Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 48 nº 3 - May / June of 2015
Vol. 48 nº 3 - May / June of 2015
|
LETTER TO THE EDITOR
|
|
Mammographic artifact leading to false-positive result |
|
|
Autho(rs): Matheus Silveira Avelar; Orlando Almeida; Beatriz Regina Alvares |
|
|
Dear Editor,
A female, 75-year-old was referred by another service with previous screening mammogram demonstrating clustered pleomorphic microcalcifications in the superolateral quadrant of her left breast, classified as highly suspicious mammographic findings (BI-RADS category 5), to be submitted to mammography-guided needle localization followed by excisional biopsy of the suspicious lesion. A new mammography demonstrated an apparently benign nodule already present and stable in relation to the findings of the previous mammogram, besides the presence of clustered pleomorphic microcalcifications, both findings located in the superolateral quadrant of the left breast. The finding of suspicious microcalcifications drew attention for being a round-shaped cluster (Figures 1A and 1B). 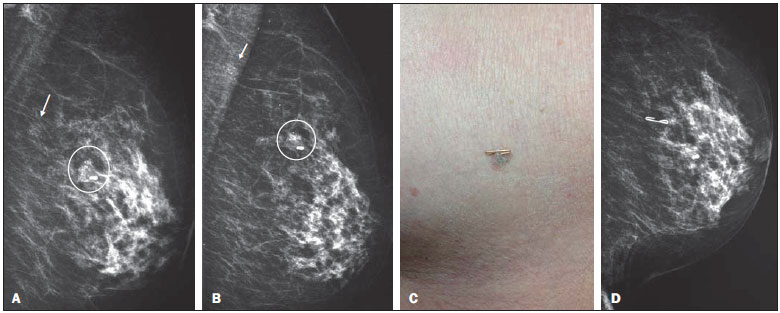 Figure 1. A,B: Mediolateral oblique and craniocaudal views of left breast showing a partially calcified nodule (circle) and a cluster of pleomorphic microcalcifications (arrow) located in the superolateral quadrant of the breast. C,D: Metal clip on the dermal nevus with talc residues in its fissures, and craniocaudal view of the left breast demonstrating that the cluster of microcalcifications corresponded to talc residues. A new assessment detected a skin nevus with irregular surface presenting with talc residues in the lesion fissures. Once the lesion was marked with a metal clip, a new mammographic image revealed that the microcalcifications corresponded to artifacts related to the talc residues present on the dermal nevus surface (Figures 1C and 1D). The mammogram was reclassified as benign mammographic findings (BI-RADS category 2) and the patient was referred for follow-up at the public basic health network. Except for non-melanoma skin tumors, breast cancer is the most frequent neoplasm with high mortality in women in Brazil(1). Mammography is the main imaging method for the early diagnosis of breast cancer; and the analysis of the differences between normal breast tissue and suspicious findings requires high imaging quality for early detection of lesions(2-9). In addition, the presence of imaging artifacts reduces the sensitivity and specificity of imaging methods, masking or mimicking the diagnosis of initial-stage lesions and leading to the adoption os inappropriate approaches. Most common artifacts are associated with factors related to the patient, to the imaging technique, image processing or problems in the apparatus(10,11). The main patient-related artifacts are caused by motion during images acquisition and use of substances on the skin. The present case illustrates the necessity of a strict mammographic image quality control and correlation with clinical findings for greater diagnostic accuracy. As already mentioned, the skin lesion led to simulation of a clustered pleomorphic microcalcifications which would imply the necessity of biopsy. The active quest for prevention and detection of artifacts, in association with a continued quality control of imaging, processing, storage and images analysis, reduces the incidence of misdiagnosis and costs, e should be the objective of any team involved in mammography services. REFERENCES 1. Brasil. Ministério da Saúde. Instituto Nacional do Câncer. Estimativas 2012 - Incidência de câncer no Brasil. Rio de Janeiro, RJ: INCA; 2011. 2. Pisano ED, Hendrick RE, Yaffe MJ, et al. Diagnostic accuracy of digital versus film mammography: exploratory analysis of selected population subgroups in DMIST. Radiology. 2008;246:376-83. 3. Caldas FAA, Isa HLVR, Trippia AC, et al. Controle de qualidade e artefatos em mamografia. Radiol Bras. 2005;38:295-300. 4. Badan GM, Roveda Júnior D, Ferreira CAP, et al. Auditoria interna completa do serviço de mamografia em uma instituição de referência em imaginologia mamária. Radiol Bras. 2014;47:74-8. 5. Bitencourt AGV, Lima, ENP, Chojniak R, et al. Correlação entre resultado do PET/CT e achados histológicos e imuno-histoquímicos em carcinomas mamários. Radiol Bras. 2014;47:67-73. 6. Rodrigues DCN, Freitas-Junior R, Corrêa RS, et al. Avaliação do desempenho dos centros de diagnóstico na classificação dos laudos mamográficos em rastreamento oportunista do Sistema Único de Saúde (SUS). Radiol Bras. 2013;46:14955. 7. Coeli GNM, Reis HF, Bertinetti DR, et al. Carcinoma mucinoso da mama: ensaio iconográfico com correlação histopatológica. Radiol Bras. 2013;46:2426. 8. Pardal RC, Abrantes AFL, Ribeiro LPV, et al. Rastreio de lesões mamárias: estudo comparativo entre a mamografia, ultrassonografia modo-B, elastografia e resultado histológico. Radiol Bras. 2013;46:21420. 9. Badan GM, Roveda Júnior D, Ferreira CAP, et al. Valores preditivos positivos das categorias 3, 4 e 5 do Breast Imaging Reporting and Data System (BI-RADS®) em lesões mamárias submetidas a biópsia percutânea. Radiol Bras. 2013;46:20913. 10. Chaloeykitti L, Muttarak M, Ng KH. Artifacts in mammography: way to identify and overcome them. Singapore Med J. 2006;47:63441. 11. Geiser WR, Haygood TM, Santiago L, et al. Challenges in mammography: Part I, artifacts in digital mammography. AJR Am J Roentgenol. 2011;197:102330. Departamento de Radiologia da Faculdade de Ciências Médicas da Universidade Estadual de Campinas (FCM-Unicamp), Campinas, SP, Brazil Endereço para correspondência: Dr. Matheus Silveira Avelar Rua Hermantino Coelho, 299, ap. 114A, Bairro Mansões Santo Antônio Campinas, SP, Brazil, 13087-500 E-mail: avelarmatheus@ig.com.br |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554