Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 43 nº 3 - May / June of 2010
Vol. 43 nº 3 - May / June of 2010
|
ORIGINAL ARTICLE
|
|
Interobserver reproducibility of vascular indices obtained with three-dimensional power Doppler ultrasonography of embryos at 7 to 10 weeks and 6 days of gestation |
|
|
Autho(rs): João Bortoletti Filho, Luciano Marcondes Machado Nardozza, Edward Araujo Júnior, Liliam Cristine Rolo, Paulo Martin Nowak, Hélio Antonio Guimarães Filho, Antonio Fernandes Moron |
|
|
Keywords: First trimester of gestation, Color Doppler ultrasonography, Reproducibility of results, Three-dimensional imaging |
|
|
Abstract:
IMasters, MDs, Department of Obstetrics - Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil
INTRODUCTION The embryonic vasculogenesis starts at the 18th day, separately from the extra-embryonic vasculogenesis, in the parietal mesoderm of the intraembryonic coelom wall. The aggregates of endothelial cells form networks of angioblastic cords that accrete, grow and transform into cavities (angiocysts). These invade other tissues to form the embryonic vasculature that initially does not have blood vessels. As the embryo develops, the primary vessels network grows more by a process of vasculo-genesis than by a process of angiogenesis(1). Power Doppler ultrasonography, utilizing the signal received (echo) by the number of blood cells in motion, allows the detection of very slow flows as those in the small intraplacental vessels, and is not subject to the same limitations presented by conventional color Doppler technique, namely angle dependence and the aliasing effect(2). Three-dimensional power Doppler (3D power Doppler) allows the mapping of the embryonic vessels architecture, besides a quantitative evaluation by means of vascular indices (vascularization index - VI; flow index - FI; and vascularization and flow index - VFI)(1). The 3D power Doppler vascular indices have not demonstrated any correlation with the crown-rump length (CRL) at the first gestational trimester(1,3). The 3D power Doppler vascular indices have been applied in the evaluation of the placental vascularization at the second and third gestational trimesters, presenting a proven intra- and interobserver reproducibility(4,5). Recently, a good intraobserver reproducibility was also demonstrated for vascular indices of the intervillous and uteroplacental circulation between the 5th and 12th gestational weeks(6); however, no description is found about their reproducibility in the evaluation of the embryo's vascularization at the first gestational trimester. The present study was aimed at evaluating the interobserver reproducibility of 3D power Doppler vascular indices in embryos in the period between 7 and 10 weeks and 6 days of gestation.
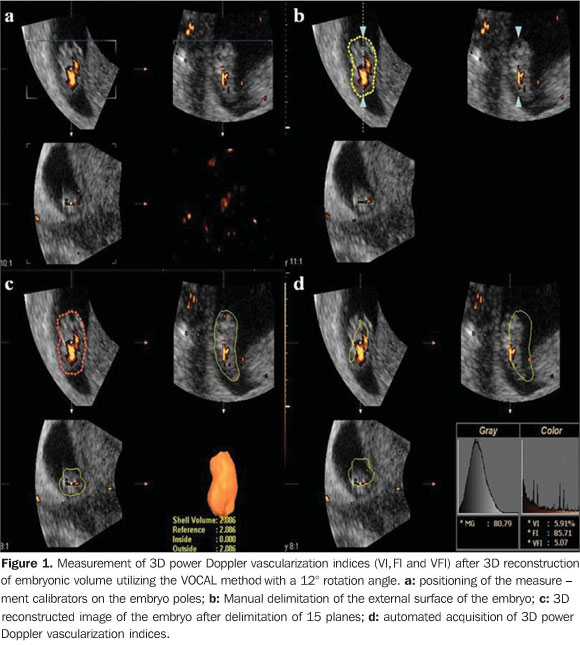
MATERIALS AND METHODS A prospective reproducibility study was developed with 36 healthy pregnant women at their 7th-10th gestational weeks. The present study was approved by the Committee for Ethics in Research of Universidade Federal de São Paulo (Unifesp), and all the patients signed a term of free and informed consent. The following inclusion criteria were considered: single gestation with live embryo; gestational age determined by the date of last menstruation and confirmed by ultrasonography performed up to the 10th gestational week using the CRL as a parameter; absence of vaginal bleeding, thermal index between 0.6 and 0.7; and maximum mechanical index of 0.3. Exclusion criteria were the following: pregnant women with chronic diseases (diabetes mellitus, arterial hypertension and collagenosis); smokers; use of illicit drug in the current pregnancy and low quality of volumes not allowing the appropriate evaluation of vascular indices. Such thermal and mechanical indices are within the safety limits for Doppler effects established by the European Committee for Radiation Safety(7) and by the American Institute of Ultrasound in Medicine(8). The patients were submitted to first- and second-trimester morphological ultrasonography, and underwent follow-up until their 22th gestational week in order to verify the occurrence of miscarriage which would lead to their exclusion. All the patients were selected at the Unit of Low-Risk Prenatal Care, Department of Obstetrics of Unifesp. The sonographic studies were performed with a Sonoace 8000 Live unit (Medison; Seoul, Korea) equipped with a volumetric and multifrequency endocavitary transducer (3D4-7EK). All the studies were performed by a single observer, with two-year experience in 3D ultrasonography in Obstetrics, with all the patients undergoing evaluation one single time. Initially, a real-time 2D evaluation was performed in order to measure the CRL, gestational sac diameter (arithmetic mean of the three largest diameters), and to evaluate embryonic heart rate. The following 3D power Doppler settings were standardized: frame rate (10), penetration frequency (low), enhance (1), reject (8), color Doppler gain (50), frame average (2), sensitivity (15), density (activates), balance (16), scala (1.5 kHz) and filter (1). An aperture angle of 30° was utilized, the scan velocity was normal and quality was high. Subsequently, the 3D key was activated, the three-dimensional window was displayed and positioned in such a way to comprise only the embryo (region of interest - ROI). After the three-dimensional scanning, the image was displayed on the screen in three orthogonal planes: axial, sagittal and coronal. The sagittal plane was selected as a reference, and it was magnified by 50%. Then, the embryo's image was moved to the center of the plane and rotated around the "z" axis, so that the embryo was horizontally visualized. In the sequence, the vocal key was activated with an angle of 12° and manual plane delimitation mode. The measurement calibrators were positioned at the embryo poles, and after the delimitation of 15 sequential planes, the equipment processed a reconstructed image with its volume expressed in cm3. After adjustments in the areas constituting the three-dimensional image, such image was accepted, and the vocal shell histogram key was activated, and the 3D power Doppler indices of the embryo (VI, FI and VFI) (Figure 1) were automatically calculated, VI corresponding to the number of color voxels and representing the percentage of the Doppler signal (vascularization) detected within the ROI; FI corresponding to the mean color value of all the color voxels, representing the mean intensity of the Doppler power signal within the ROI; and VFI, comprising the mean color value of all the color voxels and of the gray scale, constituting a combination of the other indices (originated from their multiplication and division of the result by 100) and has been suggested to be representative of the vascularization and flow intensity(9). At the end of the volumetric calculation, the VOCAL (Virtual Organ Computer-aided AnaLysis) software allows the return to each one of the delimited planes, in order to perform corrections on the embryo's contours, if necessary. In case such corrections were made, a new volume was obtained and consequently new vascular indices were also obtained. Two volumes were acquired from each patient, being such data stored in the equipment's memory. The volume presenting the highest vascular density was chosen to obtain the vascular indices. The volumetric and 3D power Doppler indices analyses were made in the absence of the patients by means of the software SonoView Pro version 1.03 (Medison; Seoul, Korea), being such analyses carried out by a single observer.
The data were stored on an Excel 2003 (Microsoft; Redmond, WA, USA) work-sheet and then analyzed by the statistical software SPSS for Windows version 13.0 (SPSS Inc.; Chicago, IL, USA). In order to evaluate the interobserver reproducibility of the 3D power Doppler vascular indices, a second observer, with a three-year experience in obstetric three-dimensional ultrasonography, performed blind measurements of the same 36 pregnant women. For the reproducibility calculation, the paired Student t-test, the intraclass correlation coefficient (ICC) and Bland-Altman plots were utilized. An ICC < 0.40 is considered as poor; between 0.40 and 0.75 is satisfactory and a correlation > 0.75 is excellent(10). The Bland-Altman plots demonstrate the mean value of the measurements performed by two observers against the difference of their measurements with agreement limits of 95% and 1.96 standard deviation(11). In all the analyses, the significance level (p) of 0.05 was utilized.
RESULTS Initially, 36 healthy pregnant women were selected. However one case was excluded because of a thermal index > 1.0 and three others were also excluded because of the low quality of obtained volumes as a consequence of transmission artifacts not allowing an appropriate evaluation of vascular indices. The 32 remaining pregnant women were followed-up until the 22nd gestational week, without any miscarriage, thus comprising the final sample. A good interobserver reproducibility was observed for the three analyzed vascular indices of 3D power Doppler. For VI, the mean difference between measurements was -1.1 (confidence interval [CI] 95%: -2.3 - 0.1) with the paired t-Student test demonstrating no significant difference among them (p = 0.09); the ICC was 0.9 (CI 95%: 0.8 - 0.9), while on the Bland-Altman plot the mean difference between measures was -1.1 (limits of agreement 95%: -8.0 - 5.8) (Figure 2a). For FI, the mean difference between measurements was -0.5 (CI 95%: -2.9 - 1.1), with the paired Student t-test showing no significant difference among them (p = 0.65); the ICC was 0.9 (CI 95%: 0.8 - 0.9), while in the Bland-Altman plot the mean difference between measurements was -1.1 (limits of agreement 95%: -8.0 - 5.8) (Figure 2b). For VFI, the mean difference between measurements was -1.1 (CI 95%: -2.2 - 0.4), with the paired Student t-test demonstrating no significant difference among them (p = 0.05); the ICC was 0.9 (CI 95%: 0.8 - 0.9), while on the Bland-Altman plot the mean difference between measurements was -1.1 (limits of agreement 95%: -5.0 - 5.1) (Figure 2c). Such results confirm the applicability of 3D power Doppler in the study of the embryonic vascularization at the first trimester of gestation, particularly with regards to FI, which presented the smallest mean difference between the measurements.
DISCUSSION The vascular indices of 3D power Doppler are not capable of quantifying the actual blood flow or perfusion, as the flow is the quantity of blood that passes through a vessel in a unit of time (generally per minute), while perfusion is defined as a quantity of flow in a volume of tissue per unit of time, and is generally measured as milliliters per minute per gram of tissue. As the three-dimensional vascular indices are not calculated as a function of time, their quantification cannot, consequently, match the actual perfusion or the flow of the studied tissue(12,13). Such indices would be, actually, a representation of power Doppler data contained within the three-dimensional volume, with VI being the percentage of power Doppler data contained within the volume, FI the mean intensity of the Doppler signal within the volume, and VFI a combination of both indices. However, it is suggested that such indices represent a semi-quantification of vascularization (VI) and flow intensity (FI)(13). In the present study, the VOCAL method was utilized for the volumetric assessment of the embryo. Such technique is relatively simple and is commercially available in several ultrasonography apparatuses Additionally, it presents a proven reproducibility in the evaluation of placental power Doppler vascular indices(4,5,14). A rotation angle of 12° was selected for allowing the determination of a higher number of planes (15) and, consequently, attempting to obtain higher accuracy in the measurements. In a study in vitro, measurements performed with an angle of 6° (30 planes) proved to be more reliable than those obtained with other rotation angles or multiplanar method, with the exception of the 9° angle (20 planes), and significantly more valid than those performed with a 30° angle or by the multiplanar method(15). In another study using an endometrium-like experimental model, the measurements performed with the VOCAL method with rotation at 15° (12 planes) demonstrated to be valid and reproducible(16). There are only two studies on the quantitative evaluation of embryonic vascularization at the first trimester of gestation(1,3), and in both cases no correlation between the vascular indices of the 3D power Doppler and CRL was observed. A possible explanation would be a state of homeostasis between demand of the tissues and the supply of blood from the vascular network in the first trimester of gestation(1). The interobserver reproducibility was tested with two volumes previously recorded by a single examiner. Therefore the reproducibility of the whole procedure, that is, from the volume acquisition, was not tested. There are two ways of analyzing reliability involving the use of the three-dimensional technique: by 3D volume acquisition and by volume calculation after definition of the contour by VOCAL method(17). The reliability of three-dimensional volume acquisition is directly related to the level of confidence in accurately performing the contour definition on which the volume will be calaculated18). Additionally, the data acquisition is much more subject to uncertainties than a series of measurements of any given data, particularly in Dopplerfluxometric studies(15). A good interobserver reproducibility was observed for the three 3D power Doppler vascular indices, with FI being the one with the lowest variability, with a mean difference between measurements of only -0.5. Previous studies in placentas have shown that FI is the index that best correlates with gestational age and the one presenting the lowest correlation coefficient in relation to the various measurements in the same placenta(14,19). Recently, the intervillous vascularization was evaluated in a gestational period similar to the one in the present study, 5 to 12 weeks and 6 days, observing that FI was the 3D power Doppler vascular index with highest ICC(6). This is explained by the increase of placental vascularization as the gestation progresses, which is consistent with histological data(20). Additionally, the increase in the number of vessels is followed by a progressive decrease in the vascular resistance, which contributes to the increase in perfusion and intraplacental flow(21). The results of the present study are in agreement with those obtained by a Spanish group that has utilized the placental biopsy technique, in which the authors obtained ICC above 0.85 for the three indices, with best intraobserver reproducibility for the flow indices (FI and VFI)(4). Recently, researchers evaluated the placental vascularization between the 12th and 40th gestational weeks, using the VOCAL method with manual delimitation of the whole external surface, and observed good intra- and interobserver reproducibility for the three indices, with FI presenting the highest ICC and the lowest difference between measurements(5). It should be highlighted that there are no studies on the reproducibility of 3D power Doppler vascular indices of embryos at the first trimester of gestation. In the present study, some FI measurement presented values above 100, which contradicts the definition of such index(6). The majority of the studies on 3D power Doppler have evaluated the placental vascularization at the first(6,22) as well as at the second and third gestational trimesters(14,19,23), observing that the FI values were within the normal variation range between 0 and 100. In previous studies the authors of the present study evaluated the vascularization in other structures such as the region of the middle cerebral artery of the fetus(24) and the embryo itself(3), observing that for these structures the maximum values of FI were above 100. A possible explanation for such fact would be the diverse vascular development of the placenta in relation to other fetal organs. The authors do not believe that the apparatus or training of the observers may have contributed for such result, considering that in a recent study developed by this same group, evaluating the placental vascularization at the second and third trimesters, using an apparatus from the same manufacturer with the same settings utilized in the present study, the mean values of FI ranged from 35.73 to 39.98(25). Further studies evaluating the vascularization of other structures or fetal organs are necessary to prove the actual validity of the 3D power Doppler vascular indices.
CONCLUSION The vascular indices, particularly the flow índex, obtained with 3D power Doppler ultrasonography at the first trimester of gestation demonstrated a high interobserver reproducibility.
REFERENCES 1. Kurjak A, Hafner T, Kupesiƒ S, et al. Three-dimensional power Doppler in study of embryonic vasculogenesis. J Perinat Med. 2002;30:18-25. [ ] 2. Yu CH, Chang CH, Ko HC, et al. Assessment of placental fractional moving blood volume using quantitative three-dimensional power Doppler ultrasound. Ultrasound Med Biol. 2003;29:19-23. [ ] 3. Bortoletti Filho J, Nardozza LM, Araujo Júnior E, et al. Embryo vascularization by three-dimensional power Doppler ultrasonography at 7-10 weeks of pregnancy. J Perinat Med. 2009;37:380-5. [ ] 4. Mercé LT, Barco MJ, Bau S. Reproducibility of the study of placental vascularization by three-dimensional power Doppler. J Perinat Med. 2004; 32:228-33. [ ] 5. de Paula CF, Ruano R, Campos JA, et al. Quantitative analysis of placental vasculature by three-dimensional power Doppler ultrasonography in normal pregnancies from 12 to 40 weeks of gestation. Placenta. 2009;30:142-8. [ ] 6. Mercé LT, Barco MJ, Alcázar JL, et al. Intervillous and uteroplacental circulation in normal early pregnancy and early pregnancy loss assessed by 3-dimensional power Doppler angiography. Am J Obstet Gynecol. 2009;200:315.e1-8. [ ] 7. Duck FA. Is it safe to use diagnostic ultrasound during the first trimester? Ultrasound Obstet Gynecol. 1999;13:385-8. [ ] 8. American Institute of Ultrasound in Medicine/National Electrical Manufactures Association. Standards for real-time display of thermal and mechanical acoustic output indices on diagnostic equipment. 2nd ed. Rockville, MD: American Institute of Ultrasound in Medicine; 1998. [ ] 9. Pairleitner H, Steiner H, Hasenoehrl G, et al. Three-dimensional power Doppler sonography: imaging and quantifying blood flow and vascularization. Ultrasound Obstet Gynecol. 1999;14: 139-43. [ ] 10. Shrout PE, Fleiss JL. Intraclass correlation: uses in assessing rater reliability. Psychol Bull. 1979; 86:420-8. [ ] 11. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307-10. [ ] 12. Cosgrove D, Eckersley R, Blomley M, et al. Quantification of blood flow. Eur Radiol. 2001;11: 1338-44. [ ] 13. Raine-Fenning NJ, Welsh AW, Jones NW, et al. Methodological considerations for the correct application of quantitative three-dimensional power Doppler angiography. Ultrasound Obstet Gynecol. 2008;32:115-7. [ ] 14. Guiot C, Gaglioti P, Oberto M, et al. Is three-dimensional power Doppler ultrasound useful in the assessment of placental perfusion in normal and growth-restricted pregnancies? Ultrasound Obstet Gynecol. 2008;31:171-6. [ ] 15. Raine-Fenning NJ, Clewes JS, Kendall NR, et al. The interobserver reliability and validity of volume calculation from three-dimensional ultrasound datasets in the in vitro setting. Ultrasound Obstet Gynecol. 2003;21:283-91. [ ] 16. Martins WP, Ferriani RA, Barra DA, et al. Reliability and validity of tissue volume measurement by three-dimensional ultrasound: an experimental model. Ultrasound Obstet Gynecol. 2007;29: 210-4. [ ] 17. Järvelä IY, Sladkevicius P, Tekay AH, et al. Intraobserver and interobserver variability of ovarian volume, gray-scale and color flow indices obtained using transvaginal three-dimensional power Doppler ultrasonography. Ultrasound Obstet Gynecol. 2003;21:277-82. [ ] 18. Duin LK, Willekes C, Vossen M, et al. Reproducibility of fetal renal pelvis volume measurement using three-dimensional ultrasound. Ultrasound Obstet Gynecol. 2008;31:657-61. [ ] 19. Mercé LT, Barco MJ, Bau S, et al. Assessment of placental vascularization by three-dimensional power Doppler "vascular biopsy" in normal pregnancies. Croat Med J. 2005;46:765-71. [ ] 20. Jauniaux E, Jurkovic D, Campbell S. In vivo investigations of the anatomy and physiology of early human placental circulations. Ultrasound Obstet Gynecol. 1991;1:435-45. [ ] 21. Reynolds LP, Redmer DA. Angiogenesis in the placenta. Biol Reprod. 2001;64:1033-40. [ ] 22. Rizzo G, Capponi A, Cavicchioni O, et al. Placental vascularization measured by three-dimensional power Doppler ultrasound at 11 to 13 + 6 weeks' gestation in normal and aneuploid fetuses. Ultrasound Obstet Gynecol. 2007;30:259-62. [ ] 23. Zalud I, Shaha S. Evaluation of the utero-placental circulation by three-dimensional Doppler ultrasound in the second trimester of normal pregnancy. J Matern Fetal Neonatal Med. 2007;20: 299-305. [ ] 24. Nardozza LM, Araujo Júnior E, Simioni C, et al. Evolution of 3-D power Doppler indices of fetal brain in normal pregnancy. Ultrasound Med Biol. 2009;35:545-9. [ ] 25. Guimarães Filho HA, Araujo Júnior E, Mattar R, et al. Placental blood flow measured by three-dimensional power Doppler ultrasound at 26 to 35 weeks gestation in normal pregnancies. J Matern Fetal Neonatal Med. 2010;23:69-73. [ ] Received March 3, 2010. * Study developed at the Unit of Three-Dimensional Ultrasonography, Department of Obstetrics - Universidade Federal de São Paulo (Unifesp), São Paulo, SP, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554