Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 48 nº 1 - Jan. /Feb. of 2015
Vol. 48 nº 1 - Jan. /Feb. of 2015
|
LETTER TO THE EDITOR
|
|
Epidural cavernous hemangioma of the spine: magnetic resonance imaging findings |
|
|
Autho(rs): Marcelo Mantiolhe Martins1; Flavia Angelica Ferreira Francisco1; Rafael Alfenas de Paula1; Daniella Braz Parente2 |
|
|
Dear Editor,
A previously healthy male, 52-year-old patient complaining of progressive lower limbs paraparesis for four months and recent onset of urinary incontinence, with no history of local trauma. At admission, the patient was afebrile and, at physical examination presented with spastic paraparesis with sensitive level at D8. Laboratory tests (blood count and biochemical blood tests) did not demonstrate any significant alteration. Magnetic resonance imaging (MRI) demonstrated the presence of an elongated lesion with regular contour, intermediate signal intensity on T1-weighted and marked hypersignal on T2-weighted sequences, with intense and homogeneous contrast enhancement, located in the epidural space, extending from D5 to D7. Such a lesion determined a significant narrowing of the rachidian canal and medullary compression on the corresponding segments, with consequential medullary hypersignal on T2-weighted and STIR sequences compatible with compressive myelopathy (Figure 1). 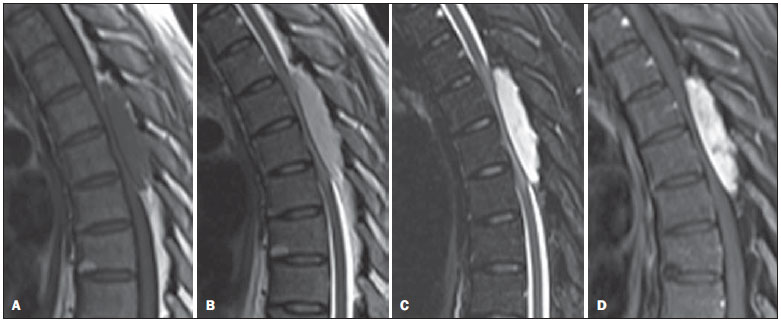 Figure 1. Sagittal MRI T1-weighted (A), T2-weighted (B), STIR (C) and T1-weighted sequences with fat saturation following intravenous contrast injection (D) demonstrating an elongated, expansile well-delimited lesion with regular contour, located in the epidural space of the posterior region of the dorsal spine, extending from D5 to D7. The lesion presents intermediate signal on T1-, marked hypersignal on T2-weighted and STIR sequences, with intense and homogeneous contrast enhancement, suggestive of hemangioma. Such a tumor causes remarkable narrowing of the rachidian canal, determining high signal intensity in the spinal cord (better visualized on STIR sequences) due to compressive myelopathy. The patient was submitted to surgical procedure where a wine-colored lesion compressing the dural sac was observed. The lesion was completely resected with no significant complication. Anatomopathological analysis demonstrated proliferation of middle-sized vessels filled with blood, with no atypias, compatible with cavernous hemangioma. Hemangiomas are benign proliferative vascular lesions. According to the predominant type of vascular canal, hemangiomas are classified as follows: venous, arteriovenous, capillary and cavernous(1). A purely epidural hemangioma is a rare lesion, representing only 4% of epidural lesions, and the cavernous subtype is the most commonly found in this region(1). The lesion is located in the posterior region of the spine in up to 93% of cases and the dorsal spine is affected in 80% of cases(2). Epidural cavernous hemangioma is most commonly found in men (at a 2:1 ratio) aged over 40(2). Vertebral intraosseous involvement is frequent, with a prevalence of 11%(3). The clinical condition includes dorsal or lumbar pain, with signs of radiculopathy and myelopathy, and the patient is referred to undergo imaging study for suspicion of disk herniation. The clinical presentation is normally insidious, but acute clinical deterioration due to sudden increase in the lesion volume resulting from hemorrhage or venous occlusion(4). As the lesion is highly vascularized, the diagnostic suspicion is very important for the surgical planning, reducing the chances of bleeding during the procedure. Incomplete resection due to bleeding might lead to persistence of clinical symptoms and reoperation would be difficult because of local adhesions(1,4). Epidural hemangiomas are described as elongated and lobulated lesions, possibly with distinctive imaging findings depending on the subtype. Venous and arteriovenous hemangiomas present as cystic masses, generally with hypo- or intermediate signal on T1-weighted and marked hypersignal on T2-weighted images with peripheral contrast enhancement. Capillary and cavernous hemangiomas are seen as solid masses, with hypo- or intermediate signal on T1-weighted, marked hypersignal on T2-weighted images, and intense contrast-enhancement(1,4-6). The main differential diagnoses of epidural hemangiomas include nerve sheath tumor, meningioma, lymphoma, abscess and extradural hematoma(1,6-8). Finally, cavernous hemangioma should be considered in the differential diagnosis of epidural lesion with hypersignal on T2-weighted images and prominent contrast enhancement, particularly in case where the posterior region of the dorsal spine is affected. REFERENCES 1. Lee JW, Cho EY, Hong SH, et al. Spinal epidural hemangiomas: various types of MR imaging features with histopathologic correlation. AJNR Am J Neuroradiol. 2007;28:1242-8. 2. Aoyagi N, Kojima K, Kasai H. Review of spinal epidural cavernous hemangioma. Neurol Med Chir (Tokyo). 2003;43:471-5. 3. Castro DG, Lima, RP, Maia MAC, et al. Hemangioma vertebral sintomático tratado exclusivamente com radioterapia exclusiva: relato de caso e revisão da literatura. Radiol Bras. 2002;35:179-81. 4. Sanghvi D, Munshi M, Kulkarni B, et al. Dorsal spinal epidural cavernous hemangioma. J Craniovertebr Junction Spine. 2010;1:122-5. 5. Rovira A, Rovira A, Capellades J, et al. Lumbar extradural hemangiomas: report of three cases. AJNR Am J Neuroradiol. 1999;20:27-31. 6. Shin JH, Lee HK, Rhim SC, et al. Spinal epidural cavernous hemangioma: MR findings. J Comput Assist Tomogr. 2001;25:257-61. 7. Atlas SW. Magnetic resonance imaging of the brain and spine. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2008. 8. El Khamary SM, Alorainy IA. Case 100: spinal epidural meningioma. Radiology. 2006;241:614-7. 1. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brasil 2. Instituto D'Or de Pesquisa e Ensino, Rio de Janeiro, RJ, Brasil Mailing Address: Dr. Marcelo Mantiolhe Martins Rua Francisco Otaviano, 23/802, Copacabana Rio de Janeiro, RJ, Brazil, 22080-040 E-mail: marcelomantiolhe@hotmail.com |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554