Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 46 nº 1 - Jan. /Feb. of 2013
Vol. 46 nº 1 - Jan. /Feb. of 2013
|
CASE REPORT
|
|
Unilateral emphysematous pyelitis: case report |
|
|
Autho(rs): Eduardo Gonçalves1; Bruna Tupinambá Maia2; Camila Matos Versiani2; Cristiane Turano Mota3; Augusto Gonçalves Santos Filho3 |
|
|
Keywords: Emphysematous pyelitis; Complicated urinary tract infection; Computed tomography. |
|
|
Abstract: INTRODUCTION
Gas-forming renal infections are classified into two major groups. The first one includes those infections which involve only the pyelocaliceal system - emphysematous pyelitis-, while the other group includes renal parenchyma injuries, either sparing or not the collecting system(1,2). Emphysematous pyelitis is a benign condition with lower mortality rates as compared with emphysematous pyelonephritis. Thus, the distinction between such conditions is of paramount relevance, considering the significant differences related to prognosis and clinical management of each of these diseases(3). The present report describes a case of unilateral emphysematous pyelitis documented by abdominal computed tomography (CT) and laboratory tests. CASE REPORT A 22-year-old, female patient was admitted into the hospital emergency department presenting acute lumbar pain at right, dysuria, chills, recurrent vomiting not related to feeding, temperature of 38.5ºC and bladder fullness > three hours, followed by small volume overflow micturition. The patient reported use of norfloxacin (400 mg), ciprofloxacin (500 mg) and levofloxacin (500 mg) every 12 hours as an empirical treatment for cystitis. At clinical examination, the patient demonstrated to be restless, oriented and afebrile. Vital signs showed heart rate of 78 bpm; respiratory rate of 17 breaths per minute and arterial pressure of 100 × 70 mmHg. The cardiovascular, respiratory and digestive systems were unaltered. Giordano's maneuver was positive. Uroculture + antibiogram and routine urinalysis were requested, demonstrating urinary tract infection by Gram-negative bacteria Escherichia coli (> 1,000,000 UFC). Resistance to nalidixic acid, ampicillin norfloxacin and ofloxacin was demonstrated. Laboratory tests results revealed: urea levels 39 mg/dl, creatinine levels 0.9 mg/dl, and glycemic levels 80 mg/dl. Global leukocyte count was 8.400/mm3, with 62% neutrophils, 29% lymphocytes, and 6% monocytes. Additionally, abdominal CT was performed and demonstrated a slight increase in size of the right kidney in association with pyelocaliceal dilation, presence of innumerable calculi and gas foci in the renal pelvic calices (Figure 1). Also, a delay was observed in the concentration and elimination of the contrast medium, determining the finding of striated nephrogram (Figure 2), as well as rotational anomaly of both kidneys (Figure 3). The left kidney and other organs were unaltered, but the presence of gas foci in the right collecting system determines emphysematous pyelitis caused by Gram-negative bacteria. 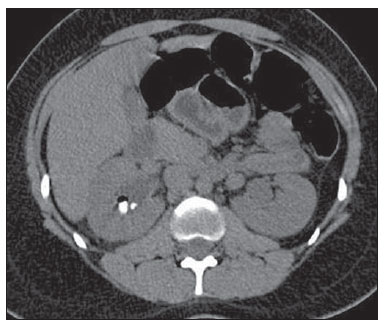 Figure 1. Contrast-enhanced whole abdomen CT, nephrographic phase. Subtle increase in renal size and pyelocaliceal dilation at right, besides innumerable calculi and gas foci in the ipsilateral collecting system. Striated nephrogram. 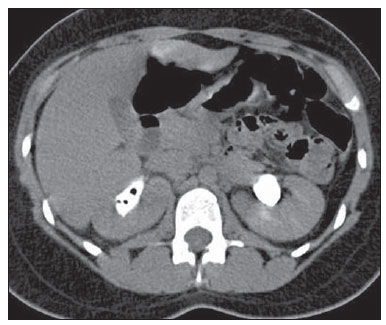 Figure 2. Whole abdomen excretory phase CT. Pyelocaliceal dilation and delayed uptake and elimination of contrast medium at right. Persistent presence of gas foci in the collecting system. 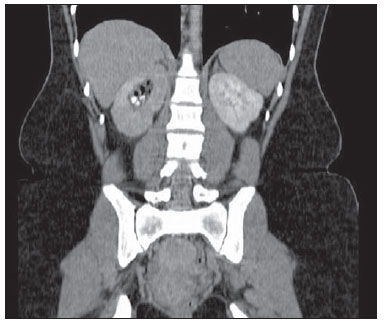 Figure 3. Rotation anomaly of both kidneys, without lower poles fusion, as well as delayed contrast uptake and striated nephrogram at right. Presence of gas foci in the calices and renal pelvis at right, associated with numerous calculi. The therapeutic approach included intravenous antibiotic therapy with levofloxacin (500 mg) for five days, and N-butylscopolamine (20 mg) to alleviate the symptoms. At the fifth day, the patient was clinically stable and asymptomatic and was discharged. Maintenance of oral antimicrobial therapy was prescribed for the seven subsequent days. For diagnostic confirmation, the patient underwent a CT scan at the 15th day after the treatment initiation. Such scan demonstrated a significant resolution of the emphysematous process (Figure 4). 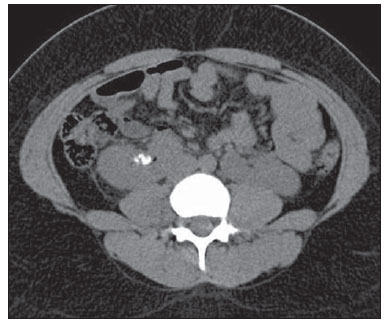 Figure 4. CT performed 15 days after the treatment initiation. Presence of a small, residual gas focus and persistence of calculi. DISCUSSION Emphysematous pyelitis is a rare urinary tract infection caused by gas-forming bacteria. The condition is generally benign, but may be worsened in cases of late diagnosis, which favors the involvement of the renal parenchyma(4). Usually, the course of this disease develops with the same symptoms of urinary tract infections, and may either be or not be associated with obstructive phenomena, whose main cause is lithiasis(2,5), which was present in this patient. The diagnosis of urinary tract infection is based on the findings of routine urinalysis and uroculture associated with the patient's symptoms(4,6). On the other hand, the identification of its emphysematous variant requires imaging methods, particularly ultrasonography (US) and CT. US may be misleading, giving gas collections an appearance of calculi. However, at a careful analysis, one can observe that the posterior acoustic shadowing produced by the gas is "dirty" as compared with the shadowing produced by calculi. Usually, calculi produce a strong and clean acoustic shadow(1,2,7). CT is the method of choice for detecting gas foci in the urinary tract, also allowing a better visualization of calculi, obstructions and anatomic deformities. Furthermore, this method is useful in the differentiation between emphysematous pyelitis and emphysematous pyelonephritis, since such conditions correspond to different prognoses and require different clinical follow-up(1,2,8). Finally, the present case report highlights the occurrence of emphysematous pyelitis as a possible complication from urinary tract infection. Also, the authors highlight that, according to the literature, CT has proven to be a useful imaging method to investigate such complication. Thus, thanks to early diagnosis, it is possible to establish an appropriate management strategy varying according to the clinical severity of the condition and reducing the rate of complications and mortality resulting from this disease. REFERENCES 1. Srinivasan S, Teh HS, Clarke MJ. Clinics in diagnostic imaging (138). Emphysematous pyelitis. Singapore Med J. 2012;53:214-7. 2. Kua CH, Abdul Aziz Y. Air in the kidney: between emphysematous pyelitis and pyelonephritis. Biomed Imaging Interv J. 2008;4:e24. 3. Roy C, Pfleger DD, Tuchmann CM, et al. Emphysematous pyelitis: findings in five patients. Radiology. 2001;218:647-50. 4. Nishiura JL, Heilberg IP. Infecção urinária. RBM. 2009;66:5-12. 5. Derouiche A, El Attat R, Hentati H, et al. Emphysematous pyelitis: epidemiological, therapeutic and evolutive features. Tunis Med. 2009;87:180-3. 6. Campos FA, Rosas GQ, Goldenberg D, et al. Freqüência dos sinais de pielonefrite aguda em pacientes submetidos a tomografia computadorizada. Radiol Bras. 2007;40:309-14. 7. Nabi Z, Almukdad H, Alnassri A, et al. Gas-forming urinary tract infection. J Coll Physicians Surg Pak. 2008;18:652-4. 8. Sakate M, Sakate ATY, Yamashita S, et al. Tomografia computadorizada de abdome normal: estudo retrospectivo das angulações dos hilos renais. Radiol Bras. 2009;42:27-9. 1. Master, Assistant Professor, Department of Women's and Children's Health /CCBS/Unimontes and Course of Graduation in Medicine, Faculdades Integradas Pitágoras (FIPMoc), Montes Claros, MG, Brazil. 2. Graduation in Medicine, Faculdades Integradas Pitágoras (FIPMoc), Montes Claros, MG, Brazil. 3. Titular Members of Colégio Brasileiro de Radiologia e Diagnóstico por Imagem (CBR), Radiologists, Grupo Ressonar, Montes Claros, MG, Brazil. Mailing Address: Bruna Tupinambá Maia Rua Doutor Veloso, 1018, ap. 502, Centro Montes Claros, MG, Brazilo, 39400074 E-mail:bruna.btm@hotmail.com Received September 13, 2012. Accepted after revision November 5, 2012. * Study developed at Faculdades Integradas Pitágoras (FIP-Moc), Montes Claros, MG, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554