Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 42 nº 2 - Mar. / Apr. of 2009
Vol. 42 nº 2 - Mar. / Apr. of 2009
|
WHICH IS YOUR DIAGNOSIS?
|
|
Which is your diagnosis? |
|
|
Autho(rs): Fábio Abilio Gomes de Almeida, Marcelo Bordalo-Rodrigues |
|
|
IMD, Collaborator to Institute of Radiology at Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (InRad/HC-FMUSP), São Paulo, SP, Brazil
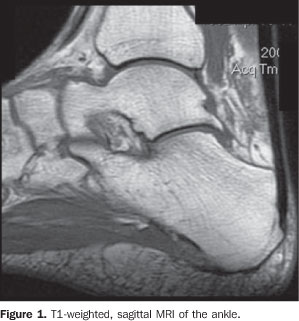
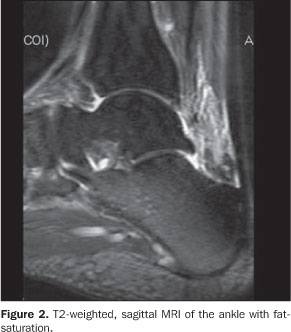
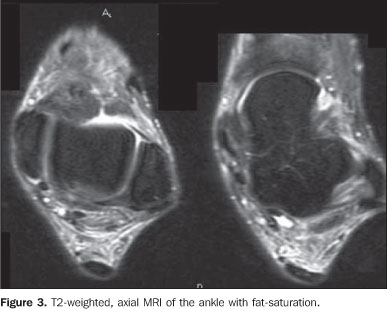
A male, 45-year-old patient undergoing antiretroviral therapy was referred with diagnosis of lipodystrophy for evaluation of plantar fat pad thickness. The patient presented with a mild pain in the posterior region of the ankle, with no history of trauma or fever. Images description Figures 1 to 4. Hypointense signal on the T1-weighted image of the Kager's fat pad, and hyperintense signal on T2-weighted images, indicating edema, with a normal aspect of bone, tendinous and ligamentous structures. Also, the calcaneus tendon as well as the paratendon present a normal aspect.
Diagnosis: Inflammatory process of Kager's fat pad associated with HIV-infection.
COMMENTS The number of HIV-infected persons has been increasing all over the world, but antiretroviral therapy improves the overall survival of these patients. Consequently, an increasing number of cases with involvement of the musculoskeletal system have been reported in the literature. In 2007, a non-specific presentation of inflammatory involvement of Hoffa's fat pad in association with HIV-infection was reported(1). Generally, these cases are associated with non-specific pain, with no predisposing factors. Like in all described cases of Hoffa's fat pad involvement, in the present case, the patient was also undergoing antiretroviral therapy, and up to the present moment this therapy could not be established as a single or associated causative factor. The association of the classical lipodystrophy secondary to the utilization of HIV-protease inhibitors has not been found and it is supposed that these are distinct and unrelated processes. Among the cases reported in the literature, three presented signs of avascular necrosis associated with adjacent bone structures. Although the relationship between avascular necrosis and use of antiretroviral has already been established, one could not affirm that inflammatory processes involving Hoffa's and Karger's fat pads are included in the spectrum of avascular necrosis or independent pathological processes. In the present case, the bone marrow signal was preserved. The differential diagnosis includes an inflammatory process related to the calcaneus tendon, especially a paratendinosis. In the present case, besides the involvement of the Karger's fat pad, there is a tendency of circumferential involvement of the calcaneus tendon by the edema, affecting the respective paratendon.
REFERENCE 1. Torshizy H, Pathria MN, Chung CB. Inflammation of Hoffa's fat pad in the setting of HIV: magnetic resonance imaging findings in six patients. Skeletal Radiol. 2007;36:35-40. [ ] |
|


Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554