac malformation with arrhythmia diagnosed by routine sonographic study. Echographic findings demonstrated the presence of an intracardiac bulky mass in the right atrium, with the interatrial septum bulging. The mass presented a hyperechogenic, homogeneous aspect, and measured about 25 × 21 mm in its largest diameters (Figure 1). The fetus presented with persistent, marked tachyrrhythmia (on average, 263 beats/minute), with clear signs of congestive heart failure at 2D echography and ultrasoud Doppler, and hydrops (Figures 2, 3 and 4).
In spite of the established therapy, the fetus progressed to death in ten days. Necropsy confirmed the prenatal diagnostic suspicion of cardiac rhabdomyoma.
DISCUSSION Cardiac tumors, although constituting a rare condition, have presented an increased incidence of up to 0.2% in reference centers for pediatric cardiopathy(6). Varied hemodynamic repercussions may be observed. According to their localization, size and number, these tumors may lead to blood flow obstruction and alteration of the ventricular ejection fraction, causing arrhythmia, congestive heart failure, pericardial effusion, cardiomegaly, hydrops and fetal death(5,7). As regards histological types, cardiac rhabdomyomas or hamartomas represent the most frequently found histological lineage in the prenatal period(6,7). The frequent association of this entity with tuberous sclerosis, a disease with autosomal dominant transmission, emphasizes the relevance of the diagnostic screening both in the fetus and its parents. In fact, tuberous sclerosis is observed in more than 50% of the fetuses with primary cardiac tumors(7). In the present case, sonographic evaluation of the fetal central nervous system did not detect any suspicious intracranial involvement, and the parents are currently undergoing investigation for tuberous sclerosis. Fibromas, hemangiomas and teratomas are less frequently found in the fetal heart(8,9). Fibromas usually present as a single lesion, frequently involving the left ventricular wall or the interventricular septum(6). Teratomas originate in the pericardium and present as a single, heterogeneous, encapsulated and large sized mass, frequently reaching the base of the heart at right(8). On the other hand, cardiac hemangiomas are rare in the intrauterine life and in the childhood(7). Although cardiac myxomas are prevalent in the adult age group, only one study in the literature reports this histological type of tumor diagnosed in intrauterine life(10). Usually, at ultrasonography, cardiac rhabdomyomas are detected by the end of the second gestational trimester either as a single or multiple, well delimitated, solid, homogeneous, hyperrefringent mass with varied dimensions(2,6,7). Frequently, these lesions affect the left ventricle (60%) and, at a lower ratio, the right ventricle (26%)(6). Cardiac dysrhythmias are observed in 16% to 47% of cases(5). Therapy with digitalis and other antiarrhythmic drugs orally administered to mother or by fetal intravenous route (cordocentesis), and therapeutic preterm delivery should be considered in the presence of cardiac function involvement(6,7). Intrauterine surgical resection of these tumors has been suggested for management of immature fetuses with hydrops, but a consensus is still to be reached in relation to the indication of this therapeutic alternative(11). Most of times, however, cardiac rhabdomyomas are typically well tolerated, with risk for fetal death estimated in 4% to 6% of cases(7). There are studies in the literature reporting spontaneous tumor regression, particularly in the third gestational trimester(7). In a retrospective study, 19 cases of fetal cardiac tumors have been evaluated, with partial or complete regression of these masses in eight patients, and with 10 patients presenting later development of tuberous sclerosis(7). In fact, a perinatal benign course, with progressive regression and complete resolution of the tumor can be observed in more than 80% of cases in the childhood(6,7).
CONCLUSION The prenatal diagnosis of fetal cardiac tumors can be achieved by means of a detailed echographic study, with rare cases of false-positive diagnosis(12). The early detection of these tumors allows a specialized prenatal follow-up and, if indicated, the institution of appropriate therapeutics, thus contributing for reducing the perinatal morbimortality.
REFERENCES 2. McAllister HA Jr. Primary tumors of the heart and pericardium. Patol Annu. 1979;14 Pt 2:325-55. [ ] 3. Zhou QC, Fan P, Peng QH, et al. Prenatal echocardiographic differential diagnosis of fetal cardiac tumors. Ultrasound Obstet Gynecol. 2004;23: 165-71. [ ] 4. Araujo Júnior E, Zanforlin Filho SM, Pires CR, et al. Spatio-temporal image correlation (STIC): nova técnica para avaliação do coração fetal. Radiol Bras. 2006;39:373-7. [ ] 5. Kagan KO, Schmidt M, Kuhn U, et al. Ventricular outflow obstruction, valve aplasia, bradyarrhythmia, pulmonary hypoplasia and non-immune fetal hydrops because of a large rhabdomyoma in a case of unknown tuberous sclerosis: a prenatal diagnosed cardiac rhabdomyoma with multiple symptoms. BJOG. 2004;111:1478-80. [ ] 6. Holley DG, Martin GR, Brenner JI, et al. Diagnosis and management of fetal cardiac tumors: a multicenter experience and review of published reports. J Am Coll Cardiol. 1995;26:516-20. [ ] 7. Bader RS, Chitayat D, Kelly E, et al. Fetal rhabdomyoma: prenatal diagnosis, clinical outcome, and incidence of associated tuberous sclerosis complex. J Pediatr. 2003;143:620-4. [ ] 8. Riskin-Mashiah S, Moise KJ Jr, Wilkins I, et al. In utero diagnosis of intrapericardial teratoma: a case for in utero open fetal surgery. Prenat Diagn. 1998;18:1328-30. [ ] 9. Tongsong T, Sirichotiyakul S, Sittiwangkul R, et al. Prenatal sonographic diagnosis of cardiac hemangioma with postnatal spontaneous regression. Ultrasound Obstet Gynecol. 2004;24:207-8. [ ] 10. Paladini D, Tartaglione A, Vassallo M, et al. Prenatal ultrasonographic findings of a cardiac myxoma. Obstet Gynecol. 2003;102(5 Pt 2):1174-6. [ ] 11. Parry AJ, Carroll S, Lotto A, et al. Median sternotomy as an exit procedure in a child with massive pericardial tumor. J Pediatr Surg. 2004;39: 1408-10. [ ] 12. Tehrani M, Vettraino IM, Chang CH. Localized nodular hypertrophy mimicking rhabdomyoma in the fetal heart: prenatal sonographic and pathology findings. Pediatr Dev Pathol. 2004;7:192-7. [ ] Received May 8, 2007. * Study developed at Universidade Federal de São Paulo/Escola Paulista de Medicina (Unifesp/EPM) and Centro de Treinamento em Ultrassonografia de São Paulo (Cetrus), São Paulo, SP, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554