Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 3 - May / June of 2009
Vol. 42 nº 3 - May / June of 2009
|
ORIGINAL ARTICLE
|
|
Signs of hypervascularization at magnetic resonance imaging in bone metastases from renal cell carcinoma |
|
|
Autho(rs): Leonir Terezinha Feltrin, José Renato Ferreira, Augusto Elias Mamere, Rafael Darahem de Souza Coelho, Alexandre Oliveira Cecin, Fabiano Rubião Lucchesi, Marco Antônio Lopes Pinheiro, Clóvis Simão Trad |
|
|
Keywords: Bone metastases, Renal cell carcinoma, Magnetic resonance imaging, Hypervascularization |
|
|
Abstract:
IMasters, MDs, Radiologists, Hospital de Câncer de Barretos - Fundação Pio XII, Barretos, SP, Brazil
INTRODUCTION Renal cell carcinomas (RCC) correspond to 3% of neoplasms(1). Metastases indicate the worst prognosis, and the most frequent sites are lungs, bones, central nervous system and adrenal glands(2). Bone metastases are found in 20-60% of patients with RCC(3) and may be the first sign of this neoplasm in 48% of patients(4). In cases where the spine is involved, the bone lysis may be associated with mechanical instability, severe pain, radiculopathies and symptoms of nervous compression. Surgical decompression and stabilization constitute the treatment of choice for radiotherapy-resistant lesions(5). Long bones with metastatic lesions are also frequently submitted to surgical management, especially in cases where fractures are present. RCC metastases are highly vascularized(6) and sometimes result in intense intraoperative bleeding(7). Thus the observation of this intense vascularization on imaging studies may be useful to the surgeon performing a biopsy or surgical resection as a warning sign regarding the possibility of bleeding. Additionally, the presence of hypervascularization may suggest the renal etiology of a bone metastasis whose primary tumor is unknown. The present study is aimed at evaluating the frequency of this sign observed at magnetic resonance imaging (MRI) studies of patients with bone metastases from RCC.
MATERIALS AND METHODS The present study retrospectively evaluated MRI examinations showing 15 lesions in 13 patients - 4 women and 9 men, age range between 37 and 69 years (mean, 52 years) - with renal cell neoplasm and bone metastases. The diagnoses of bone metastases were based on previous radiological and histopathological findings of RCC. MRI studies were performed in a 1.5 T Magnetom Symphony (Siemens; Erlangen, Germany) equipment, with T1- and T2weighted TSE sequences and 3 mm-thick slices for all of the patients. Seven patients received intravenous contrast agent (gadolinium) for pre- and post-contrast, multi-planar, T1-weighted acquisitions. All the lesions were evaluated before surgery, chemotherapy, arterial embolization or radiotherapy. The lesions were independently and retrospectively evaluated by two radiologists with experience in bone lesions, considering the signal intensity and presence/absence of hypervascularization. The presence of hypervascularization at MRI was defined as the visualization of multiple spots and tubular structures with hyposignal intensity on all the sequences, corresponding to vessels within or surrounding the lesion.
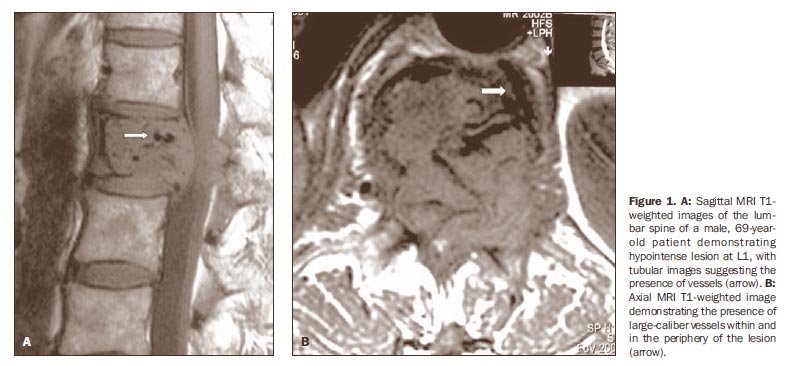
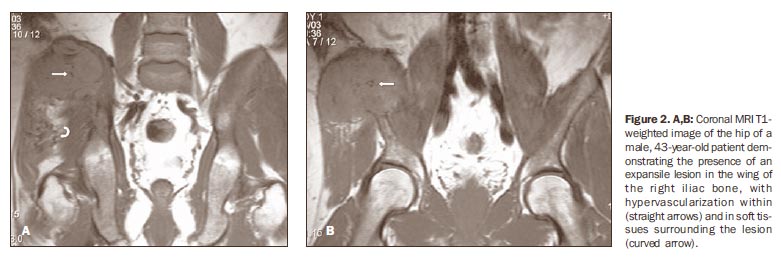
RESULTS Among the 13 patients with bone metastasis from renal cell carcinoma, 15 lesions were found, as follows: 6 in the lumbar spine, 3 in the thoracic spine, 3 in the hip, 1 in the humerus, 1 in the ulna, and 1 in the tibia. In two cases lesions were found in both the lumbar spine and hip. Vessels (sign of hypervascularization) were found within the lesions (Figures 1, 2 and 3) and in the periphery (Figures 2 and 3) in 12 of the 15 lesions (80%), 6 of them in the lumbar spine, 3 in the hip, 1 in the thoracic spine, 1 in the ulna, and 1 in the tibia.
Two patients with metastasis to the lumbar spine were submitted to surgery (because of medullary compression), with intense intraoperative bleeding. One of these patients presented hypovolemic shock. The other patients were treated with radiotherapy.
DISCUSSION Signs of hypervascularization (flow void) as an imaging finding frequently observed in RCC metastases have been described by Choi et al.(8), being reported in 76.7% of 20 cases studied. Uchino et al.(9) have evaluated MRI studies of patients with single intracranial metastasis of RCC, reporting intra- and/or peritumor vessels in five of among seven cases. Nguyen et al.(10) have reported a case of RCC with visible vessels within a thrombus invading the inferior vena cava and the right atrium. In spite of being very frequently found, the presence of hypervascularization is not RCC-specific. Hypervascularization is also found in other less common lesions, such as arteriovenous malformations, high-flow hemangiomas and alveolar soft part sarcoma(11,12). Kawahara et al.(13) have reported a case of hepatocellular carcinoma metastasis to calvaria presenting signs of hypervascularization (flow void) at MRI. It is known that tumors such as thyroid melanomas and carcinomas present hypervascularization. However, no report has been found in the literature about observation of vessels within metastases of these tumors. Similarly to data in the literature, the authors of the present study have found signs of hypervascularization in 80% of cases. Although these signs have been described in studies with small samples, their high frequency allows the authors to affirm that the presence of hypervascularization within or surrounding bone lesions must suggest the evaluation of the kidney as the primary site of the neoplasm. In cases where the primary tumor is already known and a surgical treatment is indicated, the surgeon must be warned about the presence of these large, newly formed vessels(14), to prevent eventual intraoperative complications (hemorrhage).
CONCLUSION The presence of hypervascularization (flow void) within or in the periphery of multiple or single bone lesions should be considered as an indication for investigation of the kidney as primary site of the tumor. The surgeon must be warned about the presence of these vessels, in order to prevent complications resulting from intraoperative hemorrhage.
REFERENCES 1. Boring CC, Squires TS, Tong T, et al. Cancer statistics, 1994. CA Cancer J Clin. 1994;44:7-26. [ ] 2. Thrasher JB, Paulson DF. Prognostic factors in renal cancer. Urol Clin North Am. 1993;20:247-62. [ ] 3. Saitoh H. Distant metastasis of renal adenocarcinoma. Cancer. 1981;48:1487-91. [ ] 4. Nielsen OS, Munro AJ, Tannock IF. Bone metastases: pathophysiology and management policy. J Clin Oncol. 1991;9:509-24. [ ] 5. Sundaresan N, Scher H, DiGiacinto GV, et al. Surgical treatment of spinal cord compression in kidney cancer. J Clin Oncol. 1986;4:1851-6. [ ] 6. Prando A. Achados da tomografia computadorizada em metástases pancreáticas do carcinoma de células renais. Radiol Bras. 2008;41:225-8. [ ] 7. King GJ, Kostuik JP, McBroom RJ, et al. Surgical management of metastatic renal carcinoma of the spine. Spine. 1991;16:265-71. [ ] 8. Choi JA, Lee KH, Jun WS, et al. Osseous metastasis from renal cell carcinoma: "flow void" sign at MR imaging. Radiology. 2003;228:629-34. [ ] 9. Uchino A, Hasuo K, Mizushima A, et al. Intracranial metastasis of renal cell carcinoma: MR imaging. Radiat Med. 1996;14:71-6. [ ] 10. Nguyen BD, Westra WH, Zerhouni EA. Renal cell carcinoma and tumor thrombus neovascularity: MR demonstration with pathologic correlation. Abdom Imaging. 1996;21:269-71. [ ] 11. Rak KM, Yakes WF, Ray RL, et al. MR imaging of symptomatic peripheral vascular malformations. AJR Am J Roentgenol. 1992;159:107-12. [ ] 12. Suh JS, Cho J, Lee SH, et al. Alveolar soft part sarcoma: MR and angiographic findings. Skeletal Radiol. 2000;29:680-9. [ ] 13. Kawahara I, Tsutsumi K, Hirose M, et al. Skull metastasis of hepatocellular carcinoma: case report. No Shinkei Geka. 2005;33:903-9. [ ] 14. Baroni RH. Novos paradigmas na avaliação por imagem dos tumores parenquimatosos renais. Radiol Bras. 2008;41:v-vi. [ ] Received March 11, 2008. * Study developed at Hospital de Câncer de Barretos - Fundação Pio XII, Barretos, SP, Brazil. |
|


{kind=link}
{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554