Sr. Editor,
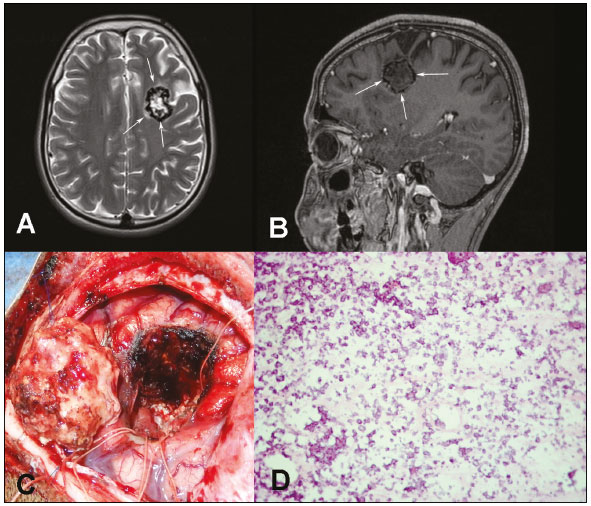
Paciente do sexo masculino, 17 anos, com história de crises convulsivas tonicoclônicas generalizadas desde os cinco anos de idade, foi encaminhado ao nosso serviço para investigação. A ressonância magnética (RM) mostrou lesão expansiva no lobo frontal esquerdo, com hipossinal em T1 e hipersinal em T2, com halo de hipossinal nas duas sequências, sem realce pelo meio de contraste e com discreto edema circunjacente (Figuras 1A e 1B). A lesão foi totalmente ressecada (Figura 1C) e enviada para estudo histopatológico e imuno-histoquímico (Figura 1D), sendo concluído o diagnóstico de pseudoneoplasia calcificada do neuroeixo (
calcifying pseudoneoplasm of the neuraxis – CAPNON). O paciente está sendo acompanhado há dois anos, sem sinais clínicos ou radiológicos de recidiva.
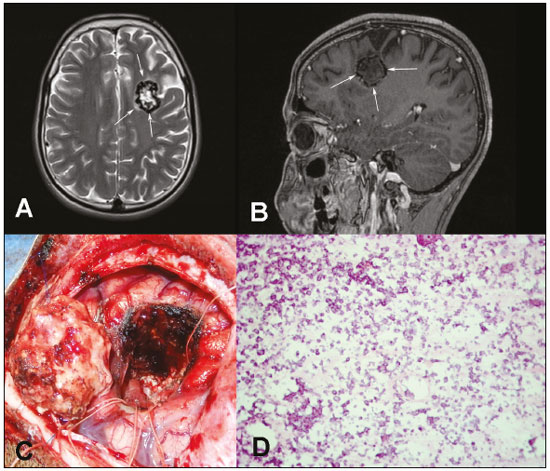 Figura 1.
Figura 1. RM pré-operatória nas sequências T2 sem contraste (
A) e T1 pós-contraste (
B) mostrando lesão expansiva no lobo frontal esquerdo, com halo de hipossinal nas duas sequências, componente interno com hipersinal em T2 e hipossinal em T1, sem realce pelo meio de contraste e com discreto edema circunjacente.
C: Imagem intraoperatória da pseudoneoplasia calcificada após ressecção total.
D: Corte histológico do pseudotumor exibindo inúmeros focos de calcificação (microcalcificações), que correspondem às células da lesão. Raras células viáveis de permeio só podem ser demonstradas pelo estudo por imuno-histoquímica (hematoxilina e eosina, ampliação 20×).
CAPNON, também conhecida como lesão fibro-óssea do sistema nervoso central (SNC), é uma lesão benigna rara, primeiramente relatada por Rhodes et al. em 1978
(1). A CAPNON caracteriza-se por ser lesão calcificada, de crescimento lento, normalmente única e que pode ter localização em qualquer parte do SNC. A origem ainda não é totalmente conhecida, porém, com base na evolução clínica benigna e nos achados histopatológicos, acredita-se em um processo reacional a fatores como trauma, infecção, inflamação ou neoplasias
(2,3). Segundo García Duque et al.
(4), a maioria dos casos publicados na literatura ocorreu em homens (59,38%) e em sítio intracraniano (54,2%), principalmente supratentorial. Os principais sintomas relacionados à CAPNON são cefaleia, convulsões e sintomas focais neurológicos. Todavia, a apresentação clínica vai depender da localização, das dimensões e do consequente efeito de massa provocado pela lesão
(4,5).
Os exames de imagem são importantes ferramentas para o diagnóstico de lesões tumorais do SNC
(6–10), servindo também para a caracterização da CAPNON e para incluí-la na lista de diagnósticos diferenciais de lesão calcificada no SNC. A maior parte dos casos descritos na literatura apresenta-se na radiografia convencional e na tomografia computadorizada como lesão sólida e calcificada, ou com calcificações periféricas. Na RM, normalmente apresenta hipossinal em T1 e T2, com mínimo ou nenhum realce pelo meio de contraste e raramente apresenta edema
(11,12). Entretanto, alguns casos foram descritos com sinais variados em T1 e T2, ou ainda com presença de edema e realce importante pelo meio de contraste
(12).
O diagnóstico depende do estudo histopatológico, que se caracteriza pela presença de nódulos com matriz condromixoide, calcificações finas, corpos psamomatosos de permeio, quantidades variáveis de estroma fibroso e células epitelioides e fusiformes na periferia. A presença de cada componente é altamente variável entre os casos descritos. Os achados da imuno-histoquímica mais comuns são a presença de antígeno epitelial de membrana e vimentina, e a ausência de proteína acida glial fibrilar e da proteína S100
(3,12).
A ressecção cirúrgica é o tratamento de escolha e normalmente apresenta bom prognóstico, não havendo relato na literatura de recidiva após remoção completa da CAPNON
(11). Nos diagnósticos diferenciais por imagem incluem-se cavernoma, meningioma, lesões infecciosas (neurocisticercose, tuberculose), oligodendroglioma e astrocitoma com calcificações
(3,12,13). Em razão do aumento do número de casos descritos nos últimos anos, a CAPNON deve entrar no diagnóstico diferencial das lesões calcificadas no SNC.
REFERÊNCIAS1. Rhodes RH, Davis RL. An unusual fibro-osseous component in intracranial lesions. Hum Pathol. 1978;9:309–19.
2. Aiken AH, Akgun H, Tihan T, et al. Calcifying pseudoneoplasms of the neuraxis: CT, MR imaging, and histologic features. AJNR Am J Neuroradiol. 2009;30:1256–60.
3. Serrano-Pardo R, Valls AB, Benítez HS, et al. Pseudoneoplasia calcificante del sistema nervioso central. A propósito de un caso y revisión de la literatura. Rev Esp Patol. 2009;42;155–8.
4. García Duque S, Medina Lopez D, Ortiz de Méndivil A, et al. Calcifying pseudoneoplasms of the neuraxis: report on four cases and review of the literature. Clin Neurol Neurosurg. 2016;143:116–20.
5. Giardina F, Guerra G, Righi A, et al. Calcifying pseudotumor of the spine: a case report. Clin Surg. 2016;1:1042.
6. Queiroz RM, Abud LG, Abud TG, et al. Burkitt-like lymphoma of the brain mimicking an intraventricular colloid cyst. Radiol Bras. 2017;50: 413–4.
7. Langer FW, Santos D, Alves GRT, et al. Malignant peripheral nerve sheath tumor of the vagus nerve: an uncommon cause of progressive dyspnea. Radiol Bras. 2017;50:412–3.
8. Abreu PP, Muniz BC, Ventura N, et al. Intraventricular ganglioglioma with dissemination of cerebrospinal fluid. Radiol Bras. 2018;51:272–3.
9. Niemeyer B, Muniz BC, Ventura N, et al. Papillary tumor of the pineal region accompanied by Parinaud''s syndrome: magnetic resonance imaging findings. Radiol Bras. 2018;51:202–4.
10. Muniz BC, Niemeyer B, Ventura N, et al. Primary intraosseous meningioma: atypical presentation of a common tumor. Radiol Bras. 2018;51: 412–3.
11. Krejčí T, Buzrla P, Vecera Z, et al. Calcifying pseudoneoplasm of the neural axis – a case report. Cesk Slov Neurol N. 2015;78/111:568–75.
12. Stienen MN, Abdulazim A, Gautschi OP, et al. Calcifying pseudoneoplasms of the neuraxis (CAPNON): clinical features and therapeutic options. Acta Neurochir (Wien). 2013;155:9–17.
13. Lyapichev K, Bregy A, Shah AH, et al. Occipital calcified pseudoneoplasms of the neuraxis (CAPNON): understanding a rare pathology. BMJ Case Rep. 2014;2014.
1. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brasil;
https://orcid.org/0000-0002-8308-1920 2. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brasil;
https://orcid.org/0000-0002-4765-8526 3. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brasil;
https://orcid.org/0000-0003-2412-8239 4. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brasil;
https://orcid.org/0000-0002-9306-7145 5. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brasil;
https://orcid.org/0000-0001-8797-7380Correspondência: Dra. Rafaela Fonseca Albuquerque Pithon
UFRJ – Departamento de Radiologia
Rua Rodolpho Paulo Rocco, 255, Cidade Universitária, Ilha do Fundão
Rio de Janeiro, RJ, Brasil, 21941-913
E-mail:
rafaelafa@hotmail.com.brRecebido para publicação em 22/9/2017.
Aceito, após revisão, em 14/12/2017.

 |
|



 Read in English
Read in English
 PDF Portuguese
PDF Portuguese
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket