Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 2 - Mar. / Apr. of 2009
Vol. 42 nº 2 - Mar. / Apr. of 2009
|
ORIGINAL ARTICLE
|
|
Evaluation of agreement between transvaginal ultrasonography and magnetic resonance imaging of the pelvis in deep endometriosis with emphasis on intestinal involvement |
|
|
Autho(rs): Maene Marcondes Cardoso, Heron Werner Junior, Plínio Tostes Berardo, Antônio Carlos Coutinho Junior, Marisa Nassar Aidar Domingues, Emerson Leandro Gasparetto, Romeu Côrtes Domingues |
|
|
Keywords: Deep endometriosis, Diagnosis, Transvaginal ultrasonography, Magnetic resonance imaging |
|
|
Abstract:
IMD, Ultrasonographist, Clínica de Diagnóstico Por Imagem (CDPI) and Hospital dos Servidores do Estado do Rio de Janeiro (HSE-RJ), Rio de Janeiro, RJ, Brazil
INTRODUCTION Endometriosis is defined as the presence of ectopic endometrial tissue, glands and stroma outside the uterine cavity. Estimated prevalence is about 10% of women of childbearing age(1). This is an enigmatic condition, so many theories have been raised about the pathogenesis of this disease. There are three types of endometriosis: superficial endometriosis, affecting basically the pelvic peritoneum; ovarian endometrioma; and deep endometriosis, penetrating the peritoneum more than 5 mm in depth and generally affecting the uterosacral ligament, vagina, bladder, ureter and bowel. Endometriosis may affect the bowel in 3% to 37% of cases, among them 90% involving the rectum the sigmoid colon or both. This site in particular represents one of the most complex problems in the treatment of the disease. Patients with endometriosis involving the rectum may present symptoms of abdominal pain, intestinal obstruction, blood in stools, diarrhea, and infertility. The decision about the treatment of these patients is extremely relevant considering that endometriosis is a benign disease and that intestinal surgery may lead to complications of difficult management(2). Clinical examination is crucial for determining the initial diagnostic suspicion of deep endometriosis and, as a result, the sequence of clinical studies to be requested(3). Imaging techniques have been utilized as an aid in the diagnosis of deep pelvic endometriosis, such as transvaginal and transrectal ultrasonography (US)(3,4), rectal endoscopic sonography(5), vaginosonography(6) and magnetic resonance imaging (MRI)(7). Despite the availability of these methods, the diagnosis of deep endometriosis still remains a challenge, corroborating the necessity of improvement of more accessible and less invasive techniques with good reproducibility. The present study was aimed at comparing the techniques of bidimensional transvaginal US and pelvic MRI in the diagnosis and prediction of the disease extent in cases of deep endometriosis, with emphasis on the rectum and rectosigmoid junction.
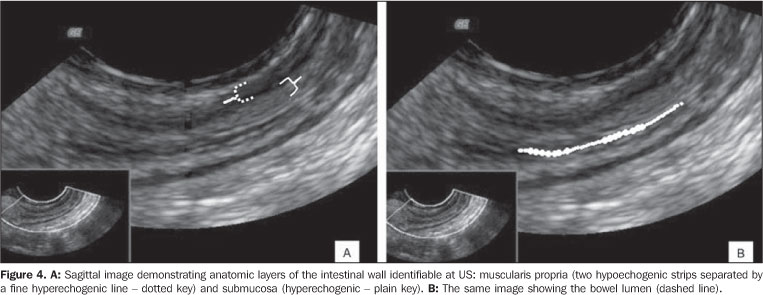
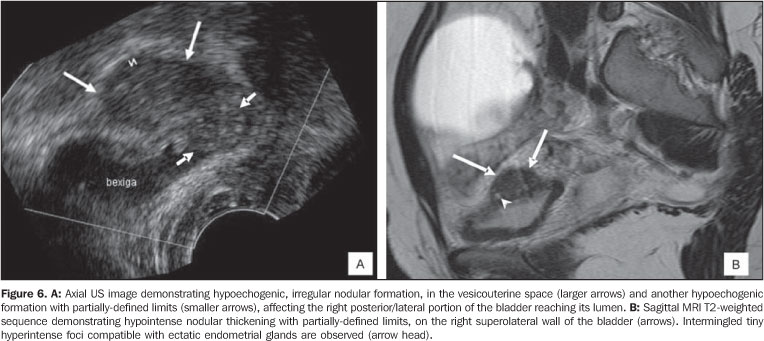
MATERIALS AND METHODS An observational study was developed in the Division of Endometriosis, Department of Gynecology at Hospital dos Servidores do Estado do Rio de Janeiro (HSE-RJ) and Clínica de Diagnóstico Por Imagem (CDPI), Rio de Janeiro, RJ, Brazil, in the period between November 2006 and January 2008. All of the patients included in this study underwent transvaginal US and pelvic MRI with a maximum interval of 60 days between examinations. The study protocol was approved by the Committee for Ethics in Research of HSE-RJ and all the patients signed a term of free and informed consent. The sample included 18 patients in the age range between 23 and 49 years (mean = 34.6 years) with clinical suspicion and gynecologic examination suggestive of deep endometriosis, presenting nodularities and/or thickening in the vaginal cul-de-sac, uterosacral ligaments and rectovaginal septum. Women in this group could be at any phase of their menstrual cycle, have a history of gynecologic/proctologic surgery, be undergoing or not hormonal therapy at the time of the proposed examinations. Exclusion criteria were: women aged under 18, pregnant women, immunocom-promised patients or presence of infecto-contagious disease or absolute contraindication to MRI. The sonographic evaluation was performed with a Voluson 730 (General Electric Healthcare; Wisconsin, USA) equipment with a 5-9 MHz transducer. The patients underwent pre-examination intestinal preparation with bisacodyl (10 mg) ingestion in the previous night and rectal fleet enema one hour before the examination. A urethral probe No.12 was utilized for introducing 40 ml US gel into the vaginal canal and 40 ml into the rectal canal to create an acoustic window between the transducer and the structures adjacent to the vaginal canal. The examination protocol included the routine analysis of the uterus and ovaries, bladder, besides the peritoneum overlying the vesicouterine space and cul-de-sac of Douglas, bowel (rectum, rectosigmoid junction and sigmoid colon), retrocervical region, uterosacral ligament, vagina and rectovaginal septum. The structures were schematized into anterior (vesicouterine space, bladder and ureter) and posterior (uterine cervix, uterosacral ligament, retrocervical region, vagina, sigmoid colon, rectosigmoid junction, rectum, rectovaginal septum, partial or complete posterior cul-de-sac obliteration). The transvaginal US images were analyzed by an experienced sonographist who defined the presence of deep or infiltrating endometriosis according to the following criteria: retrocervical endometriosis in the presence of thickening and/or hypoechogenic formations or heterogeneous formations with nodular or irregular hyperechogenic points found in this region, as well as in the uterosacral ligament and posterior cul-de-sac(8). Intestinal involvement was identified by the presence of hypoechogenic or heterogeneous images with hyperechogenic seemingly solid spots attached to the intestinal walls. As regards infiltration degree, the layers of intestinal walls were evaluated in detail: the serosa (a fine hypoechogenic line); the two layers (outer and inner) the muscularis propria (two hypoechogenic strips separated by a fine hyperechogenic line); the submucosa (hyperechogenic); the muscularis mucosa (hypoechogenic), and the interface between the lumen and the mucosa (hyperechogenic)(8). The involvement of the bladder was identified as hypoechogenic, mural, nodular images with irregular margins were found in this site, projecting into the vesicouterine space. Also, the presence of free fluid in the pelvis, adherences adjacent (particularly) to the uterus and ovaries, and posterior cul-de-sac obliteration was evaluated. MRI examinations were performed in a 1.5 T Magnetom Avanto unit (Siemens Medical Systems; Erlangen, Germany). The patients' preparation for examination included four to six-hour fasting, a partially-full bladder, intestinal preparation identical to the one utilized for US, administration of venous antispasmodic (20 mg scopolamine butylbromide) and intravaginal and rectal application of 40 ml US gel, besides venous puncture with a Jelco. The examination protocol included coronal, sagittal and axial T2-weighted sequences (TR = 3000 ms, TE = 120 ms, FOV = 240 mm, matrix = 256 × 512, 3-5 mm-thick slices), axial and sagittal T1-weighted sequences (TR = 480 ms, TE = 7.7 ms, FOV = 330 mm, matrix = 152 × 256 and 6 mm-thick slices), and axial T1-weighted sequences (TR = 591 ms, TE = 7.7 ms, FOV = 300 ms, matrix = 190 × 320 and 6 mm-thick slices). T1-weighted sequence was repeated in the three orthogonal planes following intravenous gadolinium contrast injection (0.2 ml/kg). MRI studies were analyzed by two experienced radiologists who defined the presence of deep endometriosis based on the presence of signal intensity alterations and morphological abnormalities varying according to the predominant endometriotic foci composition (hemorrhagic or fibrotic) and anatomic location of the lesions. The MRI findings varied according to type of lesion: small infiltrative implants, deep solid lesions, and visceral endometriosis involving the rectal and vesical walls(8). The analysis protocol included the investigation of deep endometriosis in the retrocervical region, vesicouterine space, uterosacral ligament, rectovaginal septum, posterior vaginal fornix and rectosigmoid wall. Retrocervical endometriosis was considered in the presence of nodular formation and/or hypointense thickening on T2-weighted sequences, with or without the presence of cysts (hematic or not) posteriorly to the cervix, adjacent to the vaginal dome(8). Intestinal involvement was considered to be present when retractable nodular formations were found attached to the bowel wall, with hyposignal on T2-weighted sequences, demonstrating delayed and variable gadolinium enhancement leading to fixation and/or angulation of the affected segment with "U" or "C" morphology. The longest axis of the lesion was measured in the sagittal plane. An evaluation was performed on the continuity of these lesions with the posterior uterine surface, causing partial or complete obliteration of the cul-de-sac of Douglas (adhesional process). The definition of bowel involvement included the identification of any lesion on the anterior rectal wall, rectosigmoid transition, sigmoid colon, cecum and small bowel loops individualized in the pelvis(8). Vesicouterine space involvement was demonstrated through nodular formations or mass with low signal intensity on T2-weighted sequences, similarly to the pelvic musculature, generally attached to the anterior uterine surface forming an obtuse angle with the bladder wall, including cysts or not (hematic or not). In infiltrating lesions there was invasion of the bladder wall and ureter, replacing the hypointense signal on T2-weighted sequences typical of the muscular layer or protruding into the lumen, invading the mucosa. The presence of hypointense signal on T2-weighted sequences obliterating the fat of the vesicouterine and ureteral septum was considered as infiltrating disease (Figures 4B and 6A,B,C). The observers had no access to results previously to US and MRI examinations. The agreement between MRI and transvaginal US was analyzed through the Cohen's kappa coefficient, also calculating the percentage of cases where intermethod agreement was observed. Possible kappa values and respective interpretations are shown on Table 1. The rate of agreement was calculated through the formula: (number of cases with intermethod agreement/total number of cases) × 100(9).
In an attempt to compare the US and MRI capability of detecting lesions suggestive of endometriosis, a summation of scores was calculated for each patient (0 = no lesion, 1 = lesion detected), representing the total number of lesions detected for each compartment (posterior and anterior) by MRI and/or US. Mean and standard deviation of this summation of scores were calculated for each diagnostic method taking the compartment involved into account. The Wilcoxon test was applied to both value sets to evaluate the presence of statistically significant differences at the level of 5% between MRI and US in the detection of deep endometriosis according to pelvic compartments.
RESULTS Alterations identified at MRI and US, as well as kappa indices and rates of intermethod agreement are shown on Tables 2 and 3.
US detected a total of 40 lesions, while MRI detected 53 pelvic lesions. Comparison between US and MRI in the detection of lesions in anterior and posterior compartments utilizing the above described summation of scores, has demonstrated no statistically significant difference (respectively p > 0.19 and p > 0.14) (Table 4) (Figures 1 to 4).
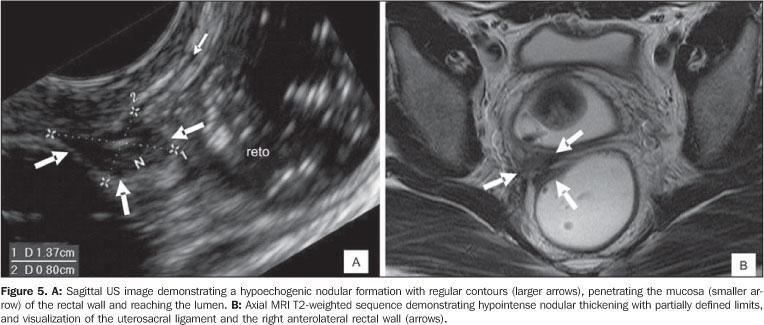
Considering specifically intestinal lesions in the rectosigmoid junction, MRI has detected one (5.6%) and US four (22.2%). In cases of rectal lesions, US has indicated eight (44.4%) and MRI seven (38.9%) (Figures 5 and 6). Only in one patient MRI has demonstrated a lesion in the sigmoid colon, which has not been detected in any case by US. In 90% of patients whose US image suggested intestinal lesion the degree of infiltration of intestinal wall layers could be determined.
DISCUSSION Deep endometriosis is a specific entity and is histologically defined when the ectopic focus is more than 5 mm deep in the peritoneum, generally involving the uterosacral ligaments, bowel, rectovaginal septum and the urinary tract(10). Chapron et al.(11) have suggested that lesions in deep endometriosis are most frequently found posteriorly on the left side of the pelvis, reinforcing the regurgitation theory for explaining the pathogenesis of the disease, added to the gravitational action and to the left hemipelvis anatomy. The previous knowledge of the intestinal lesion extent allows the selection of the most appropriate surgical technique, besides the preparation of the patient as for the necessity of surgery(12). In these cases, surgical correction may range from a partial resection of the rectal and posterior vaginal walls to en-block resection of the cul-de-sac of Douglas, including the posterior vaginal fornix, and part of the rectosigmoid colon with intestinal anastomosis(2,13). Extensive sutures in cases of incision of more than half of the intestinal wall circumference imply risks such as intestinal lumen stenosis(2). Consequently, the relevance of detailed information on these lesions through imaging diagnosis methods has encouraged the development of studies on this matter. Abrão et al.(2) have proposed that the involvement of the intestinal wall circumference, besides the number of lesions and degree of intestinal walls infiltration, should be utilized as cut-off point in the definition of the type of surgical intervention. Transvaginal US is the most sensitive imaging method in the diagnosis of pelvic endometriosis and is the method of choice for differentiating endometriomas from other ovarian cysts. In the last years, some studies have emphasized the utilization of this method to identify deep endometriosis with promising results in relation to the capacity of assessment and good tolerability of the method(8). Notwithstanding their dependence on the lesion localization and operator experience, both MRI and transrectal/transvaginal US have been considered as accurate methods in the diagnosis of deep endometriosis. Among the imaging techniques, MRI remains as a reference method in the diagnosis of deep endometriosis(14), because of its multiplanar capacity and excellent tissue characterization, MRI can also evaluate locations otherwise inaccessible by laparoscopy, as well as the extent of subperitoneal lesions and those intermingled with adherences(15). The present study compared MRI and US findings in 18 patients with clinical suspicion for deep endometriosis. Intermethod agreement was observed in 17 patients, particularly when lesions localized in the sigmoid colon were evaluated. Intermethod agreement was not observed in six patients for the uterosacral ligaments and retrocervical regions (better evaluated by MRI), and in five patients for the rectosigmoid junction and rectum (better evaluated by transvaginal US). Because of the small size of the sample, kappa coefficient values are a little distorted. Most of the present study results are in agreement with previous studies: lesions in the posterior compartment such as rectovaginal septum and vagina which were not seen by US in this study corroborate the findings reported in the literature on low diagnostic sensitivity, respectively 28.6% and 29.4%(4). Agreement with findings in the literature was also observed for lesions in the rectalsigmoid junction, with sensitivity and specificity of respectively 87.2% and 96.8%(4), and 98% and 100%(13). Abrão et al.(8) have reported their best results with a protocol including previous intestinal preparation which was also utilized in the present study. In spite of not being the main focus of the present study, anterior compartment analysis demonstrated that the sonographic identification of lesions in the bladder presented agreement with the literature (71.4% sensitivity)(4), with false-negative results being attributed to small-sized implants (< 15 mm)(4). US has not been considered as a good method for the diagnosis of ureteral endometriotic lesions(16). Generally the main limitations of the sonographic technique are: partial visualization of the pelvis and subperitoneal space, complicating the evaluation in the whole extent of the region, besides the dependence of the method on the operator experience and efficiency. In summary, this study presented limitations inherent to the low number of patients evaluated, and the absence of correlation with histological analyses, particularly for sonographic findings concerning size and infiltration of intestinal wall layers by lesions suggestive of endometriosis. Also, because of the lack of histopathological correlation, one cannot say that the lesions found at US and MRI were the same. It is important to observe that these limitations should be overcome to improve the learning curve on this matter. Based on the present analysis, it may be concluded that the intermethod agreement was poor in the rectosigmoid junction and rectum, with US detecting a higher number of lesions in these sites, although it has detected a lower number of lesions in the whole pelvis. In the global comparative analysis between US and MRI in the detection of lesions, no statistically significant difference was observed. Additionally, it is important to note that low cost, good tolerability and wide availability of ultrasonography allow the diagnosis of one of the most severe presentations of the disease in a population for which more sophisticated diagnostic resources such as MRI still remain inaccessible.
REFERENCES 1. Safe Jr JV, Safe GMS. Endometriose. In: Crispi CP, editor. Tratado de videoendoscopia ginecológica. 2ª ed. Rio de Janeiro: Atheneu; 2007. p. 294-328. [ ] 2. Abrão MS, Podgaec S, Dias JA Jr, et al. Endometriosis lesions that compromise the rectum deeper than the inner muscularis layer have more than 40% of the circumference of the rectum affected by the disease. J Minim Invasive Gynecol. 2008;15:280-5. [ ] 3. Guerriero S, Ajossa S, Gerada M, et al. Diagnostic value of transvaginal 'tenderness-guided' ultrasonography for the prediction of location of deep endometriosis. Hum Reprod. 2008;23: 2452-7. [ ] 4. Bazot M, Thomassin I, Hourani R, et al. Diagnostic accuracy of transvaginal sonography for deep pelvic endometriosis. Ultrasound Obstet Gynecol. 2004;24:180-5. [ ] 5. Bazot M, Bornier C, Dubernard G, et al. Accuracy of magnetic resonance imaging and rectal endoscopic sonography for the prediction of location of deep pelvic endometriosis. Hum Reprod. 2007; 22:1457-63. [ ] 6. Dessole S, Farina M, Rubattu G, et al. Sonovagi-nography is a new technique for assessing recto-vaginal endometriosis. Fertil Steril. 2003;79: 1023-7. [ ] 7. Koga K, Osuga Y, Yano T, et al. Characteristic images of deeply infiltrating rectosigmoid endo-metriosis on transvaginal and transrectal ultrasonography. Hum Reprod. 2003;18:1328-33. [ ] 8. Abrão MS, Gonçalves MOC, Dias JA Jr, et al. Comparison between clinical examination, transvaginal sonography and magnetic resonance imaging for the diagnosis of deep endometriosis. Hum Reprod. 2007;22:3092-7. [ ] 9. Fleiss JL. Statistical methods for rates and proportions. 2nd ed. New York: John Wiley; 1981. [ ] 10. Brosens J, Timmerman D, Starzinski-Powitz A, et al. Noninvasive diagnosis of endometriosis: the role of imaging and markers. Obstet Gynecol Clin North Am. 2003;30:95-114. [ ] 11. Chapron C, Chopin N, Borghese B, et al. Deeply infiltrating endometriosis: pathogenetic implications of the anatomical distribution. Hum Reprod. 2006;21:1839-45. [ ] 12. Fedele L, Bianchi S, Zanconato G, et al. Long term follow-up after conservative surgery for rectova-ginal endometriosis. Am J Obstet Gynecol. 2004; 190:1020-4. [ ] 13. Valenzano Menada M, Remorgida V, Abbamonte LH, et al. Does transvaginal ultrasonography combined with water-contrast in the rectum aid in the diagnosis of rectovaginal endometriosis infiltrating the bowel? Human Reprod. 2008;23: 1069-75. [ ] 14. Bazot M, Daraï E. Sonography and MR imaging for the assessment of deep pelvic endometriosis. J Minim Invasive Gynecol. 2005;12:178-85. [ ] 15. Coutinho Jr AC, Lima CMAO, Coutinho EPD, et al. Ressonância magnética na endometriose pélvica profunda: ensaio iconográfico. Radiol Bras. 2008;41:129-34. [ ] 16. Balleyguier C, Roupret M, Nguyen T, et al. Ureteral endometriosis: the role of magnetic resonance imaging. J Am Assoc Gynecol Laparosc. 2004;11:530-6. [ ] Received September 3, 2008. * Study developed at Hospital dos Servidores do Estado do Rio de Janeiro (HSE-RJ) and Clínica de Diagnóstico Por Imagem (CDPI), Rio de Janeiro, RJ, Brazil. |
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554