Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 43 nº 1 - Jan. /Feb. of 2010
Vol. 43 nº 1 - Jan. /Feb. of 2010
|
ORIGINAL ARTICLE
|
|
Ureteric jet Doppler waveform: interobserver agreement. A prospective study with asymptomatic children |
|
|
Autho(rs): Carolina Freitas Lins, Gabriela Ferreira Lima, Adonis Born Muniz Filho, João Vicente Ribeiro Neto, Silvio Cavalcanti de Albuquerque, Eduardo Just da Costa e Silva |
|
|
Keywords: Ureter, Urination, Children |
|
|
Abstract:
IMDs, Radiologists at Instituto de Medicina Integral Prof. Fernando Figueira, Recife, PE, Brazil
INTRODUCTION Voiding dysfunction occurs when one of the components of the normal voiding process is affected, causing such component not to function in an integrated manner. The alterations in the function of the lower urinary tract may be divided into neurological (neurogenic bladder), most frequently resulting from spinal dysraphism and cerebral palsy; and functional, caused by disorders in children with no evidence of neurological diseases(1,2). The relevance of early diagnosis is related to the possibility of establishing the treatment in order to minimize the social and psychological repercussions of urinary incontinence and avoiding renal injury with development of scarring and function loss(1). The urodynamic study allows the confirmation of the diagnosis of lower urinary tract dysfunction(1). By means of such study it is possible to evaluate the functions of bladder storage and emptying and the activity of the ureteral sphincter complex. However, the urodynamic assessment is not always available, besides the fact of being considered as an invasive procedure because of the need of using urethral catheterism(1-3) . The ureteric jet is a phenomenon caused by urine ejection into the vesical lumen by ureteral peristalsis(1,4,5). This phenomenon can be visualized with the use of color Doppler(6). Studies evaluating the ureteric jet by means of spectral Doppler demonstrate the presence of six waveform patterns as follows: monophasic, biphasic, triphasic, polyphasic, square and continuous(2-4,6-9) . As far as the ureteric jet is concerned, the diagnosis of urinary diseases, including vesical dysfunctions, is highly associated with clinical data of the patients and those of Doppler ultrasonography(2,4,5,8). However, as the evaluation of the ureteric jet is based on the observation of a spectral curve, difficulties in its interpretation may be raised because of individual variations among investigators with regards to patterns classification caused by different understanding of what characterizes the different patterns. The present study is aimed at evaluating the interobserver agreement on different ureteric jet patterns in children without urinary complaints.
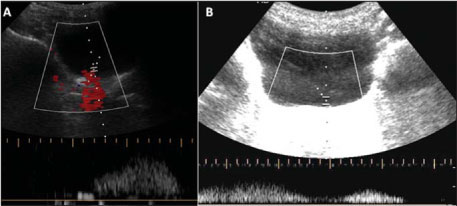
MATERIALS AND METHODS The present prospective study was previously approved by the Committee for Ethics in Research of the Institution. Free and informed consent was obtained from parents or guardians of the children. The sample of the present study included children in the age range between 6 and 12 years referred to the unit of imaging diagnosis service of a pediatric school hospital to be submitted to ultrasonography because of complaints not related to the urinary tract. The sampling method was non casual and by convenience. Patients whose examination was scheduled for a certain time during the week were selected. Such sampling method was chosen for allowing the inclusion of patients that were examined when the radiologists involved in the present study were present in the unit. The patients followed the standard recommendations for abdominal ultrasonography. In the authors' institution, US studies are scheduled for specific days in the week by order of arrival, with no preferential scheduling for any specific time slot, so that, in principle, the sampling is not affected by any special characteristic that might contribute to a selection bias. Patients with a previous history of urinary surgery or anatomic abnormalities likely to be detected at ultrasonography were excluded. The sample size was arbitrarily defined, considering that data on the appropriate sample size for studies involving kappa statistics are scarce in the literature. Variables The waveform patterns were classified into six types according to Leung et al.(4,6). A monophasic jet is characterized by one peak. Biphasic and triphasic jets are characterized by two and three peaks, respectively. Four or more peaks characterize a polyphasic jet. A wave with a plateau format with a duration of up to 20 seconds characterizes a square pattern, while a duration above 20 seconds characterizes a continuous jet(2). Operationalization The patients were sequentially examined by two sonographers, one of them a specialist in clinical pediatrics and radiology, with a five-year experience in pediatric radiology. The other investigator had a three-year experience in general and pediatric ultrasonography. The patients were not stimulated to drink a larger than usual amount of liquids, being instructed to inform when the voiding desire started, in order to initiate the study, avoiding the examination with a strong voiding desire. All the patients were evaluated in the supine position, with the bladder being observed in the transverse plane and identification of the ureteric jets with the aid of color Doppler. After obtaining the signal with the color Doppler, samples of the spectral curves were obtained for each ureteric jet. The Doppler sample volume was sufficiently wide to comprise the whole ureteric jet and was positioned on the center of the jet which corresponded to the point of largest flow. The angle was limited to remain between 30° and 60°. For each patient, three successive waves of the ureteric jets from each side were obtained. The number of peaks on each wave was observed and classified, with the most frequent one being selected whenever a variation occurred among the three samples. The maximum peak velocity of the highest peak was also observed. Statistical analysis The kappa coefficient (κ) was calculated to evaluate the interobserver agreement in relation to the results regarding wave types(10). Velocities were compared by means of the Students t-test. A significance level of 95% was adopted.
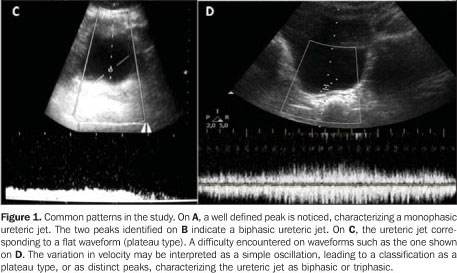
RESULTS A total of 41 children (82 ureteric jets) were evaluated. In the cases of two children, the evaluation of one ureter was compromised as these children became uncooperative before the end of the examination. Thus, 80 ureteric jets were evaluated by one observer and 82 by the other, therefore corresponding to 486 waveforms. The mean examination time was not recorded; however extremely long or difficult examinations were scarce. The interobserver agreement was moderate (κ = 0.48; 95% confidence interval: 0.36-0.60). The most frequent jet pattern was the square type, visualized in 186 jets (38.2%). The other types were detected as follows: biphasic, 119 (24.4%); monophasic, 101 (20.7%); triphasic, 64 (13.1%); continuous, 10 (2%) and polyphasic, 6 (1.2%). No statistically significant difference was observed between the two observers with respect to the patterns frequency (p = 0.41). Figure 1 shows the most common patterns in the study. One difficulty observed by the investigators was the differentiation between small oscillations on square jets and true peaks (Figure 1D).
The maximum jet velocities observed by the investigators were 32.37 cm/s and 35.63 cm/s, respectively, with no statistically significant difference (p = 0.25). Also, statistically significant differences were not observed between maximum velocities observed in the right and left ureters either. Among the ureteric jet evaluations there were variations in the waveform types per ureter in the three samples in 47 (29%).
DISCUSSION The present results demonstrate a moderate interobserver agreement regarding the type of ureteric jet observed at the color Doppler study in children. No statistically significant difference was observed in the evaluation of the maximum jet velocity. The square pattern was the most frequently observed, followed by the biphasic pattern. The identification of ureteric jets on imaging studies such as gray scale ultrasonography and excretory urography is common. The utilization of color Doppler facilitates such visualization, even in individuals under normal hydration conditions(11). Early studies have identified curve patterns at the spectral Doppler study, particularly characterized by the presence of peaks in variable numbers, or by continuous tracing without peaks(3,11). The classification proposed by Leung et al. comprises six different types of wave patterns, and has been the subject of several studies(2,4,7-9,12) . Such observations have generated theories that try to better explain the physiology of the ureterovesical junction. Such theories range from a passive participation to a possible functional sphincter function (active) of such junction(6). A double regulating component of such passive function has been proposed, compounding a neural element and a myogenic one. The presence of a monophasic wave pattern has been observed in situations in which the neural component would be suppressed, such as in infants, individuals under anesthesia and others, which has led to the denomination of immature pattern(6-9). The biphasic, triphasic and polyphasic patterns are considered as mature patterns. The continuous and square patterns are considered as being related to conditions of forced diuresis. Several physiological situations seem to interfere in the patterns observed in humans, such as pregnancy, anesthesia, age, sex and hydration status(6,7,9). The relevance of the study of such patterns is the demonstration of a possible relation between the occurrence of the immature pattern and the presence of urinary tract diseases, such as vesicoureteral reflux, urinary infection and nocturnal enuresis(4,8), with the possibility that further studies bring a significant contribution to the understanding of the physiopathology and diagnosis of these common conditions in children, which are still in need of a defined investigation strategy(13). The introduction of new methods or patterns, either in the daily clinical practice or in research models, must always take into consideration the reproducibility of proposed findings, i.e., the capacity of obtaining similar results when the examination in a same patient, under the same physiological conditions is performed by different investigators or equipment. A common way of testing the imaging studies performance is the evaluation of the interobserver agreement. The moderate interobserver agreement in the evaluation of ureteric jet patterns observed in the present study must be cautiously evaluated, as there is no other study approaching this matter in the literature. In the author's institution, such type of evaluation is not yet a part of the daily routine. A square like pattern may be easily confused with a polyphasic or triphasic pattern, considering that minimum variations in the wave's height may be interpreted as peaks or not. This difficulty was experienced by the authors as the present study was developed. A great number of studies evaluating the patterns approached in the present study have been developed by a single group with a wide experience in this type of imaging study, which contributes to a better standardization of findings interpretation. More strict parameters for the definition of a peak may be instrumental in reducing this variation in a clinical or research practice. For example, a peak might be differentiated from a non significant variation in velocity either by the variation or by its relation with the mean velocity. A longer learning curve would be another form of improving the interobserver agreement, contributing to the method application. Other possible explanation for the moderate interobserver agreement, which is coherent with the current level of knowledge about ureteric jets behavior, lies on the fact that the imaging studies were sequentially evaluated. It is already known that the ureteric jets morphology vary as the bladder becomes full. So, the ureteric jets may have presented variations over time, which may have contributed to the level of interobserver agreement. An effort was made to maintain the closest possible temporal proximity between the two investigators evaluations in order to minimize such an effect. The instruction to patients about not drinking more liquids than usual was an attempt to avoid rapid variations in the vesical volume. However this bias certainly could not be completely eliminated with this measure. Again, the absence of similar studies evaluating the interobserver agreement on the patterns does not allow comparisons to be made. A proposal for a study that could eliminate this variable would be obtaining hard copies of the waveforms which would then be separately evaluated by two different investigators. The predominance of the square pattern observed by the present study group is different from reports in the literature(2). Some factors may have contributed for such a discrepancy. As previously described, the difficulty in characterizing a waveform may have easily biased many patterns of the triphasic or polyphasic types to a square type classification. Moreover, the patients were evaluated under physiological conditions, without being instructed to drink a larger than usual amount of liquids. In the previously mentioned studies, the patients were always instructed to drink large volumes of liquids. Considering that the patterns are known to be influenced by physiological conditions, this would be a plausible further explanation for the difference in patterns. Curiously, the square pattern is usually related to situations of forced diuresis, which was not the case with the patients in the present study(6). However, the evaluation of pattern predominance was not the objective of the present study, so that following the same method employed in other studies in the literature would not be strictly necessary, provided the two observers evaluated the patients under identical conditions. The maximum velocities of the evaluated peaks did not present a significant interobserver variation, and are similar to those described in the literature(2). The fact that 57% of the evaluations demonstrated variations of wave type in the three samples may indicate a limitation of the method, as more samples per ureter might be necessary to define the predominant pattern. Such finding is similar to the one reported by Leung et al.(4). A proposed explanation for the variation would be the increase in urine volume in the bladder during the examination, affecting the correspondent waveform shape(6). This fact is particularly relevant, as a child presenting two patterns of the biphasic type and one pattern of the monophasic type would be considered as presenting a mature pattern. A new sample in this same ureter presenting a monophasic pattern would be enough to change the classification to immature. It is possible that in future researches a higher number of samples may be defined in order to characterize the predominant pattern, making the evaluation less susceptible to ureteric jets occasionally observed out of the pattern. Another practical measure would be establishing maximum vesical volumes, above which the ureteric jets should not be evaluated. The present study faced several limitations. Although they have previously been mentioned, it is convenient to review them in this topic. The fact that the ureteric jet evaluation by means of color Doppler is not routinely performed in the authors' institution was certainly one of them, since a greater experience with the method could improve the interobserver agreement. The sample size is another factor that that may have reduced eventual differences from a statistical point of view. There was no standardization of the hydration level of the children, which may have contributed to the occurrence of patterns that are less frequently found in children. Further studies should evaluate the average time spent in the performance of the examinations, to better define its feasibility in the daily practice. In conclusion, the study of wave patterns of ureteric jets by means of color Doppler is a method that demonstrated a moderate interobserver agreement. A better definition of the parameters for differentiation between waveform types and a longer learning curve may be useful for the application of the method. The observed variation between wave patterns obtained from the same ureter in different samples, indicates a possible necessity of a higher number of waveforms per ureter for the definition of the predominant type. Further studies including the evaluation of hard copies of the waveforms by different observers may prove to be useful.
REFERENCES 1. Fonseca EM, Monteiro LM. Clinical diagnosis of bladder dysfunction in enuretic children and adolescents. J Pediatr (Rio J). 2004;80:147-53. [ ] 2. Leung VY, Chu WC, Yeung CK, et al. Ureteric jet Doppler waveform and bladder wall thickness in children with nocturnal enuresis. Pediatr Res. 2006;60:582-6. [ ] 3. Cox IH, Erickson SJ, Foley WD, et al. Ureteric jets: evaluation of normal flow dynamics with color Doppler sonography. AJR Am J Roentgenol. 1992;158:1051-5. [ ] 4. Leung VY, Metreweli C, Yeung CK. The ureteric jet doppler waveform as an indicator of vesico-ureteric sphincter function in adults and children. An observational study. Ultrasound Med Biol. 2002;28:865-72. [ ] 5. Sakate M, Teixeira AS, Sakate ATY, et al. Study of the ureterovesical jet by means of color Doppler in patients with and without vesicoureteral reflux. Radiol Bras. 2006;39:425-8. [ ] 6. Leung VY, Chu WC, Yeung CK, et al. Doppler waveforms of the ureteric jet: an overview and implications for the presence of a functional sphincter at the vesicoureteric junction. Pediatr Radiol. 2007;37:417-25. [ ] 7. Leung VY, Metreweli C. Doppler waveform of the ureteric jet in pregnancy. Ultrasound Med Biol. 2002;28:879-84. [ ] 8. Leung VY, Metreweli C, Yeung CK. Immature ureteric jet doppler patterns and urinary tract infection and vesicoureteric reflux in children. Ultrasound Med Biol. 2002;28:873-8. [ ] 9. Leung VY, Metreweli C, Yeung CK, et al. Ureteric jet in the anaesthetised child. Ultrasound Med Biol. 2003;29:1237-40. [ ] 10. Kundel HL, Polansky M. Measurement of observer agreement. Radiology. 2003;228:303-8. [ ] 11. Jequier S, Paltiel H, Lafortune M. Ureterovesical jets in infants and children: duplex and color Doppler US studies. Radiology. 1990;175:349-53. [ ] 12. Leung VY, Chu WC, Yeung CK, et al. Gender difference in achieving rate of maturity of the vesicoureteric junction. Pediatr Radiol. 2007;37:189-93. [ ] 13. Paterson A. Urinary tract infection: an update on imaging strategies. Eur Radiol. 2004;14 Suppl 4:L89-100. [ ] Received June 10, 2009. * Study developed at Instituto de Medicina Integral Prof. Fernando Figueira, Recife, PE, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554