Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 49 nº 1 - Jan. /Feb. of 2016
Vol. 49 nº 1 - Jan. /Feb. of 2016
|
CASE REPORT
|
|
Glenohumeral interposition of rotator cuff stumps: a rare complication of traumatic rotator cuff tear |
|
|
Autho(rs): Paulo Moraes Agnollitto1; Marcio Wen King Chu2; Mario Muller Lorenzato3; Salomão Chade Assan Zatiti4; Marcello Henrique Nogueira-Barbosa5 |
|
|
Keywords: Interposition; Rotator cuff; Tear; Trauma; Shoulder; Magnetic resonance imaging. |
|
|
Abstract: INTRODUCTION
Traumatic rotator cuff injury is rarely observed in young patients and generally occurs after high-energy trauma. Even more rarely, traumatic rotator cuff injury may be associated with interposition of stumps or more than one of the rotator cuff tendons between the humerus and the glenoid(1-5). In the case of rotator cuff stumps interposition in the glenohumeral joint (GHJ), the most common clinical presentation is articular blockage, many times with persistence of subluxation and/or irreducible luxation of the GHJ(4-8). The objective of this report is to describe a surgically confirmed case with characteristic imaging findings of traumatic rotator cuff injury with multiple stumps interposition between the glenoid and the humerus. CASE REPORT A female, 27-year-old patient was referred to the emergency unit, at another service, with a history of motorcycle accident occurred about two hours before her arrival at the unit. She presented with pain and limited range of motion in her right shoulder. At the initial approach, there was no report of GHJ dislocation, and the patient was discharged with analgesic medication. No supplementary tests or imaging studies were performed. The patient evolved with right shoulder pain and block-age and, 15 days after the episode, she sought specialized assistance, undergoing plain radiography of her right shoulder. The analysis of the images showed coracoid process fracture, GHJ space widening, and internal humeral rotation (Figure 1). No signs of glenohumeral dislocation or instability were found at the radiographic images. 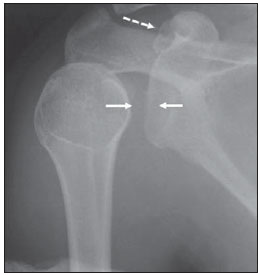 Figure 1. Radiography of right shoulder. Anteroposterior view showing glenohumeral joint space widening (continuous arrows). The humerus presented with internal rotation. The dashed arrow indicates fracture of the coracoid process. The hypothesis of traumatic rotator cuff tear was raised on the basis of the plain radiography findings, and the patient was submitted to magnetic resonance imaging (MRI) whose images demonstrated the presence of a traumatic injury with interposition of the supraspinatus, infraspinatus and subscapularis tendons stumps in the GHJ (Figures 2 and 3). Coracoid process fracture, diffuse periarticular edema, and edema of intermuscular fat planes were also identified. 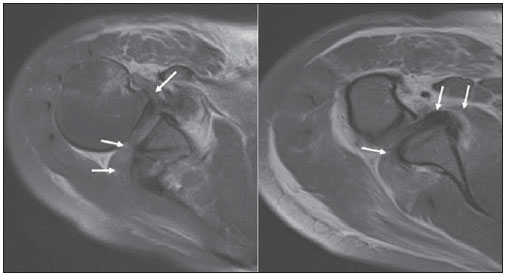 Figure 2. MRI. Axial sections images acquired with intermediate weighting demonstrates rotator cuff stumps interposition (arrows) between the glenoid and the humerus, explaining the blockage and the joint space widening.  Figure 3. MRI, coronal section, intermediate weighting. The arrows identify rotator cuff stumps interposition between the glenoid and the humerus. The white arrow indicates the supraspinatus tendon and the black arrow shows the subscapularis tendon. Then, the patient was submitted to open surgical exploration, with diagnostic confirmation and rotator cuff reinsertion (Figure 4). 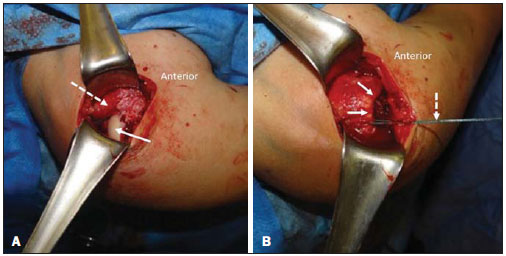 > >Figure 4. A: Intraoperative finding demonstrating uncovered humeral head (continuous arrow) and retracted and interposed rotator cuff stumps in the glenohumeral joint (dashed arrow). B: Intraoperative finding demonstrating rotator cuff (continuous arrows), repaired by surgical thread (dashed arrow) coursing up to the site of insertion of the greater humeral tuberosity. The patient presented a good evolution over the immediate postoperative period and was discharged. Three months after the surgery, she presented with external rotation restriction and was submitted to arthroscopy that revealed the presence of adhesions, which were released. After this new peocedure, the patient evolved satisfactorily, without any new complication. DISCUSSION Traumatic rotator cuff stumps interposition in the GHJ is a very rare complication in shoulder trauma. In general, it occurs as a result from high-energy trauma, and frequently is associated with either anterior or posterior GHJ luxation. Relatively few articles on this subject are found in the literature, and most of them are case reports. Difficulty or incapacity to reduce GHJ luxation is not common(1-3). Irreducible GHJ luxation may be related to bone tissue or soft tissues interposition(1,2,4,6-10). Amongst the causes associated with soft tissues interposition, one can mention, for example, interposition of the long head of biceps(9) and interposition of the musculocutaneous nerve(10); however, interposition of rotator cuff tendons, particularly the subscapularis tendon, is highlighted(2,4,5,7,8). Soft tissues interposition and bone tissue interposition may occur concomitantly(2). Most cases reported in the literature are associated with high-energy trauma, with episodes of traumatic GHJ luxation(1-5); however, like in the present case, the history of luxation is not always well established(3). As our patient was initially assisted in other service, such a possibility cannot be completely ruled out. The clinical presentation of glenohumeral interposition of rotator cuff stumps also includes pain and varied degrees of functional limitation or joint blockage. The clinical diagnosis is difficult to be made, and suspicious should be raised in cases where previous radiographic images and those obtained after articular reduction attempts demonstrate persistence of subluxation or articular space widening(2). The radiological signs are subtle, but should be taken into consideration in the clinical context. In the present case, as well as in the literature review, the authors highlight the role played by MRI in the identification of post-trauma interposition of soft tissues in the GHJ(1,2,5). Such a role is not restricted to cases involving the shoulders, and MRI has been utilized, for example, to detect post-trauma periosteal interposition in growth cartilage fracture in children and adolescents(11,12). In case of irreducible GHJ luxation, computed tomography may be utilized to better identify bone fragments blocking the reduction, but such a method is limited to evaluate soft tissues(2-5). The management of traumatic rotator cuff injury with tendons entrapment in the GHJ should be surgical, and an early diagnosis can minimize the damages to the involved muscle bellies and tendons, improving the postoperative results(2,5). Because of its rarity, such a condition may be easily neglected at emergency settings(1-3), and a previous knowledge about this entity by radiologists and orthopedists is critical for a correct diagnosis and institution of an appropriate treatment. In the present case, the authors conclude that the evaluation by MRI was appropriate to identify the post-trauma rotator cuff tendons entrapment in the GHJ. REFERENCES 1. Lin CL, Su WR, Jou IM, et al. Occult interpositional rotator cuff - an extremely rare case of traumatic rotator cuff tear. Korean J Radiol. 2012;13:98-101. 2. Walch G, Boulahia A, Robinson AH, et al. Posttraumatic subluxation of the glenohumeral joint caused by interposition of the rotator cuff. J Shoulder Elbow Surg. 2001;10:85-91. 3. Rickert M, Loew M. Glenohumeral interposition of a torn rotator cuff in a young motorcyclist. Arch Orthop Trauma Surg. 2006;126:184-7. 4. Connolly S, Ritchie D, Sinopidis C, et al. Irreducible anterior dislocation of the shoulder due to soft tissue interposition of subscapularis tendon. Skeletal Radiol. 2008;37:63-5. 5. Ilaslan H, Bilenler A, Schils J, et al. Pseudoparalysis of shoulder caused by glenohumeral interposition of rotator cuff tendon stumps: a rare complication of posterior shoulder dislocation. Skeletal Radiol. 2013;42:135-9. 6. Davies MB, Rajasekhar C, Bhamra MS. Irreducible anterior shoulder dislocation: the greater tuberosity Hill-Sachs lesion. Injury. 2000;31:470-1. 7. Bridle SH, Ferris BD. Irreducible acute anterior dislocation of the shoulder: interposed subscapularis. J Bone Joint Surg Br. 1990;72:1078-9. 8. Tietjen R. Occult glenohumeral interposition of a torn rotator cuff. A case report. J Bone Joint Surg Am. 1982;64:458-9. 9. Mihata T, Doi M, Abe M. Irreducible acute anterior dislocation of the shoulder caused by interposed fragment of the anterior glenoid rim. J Orthop Sci. 2000;5:404-6. 10. Gudena R, Iyengar KP, Nadkarni JB, et al. Irreducible shoulder dislocation - a word of caution. Orthop Traumatol Surg Res. 2011;97:451-3. 11. Moura MVT. Trapped periosteum in a distal femoral physeal injury: magnetic resonance imaging evaluation. Radiol Bras. 2012;45:184-6. 12. Raman S, Wallace EC. MRI diagnosis of trapped periosteum following incomplete closed reduction of distal tibial Salter-Harris II fracture. Pediatr Radiol. 2011;41:1591-4. 1. Physician Assistant at Division of Radiology, Hospital das Clínicas - Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (HCFMRP-USP), Ribeirão Preto, SP, Brazil 2. Volunteer Physician, Fellow of Musculoskeletal Radiology, Division of Radiology at Hospital das Clínicas - Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (HCFMRP-USP), Ribeirão Preto, SP, Brazil 3. MD, Radiologist, Clínica Radiologia Especializada, Ribeirão Preto, SP, Brazil 4. MD, Orthopedist, Hospital Especializado de Ribeirão Preto, Ribeirão Preto, SP, Brazil 5. Associate Professor of Radiology, Centro de Ciências das Imagens e Física Médica (CCIFM) - Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (FMRP-USP), Ribeirão Preto, SP, Brazil Mailing Address: Dr. Paulo Moraes Agnollitto Divisão de Radiologia / CCIFM, FMRP-USP Avenida Bandeirantes, 3900, Monte Alegre Ribeirão Preto, SP, Brazil, 14048-900 E-mail: agno53@gmail.com Received October 31, 2013. Accepted after revision April 10, 2014. Study developed at Hospital das Clínicas Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo(HCFMRP-USP), Ribeirão Preto, SP, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554