Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 48 nº 3 - May / June of 2015
Vol. 48 nº 3 - May / June of 2015
|
LETTER TO THE EDITOR
|
|
Hypertrophic olivary degeneration secondary to central tegmental tract injury |
|
|
Autho(rs): Nicole Almeida de Alencar Araujo; Mariana Trombetta de Lima Raeder; Nivaldo Adolfo da Silva Junior; Mariana Mari Oshima; Luis Otavio Parizotto; Fabiano Reis |
|
|
Dear Editor,
A male, 30-year-old patient presenting with a sudden-onset convergent squint attended the service complaining of diplopia. At physical examination the patient presented compromise of the left VI nerve and palatal myoclonus. Magnetic resonance imaging (Figure 1) demonstrated hypertrophic olivary degeneration (HOD) secondary to central tegmental tract injury. 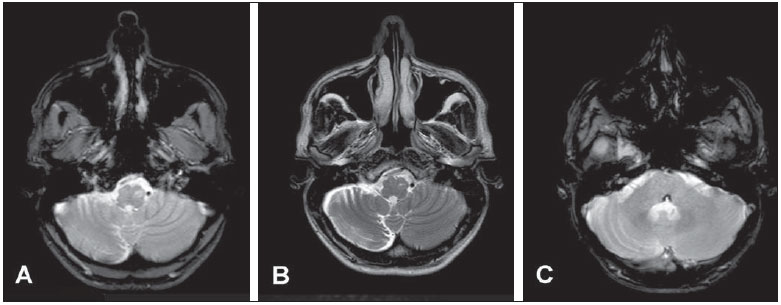 Figure 1. MRI of the brain. Axial, T2-weighted FFE image at the level of the bulb (A) and axial T2-weighted image (B) shows hypersignal in the region of the left inferior olivary nucleus, as well as accentuation of sulci in the right cerebellar hemisphere. Susceptibility-weighted imaging (C) at the level of the pons shows lesion with peripheral hyposignal in the pontine tegmentum (left facial colliculus), compatible with hemorrhagic focus. Recently, the Brazilian radiological literature has been much concerned about the relevant role played by imaging methods in the improvement of the diagnosis of central nervous system diseases.(1-10) HOD is a rare phenomenon that occurs after an insult to the dentato-rubro-olivary tract (Guillain-Mollaret triangle), constituted by the dentate, rubro and inferior olivary nuclei, which are interconnected via the central tegmentar tract and superior and inferior cerebellar peduncles. This is a degenerative disorder that initially develops with hypertrophy(11). Injury to any of such components may result in axonal interruption to the inferior olivary nucleus, leading to its degeneration(12). In cases where the alterations are restricted to the central tegmentar tract, the HOD is ipsilateral, like in the present case. In cases where there is involvement of the dentate nucleus or of the dentate nucleus or superior cerebellar peduncle, the HOD is contralateral. Bilateral compromise may be observed in cases where the lesion simultaneously affects the superior cerebellar peduncle and the contralateral central tegmentar tract, or in case of compromise of both central tegmentar tracts(11,13). HOD is characterized as a lesion with hypersignal on T2-weighted images, in the anterolateral portion of the bulb, in the olivary region, associated with increase in the volume of such a structure that does not present contrast enhancement. Additionally, the volumetric reduction of the cerebellar hemisphere contralateral to the olivary alteration corroborates the diagnosis(14). HOD occurs as a result of a range of insults. The symptoms are classically associated with palatal and ocular myoclonus, besides tremors. Such abnormal involuntary movements are consequential to failure of inhibition of inferior olive, since the fibers originated in the dentate nucleus are primarily inhibitory or GABAergic. In such case, expectant management is the approach to be adopted. Macroscopic findings reveal hypertrophy instead of olivary atrophy, which is a particularity of this transsynaptic degeneration. Histopathologically, there is hypertrophy of both neurons (due to proliferation of neurofilaments and cytoplasmic vacuolization) and glial cells. REFERENCES 1. Castro FD, Reis F, Guerra JGG. Lesões expansivas intraventriculares à ressonância magnética: ensaio iconográfico - parte 1. Radiol Bras. 2014;47:176-81. 2. Dias DA, Castro FLO, Yared JH, et al. Membrana de Liliequist: avaliação radiológica e suas implicações clínicas e terapêuticas. Radiol Bras. 2014;47:182-5. 3. Leite CC. O potencial do gamaprobe na detecção do foco epileptogênico. Radiol Bras. 2014;47(1):ix. 4. Alfenas PR, Ribeiro BNF, Bahia PRV, et al. Síndrome de Parry-Romberg: achados nas sequências avançadas de ressonância magnética - relato de caso. Radiol Bras. 2014;47:186-8. 5. Carneiro Filho O, Vilela Filho O, Ragazzo PC, et al. Um novo método para a localização intraoperatória de foco de epilepsia mediante utilização de gamaprobe. Radiol Bras. 2014;47:23-7. 6. Lara Filho LA, Omar SS, Biguelini RF, et al. Achados tomográficos de pacientes submetidos a tomografia de crânio no pronto-socorro do Hospital Universitário Cajuru. Radiol Bras. 2013;46:143-8. 7. Carvalho GBS, Sandim GB, Tibana LAT, et al. Diagnóstico diferencial das lesões inflamatórias e infecciosas do cone medular utilizando a ressonância magnética. Radiol Bras. 2013;46:51-5. 8. Fiore L, Silva Junior NA, Bertanha R, et al. Fístula arteriovenosa dural intracraniana [Qual o seu diagnóstico?]. Radiol Bras. 2013;46(4):xi-xii. 9. Reis F, Schwingel R. Linfoma do sistema nervoso central: ensaio iconográfico. Radiol Bras. 2013;46:110-6. 10. Brandão LA. Linfoma primário e secundário do sistema nervoso central. Aspectos de imagem na ressonância magnética convencional e funcional. Radiol Bras. 2013;46(2):ix-x. 11. Hornyak M, Osborn AG, Couldwell WT. Hypertrophic olivary degeneration after surgical removal of cavernous malformations of the brain stem: report of four cases and review of the literature. Acta Neurochir (Wien). 2008;150:149-56. 12. Krings T, Foltys H, Meister IG, et al. Hypertrophic olivary degeneration following pontine haemorrhage: hypertensive crisis or cavernous haemangioma bleeding? J Neurol Neurosurg Psychiatry. 2003;74:797-9. 13. Birbamer G, Buchberger W, Felber S, et al. MR appearance of hypertrophic olivary degeneration: temporal relationships. AJNR Am J Neuroradiol. 1992;13:1501-3. 14. Shepherd GM, Tauböll E, Bakke SJ, et al. Midbrain tremor and hypertrophic olivary degeneration after pontine hemorrhage. Mov Disord. 1997;12:432-7. Universidade Estadual de Campinas (Unicamp), Campinas, SP, Brazil Mailing Address: Dra. Nicole Almeida de Alencar Araújo Faculdade de Ciências Médicas, Universidade Estadual de Campinas, Departamento de Radiologia Rua Tessália Vieira de Camargo, 126, Cidade Universitária Zeferino Vaz. Caixa Postal: 6111 Campinas, SP, Brazil, 13083-887 E-mail: nicoledealencar@gmail.com |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554