Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 3 - May / June of 2009
Vol. 42 nº 3 - May / June of 2009
|
ORIGINAL ARTICLE
|
|
Videofluoroscopy chair for the study of swallowing and related disorders |
|
|
Autho(rs): Milton Melciades Barbosa Costa, Lucia Viviana Canevaro, Hilton Augusto Koch, Ricardo DeBonis |
|
|
Keywords: Videofluoroscopy, Swallowing, Dysphagia, Neuromotor disorder, Adapted chair |
|
|
Abstract:
IPhD, Titular Professor, Head of the Laboratory of Digestive Motility and Imaging of Instituto de Ciências Biomédicas - Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
INTRODUCTION Because of the absence of a specifically designed device, the videofluoroscopic study of swallowing and related disorders is performed with seriography and angiography equipment and C-arms that are radiological devices originally designed for other types of studies. The availability of an additional output in the monitors of such equipments with preserved image quality (loop through) allows the fluoroscopy images to be recorded on magnetic media while the study is being performed. Although useful, these adapted radiological devices not always are practical and/or effective to meet the requirements related to positioning and freedom of movements for an appropriate study of the swallowing phases both in healthy and dysphagic individuals. Such difficulties are many times aggravated by the frequent association of dysphagia with motor/postural impairment of neurological origin(1-4). Studies in children with dysphagia, whether of neurological origin or not, are particularly difficult because their natural restlessness associated with the limitations inherent to the available equipment. Inappropriate equipment configuration for swallowing studies, makes it very difficult to properly position children during the study, and more often than not, they end up being overexposed to radiation at the end of a longer than actually necessary examination time. These circumstances can be aggravated by the need for assistance to help in keeping the child properly positioned and to administer the contrast medium necessary for the study. The videofluoroscopic study of swallowing must be performed with the patient in the nearest possible position normally adopted to eat(5). Such position should not be affected by limitations imposed by the equipment. Obtaining a favorable position should always be attempted, particularly to overcome the postural inadequacies generated by the baseline disease. The limitations that shall be accepted, when all overcoming alternatives have been attempted are those inherent to the patient and his/her disease. Limitations resulting from technical difficulties should not be added to neither confused with the patients' limitations. As videofluoroscopy allows noninvasive, appropriate and clear analysis of the oral, pharyngeal and esophageal phases, it is considered as the method of choice for the evaluation of swallowing disorders(6- 11), and it actually is, on account of its effectiveness, the best among the currently available methods(12-16). However, a further reduction in radiation exposure and the inclusion of imaging sequences parameters capable of allowing quantitative analyses still unavailable, represent a significant, necessary, and feasible goal in principle, considering the current technological developments. These are steps that would further enhance the concept of videofluoroscopy as a tool of excellence for the study of the swallowing physiology as well as of the physiopathology of its related disorders. The main objective of the present study was the configuration of a radiological equipment to allow the videofluoroscopic evaluation of swallowing and its dysfunctions with the patient appropriately positioned and with the possibility of easily and comfortably reproducing incidences, postures and maneuvers, independently of limitations imposed by the disease, making it possible to reduce the examination time with consequent reduction of radiation exposure. A second objective of the present study is the development of possibilities for the determination of dimensional variations inherent to the generation of radiological images, by creating a calibration method to allow the recovery of original dimensions of objects from analyses of the images, making it possible to quantify dimensions and movements of structures involved in swallowing.
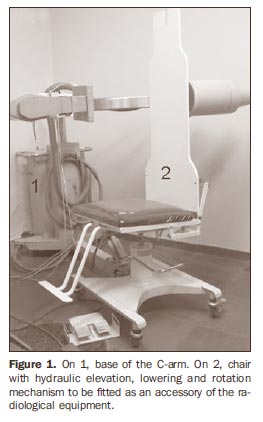
MATERIALS AND METHODS A Philips BV-22 C-Arm model was utilized with a 100 kVp x-ray tube and 20 mA maximum intensity, total nominal filtration of 2.5 mmAl equivalent and 2.4 mm focal point with a fixed anode. The available free space between the end of the x-ray tube cone and the image intensifier was 60 cm. The black-and-white video system is based on the NTSC standard, and is comprised of a Mythos B/W Sony 0.1 lux, f = 3.6 mm minicamera, with 400-line resolution, and a black-and-white 20 inch Philips monitor. Recording resources were added to this video system, allowing simultaneous image capture and analog (Panasonic NVMV 40 video recorder) or digital (Philips DVDR 3455H DVD recorder) recording. These recorders were connected in series, with control image displayed on a Panasonic CT-1383VY color video monitor. A chair was specially built to be utilized in association with the C-arm for video-fluoroscopic study of the three swallowing phases (oral, pharyngeal and esophageal) in such a manner that the examinations could be performed without active participation of individuals in the movements required for obtaining the radiological incidences (Figure 1).
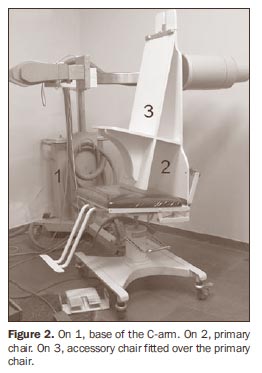
An accessory chair designed to be fit over the first one was also built to accommodate children, particularly those requiring a caregiver assistance during examination (Figure 2).
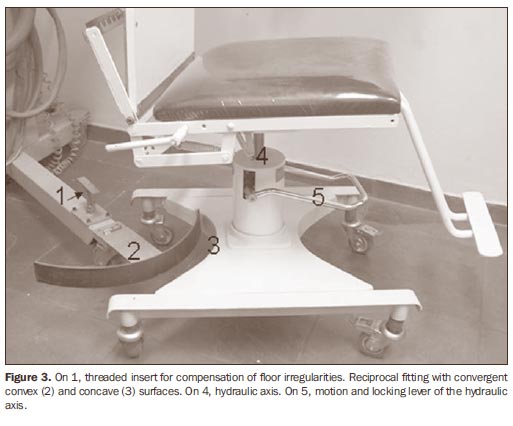
The main chair can be fitted in the space between the x-ray tube and the image intensifier, allowing the elevation or lowering of the seat plane and 360º rotation around its axis, without interfering with the structure of the x-ray equipment. The chair can be removed from the examination position to accommodate a physically disabled patient and then be placed back in the original centralized position by means of reciprocal converging, concave and convex surface fittings installed on the chair basis and adjusted to the C-arm basis. In order not to limit the movement of the chair in relation to the equipment to a centralized position, the convex limiter attached to the equipment can be removed, allowing the free movement of the chair in the space between the x-ray tube and the image intensifier. The rolling and lockable supports of the main chair comprise a hydraulic mechanism that allows the 360º rotation movement as well as a safe 15 cm range of vertical movement of the seat plane (Figure 3).
A backrest is attached to the wide padded seat, with three segments of decreasing widths from the bottom to the top, allowing the patient to be rested against it, with freedom of movement in the free space between the x-ray tube and the image intensifier. The radio-transparent backrest of the main chair is articulated to the seat by a double metallic rack system which is positioned outside (below) the exposure field, providing backrest inclination movement from 90º (vertical) to 10º (close to horizontal) (Figure 4).
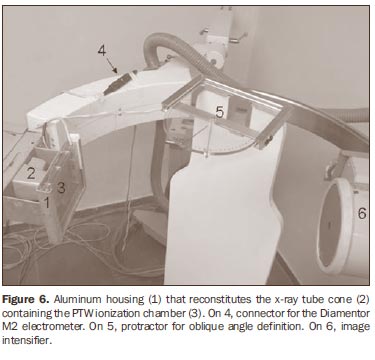
A slot hole at the center of the upper contour of the backrest of the main chair, above the area of radiological exposure, provides attachment means for accessories. The accessory chair for children fits over the main chair. When in place, the accessory chair seat forms an angle of 30º in relation to the frontal plane. Such angle provides a safe positioning of the child during the examination, and is complemented by an additional safety (abdominal) belt. The same fitting point used to attach the accessory chair is also used to attach the calibration plate which is assembled in an articulated T-shaped base that enables its movement in frontal and sagittal planes. The 25 × 25 cm plate has a metallic alloy line grid, forming 2 × 2 cm square cells, vertically and horizontally numbered from the center. This plate is adjusted between 0.5 mm thick acrylic plates, to avoid plane distortion. A 10 cm-diameter opening at the center of one of the acrylic plates generates a circular area of lower density for analysis of the primary beam centralization. The x-ray tube cone kept in its original dimensions, was fitted with a receptacle for the insertion of a PTW ionization chamber which is connected to a Diamentor M2 electrometer that measures the kerma-area product (PKA - unit defined as the product of radiation quantity by the irradiated area)(17,18). A punctual light source attached to the x-ray tube marks the point of incidence of the central ray of the primary beam. A retractable metric scale laterally attached to the image intensifier allows the measurement of the object-intensifier distance, quite useful in the quantification of the recorded images magnifications (Figure 5).
The calibration plate, x-ray tube and the C-arm support base were equipped with spirit levels to allow the correct leveling of the individual parts and also of the whole set up. In order to compensate for eventual floor surface irregularities, the C-arm support base was equipped with leveling feet with threaded inserts. For the definition of angles generated by oblique incidences, an acrylic protractor was designed and built, which attaches to the slot on the upper part of the main chair backrest, allowing the definition, from the lateral incidences, of the angle between the backrest parallel plane and the median sagittal plane of the patient, with the definition of the number of degrees produced by the several oblique incidences (Figure 6).
The main chair was tested with 20 male adult, healthy volunteers with different biotypes, including wind musicians on whom the possible presence of pharyngeal stress signs is studied. The protocol for the present study was previously approved by the Committee for Ethic in Research of the Universidade Federal do Rio de Janeiro, and all volunteers signed a term of free and informed consent. The accessory chair was tested without x-ray emission, with five children with up to 5 years of age.
RESULTS Adult individuals seated on the adapted chair could be mobilized for the required incidences - anteroposterior, postero-anterior, right- and left-lateral, antero-oblique and posterior-oblique, derived from each profile - without having to cooperate in an active manner to obtain the necessary positioning. The distance between a plane of interest of an exposed individual and the image intensifier may be defined both for frontal and lateral incidences, by means of the metric scale attached to the image intensifier. Once the distance between the desired plane and the intensifier is known, the calibration plate is placed on its T-shaped fenestered base, so its grid pattern (with known measures) is registered in an analogous plane to the known one to be occupied by the study object. The dimensional variations related to the plate and its image allows the quantification of dimensional variations occurring in the object. The dimensional variations of the plate are similar to those of the exposed object. The images of the plate with the hypotransparent central area also serve the purpose of detecting possible distortions and irregularities, even the subtle ones, in the peripheral zone of the obtained images. In the system adopted in the present study, the measured distortion was in the order of 3% (maximum tolerance: 10%, referenced on the Order (Portaria) 453)(19). The reciprocal fitting (chair/equipment) allowed its removal and repositioning in the previous centralized position. The free horizontal movement of the chair after removal of the reciprocal fitting has a range of 30 cm. Its median sagittal plane can be moved 15 cm closer to the surface of the image intensifier, generating images with smaller distortions and dimensions closer to the actual size of the objects. The free vertical displacement required for the observation of structures involved in the three phases of swallowing, is achieved by the hydraulic mechanism of the chair. Such displacement range can be increased by associating the hydraulic movement of the chair with the electrically provided vertical movement of the x-ray tube-intensifier structure. The punctual light source attached to the equipment allowed the correct localization of the areas to be irradiated, thus avoiding the need for additional radiation exposure. The accommodation of children on the accessory chair proved to be effective, and the mobility of the system, simulating several incidences, proved to be extremely nimble and easy. Furthermore, depending upon particular needs of the child, an assistant can help during the study, positioning himself posteriorly to the segment of the C-arm that holds the x-ray tube.
DISCUSSION The videofluoroscopic method, with different designations(20-26), is considered and accepted as the most appropriate method for diagnosis and follow-up of most of dysphagic processes(12-15). However, and quite often, the method is criticized due to the fact of using x-radiation as the image-generating element(9) and, with the recognition of its qualitative potential it is also desirable that the method provides a quantification of the investigated events. Radiation doses required for the investigation of swallowing dynamics can be considered as being low as compared with those necessary for the performance of the majority of radiological studies accepted and recognized as important, valid and in use in the clinical practice(26). The biased concept of high doses certainly comes from non-intensified (dark room) fluoroscopy, where the necessary doses to achieve quality images was high indeed. The addition of monitors to the conventional fluoroscopy process, with the use of a camera and an image intensifier, resulted in a significant reduction in the radiation exposure, both for the patient and the radiologist. The image analysis that previously required high radiation doses and slow adaptation to a totally dark room, has been replaced by the analysis on a monitor screen in a normally lit room, with much lower doses than those previously required(26-31). However, videofluoroscopy can be performed with even lower doses. Usually, unnecessary exposure ends up happening due to technical difficulties in comply with an evaluation protocol utilizing inappropriate, improvised radiological equipment to perform the study. Additionally, there are those difficulties found in the evaluation of children and also those specific to patients with motor deficits associated with swallowing disorders. Technical difficulties in the examination increase the exposure times, limit the information that can be obtained and cause repetitions that produce new and undesirable exposures. Furthermore, an inappropriate positioning of the patient may negatively interfere, generating additional difficulties in swallowing or enhancing the existing ones, causing difficulties imposed by the precarious structural condition to be erroneously perceived as diseases. This fact is particularly relevant for children and patients with motor deficits. An appropriate evaluation of the swallowing dynamics and related disorders comprise the study of oral, pharyngeal and esophageal phases requiring a protocol involving the evaluation of several regions with different densities and incidences that cannot be neglected with the sole intent of reducing radiation exposure time. It is possible to perform a swift exam, thus reducing exposure times, with patients capable of properly positioning themselves, understanding and acting according to requests necessary for compliance with the protocol of an appropriate investigation of the swallowing phases. However, children, patients with motor deficits and those with a low cooperation capacity end up requiring additional exposure times, which should always be kept at the minimum necessary levels. The development of adaptations with the objective of providing the radiological equipment with specificity for the video-fluoroscopic study of swallowing is certainly the correct way to reduce or even eliminate technical restrictions, with consequent lower radiation exposure for both the patient and the investigator. This solution was first proposed by Cox & Petty(32), with the development of a special chair to be utilized with patients with severe neuromotor diseases. The chair proposed by the present study is more complete, incorporating an accessory chair for evaluation of children, and other resources such as elements that allow the inclusion, in the images, of parameters for the desirable real time quantification of the phenomena and linear measurement of dimensional variations of the recorded structures. Based on the results of the present study, the developed chair in association with the C-arm, will effectively meet the positioning needs, particularly for those patients incapable of active participation and cooperation, whether adults or children, allowing them to be positioned and evaluated with freedom in the different necessary radiological incidences that so far were inaccurate and difficult to obtain. Besides benefiting patients that could not undergo the procedure due to the severity of their motor deficits, the implementation of the present project will facilitate the study protocols accomplishment, reducing the required time for their performance and the final radiation dose employed. The quantification of events in the pharyngeal and esophageal phases has been a focus of radiological methods(33,34). The utilization of this chair and the current stage of videofluoroscopy will allow the selection and quantification of the phenomena whose measurement adds information to the qualitative data allowed by videofluoroscopic evaluation(35,36). Videofluoroscopy, in principle defined as a method capable of recording the swallowing dynamic on magnetic tapes (VHS), has progressed to a method that can be defined as capable of real-time recording on magnetic media of the swallowing dynamics images. The standardization of the number of images in a given unit of time, the advent of digitalization and the possibility of insertion in the image of an element of known measures to be compared with the structure to be measured, make the quantification of dimension and time variations, an easy task. With the chair adapted to the C-arm, it is possible, with the use of the calibration plate, to establish the produced magnification at every point, between the x-ray tube and the image intensifier, and compare the dimensional variations of this pattern with the variations occurring in the object under study, positioned in the same localization between the x-ray tube and the intensifier. It is also easy to measure the duration of an event recorded in its dynamics. The time interval recorded on analog or digital media has a known number of frames per unit of time (second). In the NTSC-M system, the most frequently utilized in videofluoroscopy, the number of frames per second is 29.97, with each frame lasting 33 thousandths of a second. Thus, by counting the number of frames in an event and multiplying this number by 0.033, the duration of the event in seconds is determined. The permanent control of the distance between the object under study and the image intensifier, and the knowledge of the magnification values of the calibration plate provided by the chair at any point of the space between the x-ray tube and the image intensifier, at any of the radiological incidences, allows the calculation, by analogy, of the dimensional magnifications. By knowing the number of frames recorded in a unit of time, the duration in seconds of a dynamic event can be easily determined provided it is possible to identify in the sequence of images, the fames depicting the beginning and the end of the phenomenon. The possibility provided by the use of the chair in allowing the measurement of the events duration and the linear values of recorded phenomena, turns videofluoroscopy into a quantitative method, enhancing its qualitative possibilities, already considered as the ones with greater applicability in the study of swallowing and related disorders. The qualitative importance of the method should be pointed out, however, since this is what clearly defines the referential to be measured and what is in fact important to be measured, in order not to make the frequent mistake of measuring simply for the sake of measuring.
CONCLUSIONS The main and accessory chairs coupled to the radiological equipment were capable of accommodating and allowing all required radiological incidences without the active participation of individuals, whether adults or children, as it would happen with neuromotor impaired patients with extensive limitations. This fact not only increases the range of application of videofluoroscopy, but also makes it more effective, with shorter examination times and, consequently, lower radiation exposure. The inclusion of a calibration plate, with the possibility of quantification, increases the excellence of the method which is considered as the one with greatest qualitative effectiveness for allowing the noninvasive morphofunctional analysis of the three phases of swallowing.
REFERENCES 1. Lawrence ES, Coshall C, Dundas R, et al. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke. 2001;32:1279-84. [ ] 2. Aviv JE, Sacco RL, Thomson J, et al. Silent laryngopharyngeal sensory deficits after stroke. Ann Otol Rhinol Laryngol. 1997;106:87-93. [ ] 3. Daniels SK, Brailey K, Priestly DH, et al. Aspiration in patients with acute stroke. Arch Phys Med Rehabil. 1998;79:14-9. [ ] 4. Ramsey DJC, Smithard DG, Kalra L. Early assessments of dysphagia and aspiration risk in acute stroke patients. Stroke. 2003;34:1252-7. [ ] 5. Costa MMB. Uso de bolo contrastado sólido, líquido e pastoso no estudo videofluoroscópico da dinâmica da deglutição. Radiol Bras. 1996;29:35-9. [ ] 6. Beck TJ, Gayler BW. Image quality and radiation levels in videofluoroscopy for swallowing studies: a review. Dysphagia. 1990;5:118-28. [ ] 7. Jones B, Kramer SS, Donner MW. Dynamic imaging of the pharynx. Gastrointest Radiol. 1985; 10:213-24. [ ] 8. Linden P. Videofluoroscopy in the rehabilitation of swallowing dysfunction. Dysphagia. 1989;3:189-91. [ ] 9. Linden P, Siebens AA. Dysphagia: predicting laryngeal penetration. Arch Phys Med Rehabil. 1983;64:281-4. [ ] 10. Robbins JA, Logemann JA, Kirshner HS. Swallowing and speech production in Parkinson's disease. Ann Neurol. 1986;19:283-7. [ ] 11. Wilson PS, Bruce-Lockhart FJ, Johnson AP. Videofluoroscopy in motor neurone disease prior to cricopharyngeal myotomy. Ann R Coll Surg Engl. 1990;72:375-7. [ ] 12. Bisch EM, Logemann JA, Rademaker AW, et al. Pharyngeal effects of bolus volume, viscosity, and temperature in patients with dysphagia resulting from neurologic impairment and in normal subjects. J Speech Hear Res. 1994;37:1041-9. [ ] 13. Gottlieb D, Kipnis M, Sister E, et al. Validation of the 50 ml drinking test for evaluation of post-stroke dysphagia. Disabil Rehabil. 1996;18:529-32. [ ] 14. Macedo-Filho ED. Avaliação endoscópica da deglutição no diagnóstico da disfagia orofaríngea. In: Costa MMB, Leme EMO, Koch HA. Temas em deglutição e disfagia: abordagem multidisciplinar. Rio de Janeiro: PAEDD; 1998. p. 77-82. [ ] 15. Noll SF, Bender CE, Nelson MC. Rehabilitation of patients with swallowing disorders. In: Braddom RL, editor. Physical medicine and rehabilitation. Philadelphia: Saunders; 2000. p. 535-57. [ ] 16. Costa MMB, Monteiro JS. Exame videofluoroscópico das fases oral e faríngea da deglutição. In: Costa M, Castro LP. Tópicos em deglutição e disfagia. Rio de Janeiro: Medsi; 2003. p. 273-84. [ ] 17. International Commission on Radiological Protection. ICRP Publication 73: Radiological protection and safety in medicine, 73. Annals of the ICRP. 1997;26(2). [ ] 18. International Atomic Energy Agency. Dosimetry in diagnostic radiology. An international code of practice. Technical Reports Series No. 457. Vienna: IAEA; 2007. [ ] 19. Cowen AR, Clarke OF, Coleman NJ, et al. Leeds x-ray test objects instruction manual. Leeds: University of Leeds; 1992. [ ] 20. Lefebvre MM, Sauvegrain J, Fortier-Beaulieu M. Indications et résultats du radiocinema et de la radiotélévision en pathologie digestive infantile. Arch Mal Appar Dig. 1962;51:1044-6. [ ] 21. Skolnick ML. Videofluoroscopic examination of the velopharyngeal portal during phonation in lateral and base projections - a new technique for studying the mechanics of closure. Cleft Palate J. 1970;7:803-16. [ ] 22. Curtis DJ, Sepulveda GU. Epiglottic motion: video recording of muscular dysfunction. Radiology. 1983;148:473-7. [ ] 23. Palmer JB, Tanaka E, Siebens AA. Motions of the posterior pharyngeal wall in swallowing. Laryngoscope. 1988;98:414-7. [ ] 24. Winnberg A, Pancherz H, Westesson PL. Head posture and hyo-mandibular function in man. A synchronized electromyographic and videofluorographic study of the open-close-clench cycle. Am J Orthod Dentofacial Orthop. 1988;94:393-404. [ ] 25. Yotsuya H. An x-ray TV cinematographical study on relation of the movements of the hyoid bone, the tongue radix, the epiglottis and the soft palate during deglutition (author's transl). Shikwa Gakuho. 1981;81:1-46. [ ] 26. Costa MMB, Nova JLL, Carlos MT, et al. Videofluoroscopia: um novo método. Radiol Bras. 1992;25:11-8. [ ] 27. Airth GR. Image requirements. In: Hospital Physicists' Association (conference reports series-26) Quality control in diagnostic radiology. London: Hospital Physicists' Association; 1976. p. 26-7. [ ] 28. Costa MMB, Canevaro LV, Azevedo ACP, et al. Valores típicos do "produto dose área" (DAP) obtidos durante o estudo videofluoroscópico da deglutição. Radiol Bras. 2003;36:17-20. [ ] 29. Costa MMB, Canevaro LV, Azevedo ACP. Avaliação dosimétrica do método videofluoroscópico aplicado ao estudo da dinâmica da deglutição. Radiol Bras. 2000;33:353-7. [ ] 30. Costa MMB, Canevaro LV, Azevedo ACP. Dosimetric assessment of swallowing examinations with videofluoroscopy. International Conference on the Radiological Protection of Patients in Diagnostic and Interventional Radiology, Nuclear Medicine and Radiation Therapy; 2001 Mar; Malaga, Spain. [ ] 31. Costa MMB. Dose referência: quantificação das doses de raios-x necessárias ao estudo videofluoroscópico da deglutição. SIICSalud, Expertos del Iberoamérica; 2004. [Acessado em 20 de maio de 2007]. Disponível em: http://www.siicsalud.com/dato/dat042/05414002.htm [ ] 32. Cox MS, Petty J. A videofluoroscopy chair for the evaluation of dysphagia in patients with severe neuromotor disease. Arch Phys Med Rehabil. 1991;72:157-9. [ ] 33. Lynch CS, Chammas MC, Mansur LL, et al. Biomecânica ultra-sonográfica da deglutição: estudo preliminar. Radiol Bras. 2008;41:241-4. [ ] 34. Sakate M, Teixeira AS, Yamashita S, et al. Um novo método de avaliação do "tempo esofágico" com ultra-sonografia por abordagem externa. Radiol Bras. 2008;41:309-12. [ ] 35. Costa MMB, Moreno MPR. Videomed. Software sem registro de patente desenvolvido pelo Núcleo de Computação Eletrônica da Universidade Federal do Rio de Janeiro. Rio de Janeiro: NCE/UFRJ; 2000. [ ] 36. Spadotto AA, Gatto AR, Cola PC, et al. Software para análise quantitativa da deglutição. Radiol Bras. 2008;41:25-8. [ ] Received November 11, 2008. * Study developed at Instituto de Ciências Biomédicas and Department of Radiology -Faculdade de Medicina da Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. Financial support: Fundação Educacional Charles Darwin. |
|



Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554