Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 2 - Mar. / Apr. of 2009
Vol. 42 nº 2 - Mar. / Apr. of 2009
|
CASE REPORT
|
|
Acquired secondary Grynfeltt's hernia: a case report |
|
|
Autho(rs): Décio Valente Renck, Laura de Moraes Gomes, João Ivan Lopes Júnior |
|
|
Keywords: Lumbar hernia, Grynfeltt's hernia, Superior lumbar hernia |
|
|
Abstract:
IMaster, MD, Radiologist, Head at Center of Imaging Diagnosis of Hospital Santa Casa de Pelotas, Pelotas, RS, Brazil
INTRODUCTION Lumbar hernia is rare and is caused by a defect of the fibromuscular fascia of the posterior abdominal wall (2%)(1), with only 300 cases reported up to 1995(2). Basically, lumbar hernias occur in to sites: in the Grynfeltt's triangle (95%) and in the Petit's triangle(3,4). Frequently, lumbar hernias are unilateral and involve muscles, muscular fascia and aponeurosis(4). Lumbar hernias may be acquired or congenital (20%), and, typically, the latter manifest during the childhood(3,4), as an isolated phenomenon or in association with hereditary disorders such as syndrome of lumbar vertebral deficiency, meningocele and neurofibromatosis. Acquired hernia may be primary (50-55%), occurring in aged individuals, situation of increased intra-abdominal pressure, or excessive weight loss; and secondary (25-30%), caused by surgical procedures, blunt or open traumas(3-6). Other causes of acquired lumbar hernias include: penetrating wounds (75-80%), pregnancy, tuberculosis, Pott's disease, bone graft removal, poliomyelitis, obesity, debilitating diseases and extreme malnutrition(4). The present report describes a case of secondary, acquired Grynfeltt's hernia in a male, aged patient who, in the past, had been admitted with pleural effusion, being submitted to thoracentesis.
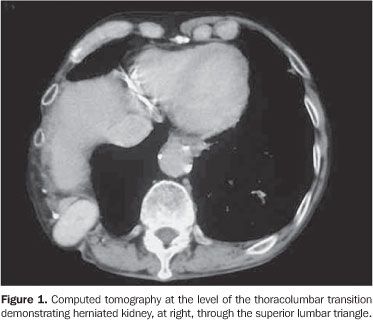
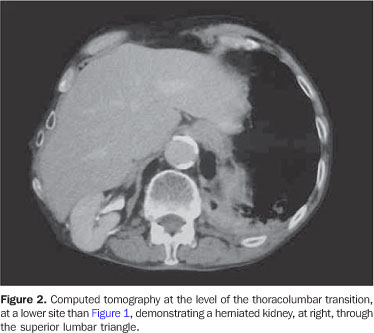
CASE REPORT A male, 79-year-old patient, smoker for 71 years and with history of alcoholism for 40 years, sought medical assistance complaining of asthenia, dyspnea on little exertion, cough and hemoptysis, without sudden weight loss. For 17 years, the patient had tuberculosis and underwent a procedure for placement of a drain because of pleural effusion. At clinical examination, the patient presented a good physical condition, with reddish and moist mucosas, unicteric, afebrile, tachypneic, with decreased vesicular murmur at right, with bilateral, diffuse snores and wheezes. Dorsal inspection retraction on the right paravertebral region could be visualized, with a bulge on the superior lumbar (Grynfeltt's) triangle, where a palpable mass could be observed. Initially, in the suspect of recidivating tuberculosis, a chest radiography was requested, and demonstrated a deformity of the lower right thoracic cage and decreased transparency in the base of the lung at right. Aiming at a higher diagnostic accuracy, contrast-enhanced chest helical computed tomography scan was performed, demonstrating deformity of the lateroposterior right thoracic cage, with pleural thickening and right kidney (functioning) herniation towards the posterior chest wall (Figures 1 and 2). Additionally, residual fibrotic striae, traction bronchiectasis in the lower lobes and centrilobular emphysema.
DISCUSSION Patients affected by lumbar hernia present a tumor in the lumbar region, with softened consistency, producing a sound at percussion, of reducible nature, but susceptible to become irreducible(4,7). Symptoms worsen under stress, and typically cause discomfort and pain in the anterior lower abdominal region suggesting bowels, kidneys, mesentery or omentum as hernia content. Hernia incarceration is observed in about 25% of cases, and strangulation in 10%(2,4,7). Lumbar hernias are predominantly left-sided and most frequently affect male individuals aged between 50 and 70 years(4). They are considered as infrequent nosological entities and are rarely diagnosed, being missed because of the lack of clinical symptoms(4,8). The diagnosis is based on the clinical history and physical examination of the patient. Differential diagnoses include soft part tumors, hematomas, abscesses and renal tumors. The diagnosis is confirmed by imaging studies(2-4,7). Generally, plain radiography present normal results; but computed tomography is useful for defining the abdominal wall and the hernial content, aiding in the differentiation between for example, retroperitoneal tumor and abdominal wall lipoma. Ultrasonography is a more accessible diagnostic method as compared with computed tomography and can be utilized in the suspect of lumbar hernia(4,7). The surgical approach is indicated, utilizing techniques aimed at getting the muscular masses of the Grynfeltt's triangle closer. Preferentially, the utilization of synthetic material should be avoided(4). A postoperative measures are common for all the types of hernias, and up to the present moment, recurrence of lumbar hernias has not been reported(4). In children, surgical repair should be performed between six and twelve months of age and, in adults, immediately after the diagnosis(4,5).
CONCLUSION Lumbar hernia is an infrequent phenomenon, and may be congenital or acquired. Diagnosis is based on clinical history, physical examination and imaging methods.
REFERENCES 1. Barden BE, Maull KI. Traumatic lumbar hernia. South Med J. 2000;93:1067-9. [ ] 2. Thor K. Lumbar hernia. Acta Chir Scand. 1985; 151:389-90. [ ] 3. Prieto-Díaz-Chávez E, Medina-Chavez JL, Prieto-Díaz S. Grynfeltt's hernia. Hernia. 2000;4:159-61. [ ] 4. Guillem P, Czarnecki E, Duval G, et al. Lumbar hernia: anatomical route assessed by computed tomography. Surg Radiol Anat. 2002;24:53-6. [ ] 5. Karmani S, Ember T, Davenport R. Congenital lumbar hernias: a case report. J Pediatr Surg. 2002;37:921-2. [ ] 6. Luna Bauza ME, Bello Fernández JF, Díaz Ramírez A. Hernia bilateral de Grynfeltt. Informe de un caso. Rev Med IMSS. 2003;41:339-43. [ ] 7. Skrekas G, Stafyla VK, Papalois VE. A Grynfeltt hernia: report of a case. Hérnia. 2005;9:188-91. [ ] 8. Alves Junior A, Maximiano L, Fujimura I, et al. Hérnia de Grynfeltt. Relato de caso e revisão da literatura. Rev Hosp Clin Fac Med São Paulo. 1995;50:111-4. [ ] Received May 25, 2007. * Study developed at the Center of Imaging Diagnosis of Hospital Santa Casa de Pelotas, Pelotas, RS, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554