Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 2 - Mar. / Apr. of 2009
Vol. 42 nº 2 - Mar. / Apr. of 2009
|
ORIGINAL ARTICLE
|
|
3D conformal external beam radiation therapy for prostate carcinoma: an experiment of Instituto do Radium de Campinas with 285 patients |
|
|
Autho(rs): Ricardo Akiyoshi Nakamura, Carlos Roberto Monti, Felipe Amstalden Trevisan, Alexandre Arthur Jacinto |
|
|
Keywords: Prostate, Cancer, Radiotherapy, Toxicity, Prognostic factors |
|
|
Abstract:
IMD, Radiotherapist at Hospital de Caridade Dr. Astrogildo de Azevedo and Universidade Federal de Santa Maria (UFSM), Santa Maria, RS, Brazil
INTRODUCTION Prostate cancer is the most frequent forma of cancer in men, except for non-melanoma skin cancer, with estimation of 49,530 new cases in 2008 in Brazil, corresponding to 52 new cases/100,000 men(1). The disease can be approached in a number of ways such as surgery, external beam radiation therapy, brachytherapy with iodine seeds, high-dose rate brachytherapy(2), androgen suppression therapy, prostate-specific antigen (PSA) monitoring alone, and cryotherapy. However, only surgery, external beam radiotherapy, brachytherapy and cryotherapy, or an association of these therapeutic modalities can provide a cure for these patients. Three-dimensional conformal radiation therapy (3DCRT), a technique of external beam radiotherapy, utilizes high technology with powerful computers and complex softwares, allowing a more accurate localization of the radiotherapy target and organs at risk, with the delivery of high doses to the target volume and better control over the radiation dose in healthy structures. The high radiation dose for prostate cancer has allowed a better biochemical control in prospective randomized studies although without resulting in increased overall survival(3,4) and with an increase in toxicity(5). However the high doses released with 3DCRT generate lower toxicity as compared with conventional radiotherapy with conventional radiation doses(6). The present study was aimed at reporting the outcomes of the treatment for localized prostate cancer with 3DCRT performed in an institution were more than 1,000 patients have already been treated up to the present moment, and evaluating prognostic factors for the management of the disease and toxicity of the therapy.
MATERIALS AND METHODS In the period between July 1997 and January 2002, 285 consecutive patients with localized prostate adenocarcinoma diagnosed by means of transrectal biopsy were submitted to 3DCRT for curative purposes in a single institution, and were retrospectively evaluated. The median follow-up was of 53.6 months (3.6-95.3 months). All the patients were staged in compliance with the staging system of the American Joint Committee on Cancer (2002). Information on the testosterone levels at the beginning of the treatment was not available. All the patients signed a term of free and informed consent before being submitted to the treatment. Other characteristics of the patients are shown on Table 1.
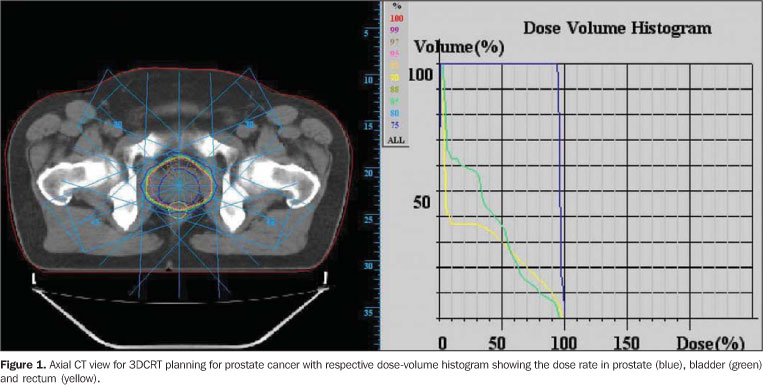
Treatment characteristics Concomitant and/or adjuvant, neoadjuvant androgen suppression and type of suppressor drug were defined by decision of the urologist and/or radiotherapist. Simulation was performed with the patient in dorsal decubitus in a helical CT equipment with venous and urethral contrast-enhancement and 5 mm-thick slices. The Med-Crane software was utilized for images acquisition. The therapy targets were delineated on the tomographic slices as follows: a) prostate - whole volume delineation (gross tumor volume - GTV); b) seminal vesicles - whole extent delineation (GTV, when affected; clinical target volume - CTV in subclinical disease); c) drainage - lymph nodes of internal and external iliac vessels from the caudal region of the sacroiliac joint, and lymph nodes of the obturator vessels, excluding the lateral perirectal lymph nodes (CTV in high-risk patients). Margins for target displacement and positioning errors measured 10 mm for all the dimensions and 3 mm posteriorly (PTV). Organs at risk were delineated as follows: a) bladder - whole volume by the outer muscular layer; b) rectum - whole volume and contents by the outer layer, from the rectoanal transition to the rectosigmoid transition. Energies of 6 or 15 MV and five radiation fields were utilized. The radiotherapy treatment was divided into phases, as follows: in the first phase, pelvis, seminal vesicles and prostate were irradiated (PTV1); following, the treatment volume was restricted to the seminal vesicles and prostate (PTV2); and, finally, the treatment field covered only the prostate with respective margins (PTV3). In the absence of pelvic irradiation, the treatment was comprised of two phases, irradiation of seminal vesicles and prostate (PTV1), and following, only the prostate (PTV2). Restriction of doses in healthy tissues corresponded to: a) rectum: 50% < 50 Gy, 25% < 70 Gy; b) bladder: 50% < 50 Gy, 30% < 70 Gy; c) femoral heads: < 55Gy; the prescription dose corresponded to 95%. Figure 1 represents the dose and volume histogram, and an axial CT view in a 3DCRT planning for prostate cancer. Transference of the planning data to the linear accelerator was the next step, the treatment being performed with a dose of 180 cGy/day five times a week. The patients were evaluated on a weekly basis or more frequently as necessary. Weekly check-films were utilized for quality control. Other treatment characteristics are shown on Table 1. Patients follow-up After the 3DCRT, the patients were followed-up with serial total PSA between three and six months, and image studies were requested in case of specific complaints. By the time of the analysis, data on the management of the disease and toxicity of the treatment were updated through phone conversations with the patients. Toxicity Late toxicity was evaluated for the rectum and bladder and rated according to the Common Terminology Criteria for Adverse Effects version 3(7). Biochemical failure The presence of biochemical failure was considered after three consecutive increases in total PSA levels(8) or introduction of therapy with androgen suppression for any reason. Statistical analysis The patients were evaluated as a single group for management of the disease and late toxicity, and as three different groups for management of the disease according to the initial total PSA levels, Gleason score and clinical T-stage, as follows: low-risk group including patients with initial total PSA < 10 ng/ml, Gleason score < 6 and stage > T2a; intermediate risk group with initial total PSA > 10 and < 20 ng/ml or Gleason score = 7 or stage T2b-T2c; and the high-risk group with initial total PSA > 20 and/or Gleason score > 8 and/or stage T3, or two or more characteristics of the intermediate risk group. The patients with late urinary or rectal toxicity may have had one or more types of toxicity, and the data and degree considered for the survival calculation were respectively the most recent and the highest. Death for prostate cancer was defined as death of the patient with distant metastasis. Association between categorical variables on contingency tables was evaluated by means of the chi-squared test and, in cases where at least one expected frequency was < 5 on 2 × 2 tables, the exact Fisher test was adopted. The significance level of 5% was considered for all the tests. Overall survival was defined as the interval between date of the treatment beginning and the date of death or last information for censured observations. The period of disease recurrence of biochemical failure was measured from the beginning of the 3DCRT to the date of recurrence. Overall survival and recurrence-free survival were estimated by the Kaplan-Meyer test, and the logrank test was applied to compare survival curves with 95% confidence interval. The gross and adjusted relative risk of death was estimated by the Cox regression model. The whole statistical analysis was performed with the Stata 7 software package (StataCorp.; Texas, USA).
RESULTS Actuarial overall survival Actuarial overall five-year and seven-year survival rates were, respectively, 85.1% and 77.0%. Age > 65 years (p = 0.0458) and absence of seminal vesicles irradiation (p = 0.0125) resulted in lower rates of overall survival (Table 2). Association between radiation dose in seminal vesicles and increase in overall survival could not be observed. Other variables analyzed (see Table 2) did not influence the actuarial overall survival. Actuarial cause-specific survival The five-year and seven-year actuarial cause-specific survival rates were respectively 97% and 94.5%. Gleason score (p = 0.0179), percentage of positive fragments (p = 0.0222), clinical T-stage (p = 0.0006), biochemical recurrence (p < 0.0001) and pre-3DCRT transurethral resection (p = 0.0206) constituted prognostic factors for death for prostate cancer. The analysis of risk groups demonstrated a tendency towards statistical significance (p = 0.0677). However, as the risk groups were separately analyzed, a same p value was found for risk groups 1 and 2 (p = 0.2403) and the group 1 demonstrated longer cause-specific survival than group 3 (p = 0.0327). Other characteristics analyzed are shown on Table 2. Actuarial metastasis-free survival The five-year and seven-year actuarial metastasis-free survival rates were respectively 94.2% and 93.1%. Seventeen patients presented distant metastasis. Age < 65 years (p = 0.0220), Gleason score (p = 0.0005), clinical T-stage (p = 0.0041), risk group (p = 0.0033), biochemical recurrence (p < 0.0001), pré-3DCRT transurethral resection (p = 0.0039) and a period > 5 months between diagnosis and introduction of 3DCRT (p = 0.0016) constituted prognostic factors for the development of distant metastasis (Table 3). Actuarial biochemical recurrence-free survival Actuarial five-year and seven-year biochemical recurrence-free survival rates were respectively 75.8% and 64.0%. Sixty-nine patients presented biochemical recurrence (24.21%). Gleason score (p = 0.0004), percentage of positive fragments > 50% (p = 0.0211), initial total PSA (p < 0.0001), clinical T-stage (p = 0.0204) and risk group (p < 0.0001) implied higher rates of biochemical failure in the univariate analysis (Table 3). In the multivariate analysis, pre-3DCRT initial total PSA and Gleason scores constituted independent prognostic factors (p < 0.0001 and p = 0.0011, respectively) (Table 4).
Pelvic 3DCRT Patients submitted to pelvic radiotherapy presented lower actuarial biochemical recurrence-free and metastasis-free survivals. However, these patients had more aggressive tumors, allowing a sampling error in the statistical analysis. Low-risk group Actuarial seven-year overall and biochemical recurrence-free survival rates for patients in the low-risk group were, respectively, 87.2% and 87.8%. Prognostic factors implying lower survival rates for this group of patients were not identified. Only a tendency to longer actuarial overall survival with doses > 76 Gy in the prostate (p = 0.0524) was observed. In account of the low incidence of deaths for prostate cancer and distant metastasis, actuarial cause-specific and distant metastasis-free survival rates could not be evaluated for this group. Intermediate-risk group Actuarial seven-year overall and biochemical recurrence-free survival rates were, respectively 78.9% and 59.2%. Irradiation of seminal vesicles resulted in longer actuarial overall and biochemical recurrence-free survival (p = 0.0034 and p = 0.0301, respectively). No association was found between the other variables. Because of the low incidence of deaths for prostate cancer and distant metastasis, actuarial cause-specific and distant metastasis-free survival rates could not be evaluated for this group. High-risk group Actuarial seven-year overall and biochemical recurrence-free survival rates were respectively 67.1% and 49.0%. Neoadjuvant and concomitant androgen suppression resulted in higher actuarial overall survival rates (p = 0.0217 and p = 0.0238, respectively), and irradiation of seminal vesicles resulted in higher actuarial biochemical recurrence-free survival rates (p = 0.0040). Other variables were not statistically significant. Because of the low incidence of deaths for prostate cancer and distant metastasis, actuarial cause-specific and distant metastasis-free survival rates could not be evaluated for this group. Late rectal toxicity The rate of actuarial seven-year survival free of late rectal toxicity (grade 2-3) was 96.38%. Three patients presented late rectal toxicity grade 2 and seven, grade 3 (Table 5). Associated prognostic factors could not be identified because of the low number of patients with late rectal toxicity.
Late urinary toxicity The rate of actuarial seven-year survival free of late urinary toxicity (grade 2-3) was 89.97%. Seven patients presented late urinary toxicity grade 2, and 15 grade 3 (Table 5). Pre-3DCRT transurethral resection and doses > 70 Gy in 30% of the bladder volume implied a higher late urinary toxicity grade 2 and 3 (respectively (p = 0.0002 and p = 0.0264). Other variables were not statistically significant.
DISCUSSION Treatment characteristics associated with the therapy results In low-risk patients with clinical T1 and T2a stages, long term outcome from conventional external beam radiotherapy have been similar to the ones from radical prostatectomy(9,10). However, in patients with locally advanced disease, the local management of the primary tumor with conventional external beam radiotherapy is unsatisfactory, with 30% to 40% local recurrence in ten years and, after 10 and 15 years, only 35% to 45% and 18% to 27% respectively are alive(10). Retrospective studies have associated local management with radiation dose in prostate adenocarcinoma(10,11). However, the delivery of doses > 70 Gy with the technique of conventional radiotherapy has implied severe complications (grades 3 and 4) in 3.5% to 6.9% of cases(12). With the technological development, the association of computed tomography with linear accelerator became feasible by means of complex software packages. This association has allowed an extremely reliable visualization of the therapeutic target as well as of adjacent healthy structures, and the estimation of the radiation dose in the target volume and structures at risk. As a result, since the beginning of the nineties, dose scaling protocols have been developed and, in cases of prostate cancer, a higher biochemical control with acceptable late toxicity has been achieved(3,4). In the present series, the actuarial five-year biochemical recurrence-free survival for low, intermediate and high-risk patients was, respectively, 91.40%, 73.29% and 64.25%, similarly to the results from 3D radiotherapy(13) and radical prostatectomy(8). Already published series with dose scaling(3,4,13) report a higher biochemical control with higher radiation doses, although without increasing the overall survival. However, the follow-up of these patients is still relatively short, and a longer follow-up may demonstrate benefits in terms of overall survival. In the meantime a decrease in biochemical failure may result in measurable benefits to the patients, with longer actuarial cause-specific and metastasis-free survival as reported by the present series, besides reducing the necessity of androgen suppression in the biochemical failure. Gleason score, clinical T-stage and initial total PSA level can predict the risk for seminal vesicles involvement(14) that, depending on the risk level, must be treated. However, irradiation of seminal vesicles may drastically increase the volume of healthy tissues irradiated and, consequently increase the risk for late toxicity. In the present study, irradiation of seminal vesicles resulted in longer actuarial overall and biochemical recurrence-free survival in patients of the intermediate risk group, and increased the biochemical recurrence-free survival in patients of the high-risk group, without increasing the toxicity. Several prospective randomized studies associating androgen suppression with radiotherapy have been developed, demonstrating benefits in terms of overall survival, disease-free survival, cause-specific survival, biochemical recurrence-free survival, distant metastasis-free survival, and local management(15,16). In the present series, the utilization of neoadjuvant and concomitant androgen suppression resulted in longer overall survival in high-risk patients. Patients at intermediate and low risks did not benefit from the procedure. The number of patients submitted to adjuvant androgen suppression was small and did not allow statistical analysis. In the present study, patients submitted to pelvic radiotherapy presented shorter actuarial biochemical recurrence-free and distant metastasis-free survival. However, patients submitted to this treatment presented more aggressive tumor characteristics, causing distortion in findings confirmed in the cases where statistically significant was not observed among patients of a same risk group submitted or not to pelvic radiotherapy. Patients' characteristics associated with treatment results The relevance of several tumor-related prognostic factors, particularly Gleason score, clinical T-stage and initial total PSA level, has been identified in the literature(14). In the present series, Gleason score, clinical T-stage and initial total PSA level constituted prognostic factor for cause-specific and biochemical recurrence-free survival. For metastasis-free survival, Gleason score and clinical T-stage were significant; initial total PSA level was marginally significant (p = 0.0545). The division into risk groups associating initial total PSA level, Gleason score and clinical T-stage in the present series was significant for biochemical recurrence-free and distant metastasis-free survival, and marginally positive for cause-specific survival. However, as the risk groups are separately evaluated, a same p value was found for risk groups 1 and 2 and the group 1 demonstrated longer cause-specific survival than group 3. In the literature, the role of pre-3DCRT transurethral resection in the management of prostate cancer is controversial(17,18). In the present series, pre-3DCRT transurethral resection resulted in shorter cause-specific and metastasis-free survival, suggesting that the procedure may reduce the 3DCRT effectiveness. After the diagnosis of prostate cancer, patients who had to wait for more than three months to have the 3DCRT started presented a tendency to a shorter metastasis-free survival (p = 0.0763). However, when the wait was extended for more than five months from the diagnosis, the distant metastasis-free survival was significantly longer (p = 0.0016), suggesting that prostate cancer should be treated in less than five months after the diagnosis. Probably, patients with > 65 years of age present less aggressive tumors, considering that they presented longer metastasis-free survival than those with < 65 years of age, suggesting that patients with > 65 years can benefit from less debilitating treatments. In the present series, patients with < 50% of positive fragments presented longer cause-specific and biochemical recurrence-free survival and a tendency to longer metastasis-free survival (p = 0.0524), suggesting that this is significant prognostic factor to be taken into consideration in the treatment individualization, as reported in the literature(19). Late toxicity Three-dimensional conformal radiation therapy for the treatment of prostate cancer reduces late effects grade > 3 as compared with conventional 2D radiation therapy. The rate of late toxicity grade > 3 for 78 Gy to the PTV in the study RTOG 94-06-group 1 (six cases) was significantly lower in relation to the historical expected 18.2 control cases (RTOG 7506 and RTOG 7706) (p = 0.0042)(6). In several studies, late rectal toxicity has been strongly associated with the rectal volume irradiated with a determined radiation dose(20). It is recognized that there is not a single point of radiation dose in the volume of a healthy organ resulting in late rectal toxicity, but there is a continuum of relations between dose and volume. Studies developed at the M.D. Anderson Cancer Center associating absolute radiation dose with percentage of rectal volume have been of aid to the clinical practice for adding safety to the radiotherapy treatment. In a retrospective study including 163 patients submitted to 3DCRT at the M.D. Anderson Cancer Center, Huang et al.(20) have suggested that doses of 60 Gy, 70 Gy, 75.6 Gy and 78 Gy should be restricted to respectively 40%, 25%, 15% and 5% of the rectal volume. In the present study, probably because of the small number of patients with grade > 2 late rectal toxicity, the authors could not observe any relation between this variable and the radiation dose to a determined rectal volume or its association with any other variable. Liu et al.(21) have evaluated 1,192 patients submitted to radiotherapy and observed that coexisting genitourinary disease, transurethral resection of the prostate or transurethral resection of vesical tumor and the presence of acute urinary toxicity during radiotherapy were significant factors for late urinary toxicity grade 3. In the present series, doses > 70 Gy to 30% of bladder volume implied a higher late urinary toxicity (grade 2-3). Patients submitted to pre-3DCRT transurethral resection of the prostate presented higher late urinary toxicity. However, the finding may result from a sampling error probably because of the selection of patients with a higher propensity to urinary toxicity, considering the previous necessity of transurethral resection of the prostate.
CONCLUSIONS The firstly reported Brazilian experiment with 3DCRT utilizing high radiation doses has shown the effectiveness of this method in the management of patients with prostate cancer and low late rectal and urinary toxicity, as reported in the literature. Despite the retrospective character and the relatively limited number of patients, the present study suggests recommendations for the clinical practice. The irradiation of seminal vesicles may be beneficial for intermediate-risk patients, as the study suggests, considering that there was an increase in the overall and biochemical recurrence-free survival. The utilization of neoadjuvant and concomitant androgen suppression in high-risk patients may extend the actuarial overall survival and irradiation of seminal vesicles may result in longer biochemical recurrence-free survival. Pre-3DCRT transurethral resection of the prostate may impair the management of the tumor and increase the late urinary toxicity (grade 2-3). The data presented herein suggest that the restriction of the radiation dose < 70 Gy in 30% of the bladder volume may reduce grade 2-3 late urinary toxicity.
REFERENCES 1. Instituto Nacional de Câncer. Estimativa 2008: incidência de câncer no Brasil. Rio de Janeiro: INCA; 2007. p. 33-4. [ ] 2. Esteves SCB, Oliveira ACZ, Cardoso H, et al. Braquiterapia de alta taxa de dose no tratamento do carcinoma da próstata: análise da toxicidade aguda e do comportamento bioquímico. Radiol Bras. 2006;39:127-30. [ ] 3. Pollack A, Zagars GK, Starkschall G, et al. Prostate cancer radiation dose response: results of the M. D. Anderson phase III randomized trial. Int J Radiat Oncol Biol Phys. 2002;53:1097-105. [ ] 4. Zietman AL, DeSilvio ML, Slater JD, et al. Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. JAMA. 2005;294:1233-9. [ ] 5. Kuban D, Pollack A, Huang E, et al. Hazards of dose escalation in prostate cancer radiotherapy. Int J Radiat Oncol Biol Phys. 2003;57:1260-8. [ ] 6. Michalski JM, Winter K, Purdy JA, et al. Toxicity after three-dimensional radiotherapy for prostate cancer on RTOG 9406 dose level V. Int J Radiat Oncol Biol Phys. 2005;62:706-13. [ ] 7. Common Terminology Criteria for Adverse Effects version 3. [cited 2005Jun 9]. Available from: http://ctep.cancer.gov/forms/CTCAEv3.pdf [ ] 8. Consensus statement: guidelines for PSA following radiation therapy. American Society for Therapeutic Radiology and Oncology Consensus Panel. Int J Radiat Oncol Biol Phys. 1997;37:1035-41. [ ] 9. Hull GW, Rabbani F, Abbas F, et al. Cancer control with radical prostatectomy alone in 1,000 consecutive patients. J Urol. 2002;167(2 Pt 1): 528-34. [ ] 10. Hanks GE, Asbell S, Krall JM, et al. Outcome for lymph node dissection negative T-1b, T-2 (A-2, B) prostate cancer treated with external beam radiation therapy in RTOG 77-06. Int J Radiat Oncol Biol Phys. 1991;21:1099-103. [ ] 11. Zagars GK, Johnson DE, von Eschenbach AC, et al. Adjuvant estrogen following radiation therapy for stage C adenocarcinoma of the prostate: long-term results of a prospective randomized study. Int J Radiat Oncol Biol Phys. 1988;14:1085-91. [ ] 12. Leibel SA, Hanks GE, Kramer S. Patterns of care outcome studies: results of the national practice in adenocarcinoma of the prostate. Int J Radiat Oncol Biol Phys. 1984;10:401-9. [ ] 13. Zelefsky MJ, Fuks Z, Hunt M, et al. High dose radiation delivered by intensity modulated conformal radiotherapy improves the outcome of localized prostate cancer. J Urol. 2001;166:876-81. [ ] 14. Partin AW, Kattan MW, Subong EN, et al. Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional update. JAMA. 1997;277:1445-51. [ ] 15. Bolla M, Collette L, Blank L, et al. Long-term results with immediate androgen suppression and external irradiation in patients with locally advanced prostate cancer (an EORTC study): a phase III randomised trial. Lancet. 2002;360: 103-6. [ ] 16. Pilepich MV, Winter K, Lawton CA, et al. Androgen suppression adjuvant to definitive radiotherapy in prostate carcinoma - long-term results of phase III RTOG 85-31. Int J Radiat Oncol Biol Phys. 2005;61:1285-90. [ ] 17. Kupelian PA, Elshaikh M, Reddy CA, et al. Comparison of the efficacy of local therapies for localized prostate cancer in the prostate-specific antigen era: a large single-institution experience with radical prostatectomy and external-beam radiotherapy. J Clin Oncol. 2002;20:3376-85. [ ] 18. Zagars GK, Pollack A, Kavadi VS, et al. Prostate-specific antigen and radiation therapy for clinically localized prostate cancer. Int J Radiat Oncol Biol Phys. 1995;32:293-306. [ ] 19. D'Amico AV, Renshaw AA, Cote K, et al. Impact of the percentage of positive prostate cores on prostate cancer-specific mortality for patients with low or favorable intermediate-risk disease. J Clin Oncol. 2004;22:3726-32. [ ] 20. Huang EH, Pollack A, Levy L, et al. Late rectal toxicity: dose-volume effects of conformal radiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys. 2002;54:1314-21. [ ] 21. Liu M, Pickles T, Agranovich A, et al. Impact of neoadjuvant androgen ablation and other factors on late toxicity after external beam prostate radiotherapy. Int J Radiat Oncol Biol Phys. 2004;58: 59-67. [ ] Received November 11, 2007. * Study developed at Instituto do Radium de Campinas (IRC), Campinas, SP, Brazil. |
|

{kind=link}
{kind=link}
{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554