Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 4 - July / Aug. of 2012
Vol. 45 nº 4 - July / Aug. of 2012
|
CASE REPORT
|
|
Osteomyelitis of the wrist in a patient with disseminated paracoccidioidomycosis: a rare presentation |
|
|
Autho(rs): Juliana Santos Bayerl1; André Ribeiro Nogueira de Oliveira2; Paulo Mendes Peçanha3; Aloísio Falqueto4 |
|
|
Keywords: Paracoccidioidomycosis; Endemic mycosis; Osteomyelitis. |
|
|
Abstract: INTRODUCTION
Paracoccidioidomycosis is the most common endemic systemic mycosis in Latin America(1,2). Such condition is acquired by inhalation of infected particles which reach the lungs, developing primary infection. In the early stages of the disease, the patient does not develop any symptom or otherwise present subtle and nonspecific symptoms. As the disease progresses, the patient presents severe involvement of several organs such as skin, mucosas, lungs and bones. Such an infection may progress with dissemination, but the disseminated presentation occurs in only 3-5% of cases.(3) The present report is aimed at evaluating bone changes observed on imaging studies of a patient with osteomyelitis of the wrist secondary to disseminated paracoccidioidomycosis, as a contribution to the early diagnosis and treatment of this disabling disease. CASE REPORT A male, 59-year old patient who as agricultural worker and with a long history of smoking attended an emergency unit in the city of Vitória, ES, Brazil, reporting progressive dyspnea for three months, ulcerative lesions on his skin and mucosas in association with pain and soft tissue enlargement in his right wrist, with serosanguineous secretion. Findings at physical examination included cervical and axillary lymph nodes enlargement, ulcerative lesions on the skin of his dorsal region and oral mucosa, besides a significant increase in volume of his right wrist. Chest radiography demonstrated diffuse and confluent opacities in the middle thirds of the pulmonary fields and opacities corresponding to fibrotic scars in the lung bases. Radiography of the right wrist demonstrated a subtle decrease in the bone density of the distal ulna (Figure 1A). 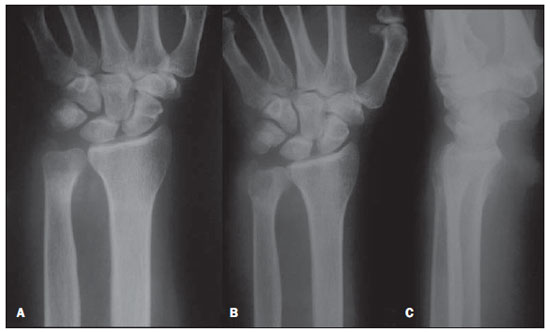 Figure 1. Plain radiograph of wrist. A: The first radiograph of the right wrist demonstrates subtle decrease in bone density of the distal ulna and preserved joint spaces. B,C: Anteroposterior and lateral radiographic images of wrist acquired one month later, clearly identify a lytic area in the distal ulna. Considering the radiographic findings, the patient was treated with antibiotics and referred to the center of infecto-parasitic diseases at Hospital Universitário Cassiano Antônio de Moraes. One month after the treatment, new radiographic images of the wrist and high resolution computed tomography (HRCT) of the chest were acquired in addition to fungal serology and cytology of the wrist secretion. The cytology revealed the presence of a high number of fungi compatible with Paracoccidioides brasiliensis. Radiography of the right wrist demonstrated a lytic area in the distal ulna (Figures 1B and 1C). The patient was submitted to magnetic resonance imaging of the wrist, which demonstrated a significant involvement of the bone marrow in the distal ulna, development of bone abscess and fistulous trajectory, with involvement of the muscle and adjacent subcutaneous tissues, with intense contrast-enhancement (Figure 2). At chest HRCT multiple consolidations were observed in the middle and lower thirds of the lungs, besides septal thickening, cavitating nodules and bronchial walls thickening (Figure 3). Technetium and gallium scintigraphy was performed, confirming the presence of active disease in the lungs and right wrist (Figure 4). Contrast uptake was not observed in other bones or in the central nervous system. 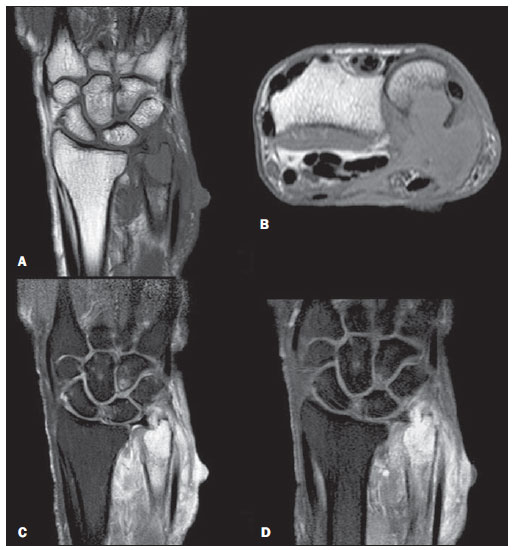 Figure 2. MRI of right wrist. A,B: Coronal and axial T1-weighted images demonstrate intermediate signal intensity in the distal ulna bone marrow, with cortical destruction and fistulous traject. C: Coronal, T2-weighted image reveals a significant bone marrow edema and extension of the infectious process towards soft tissues. D: Contrast-enhanced coronal T1-weighted image demonstrates enhancement of the bone marrow as well as of the muscle and adjacent subcutaneous tissues. 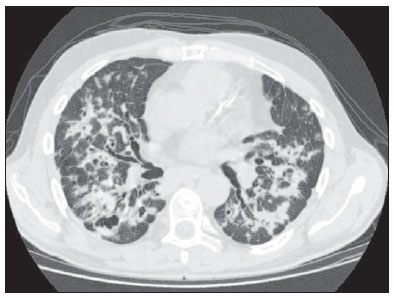 Figure 3. HRCT of chest demonstrates bilateral confluent opacities in pulmonary fields, cavitating nodules and bronchial walls thickening. 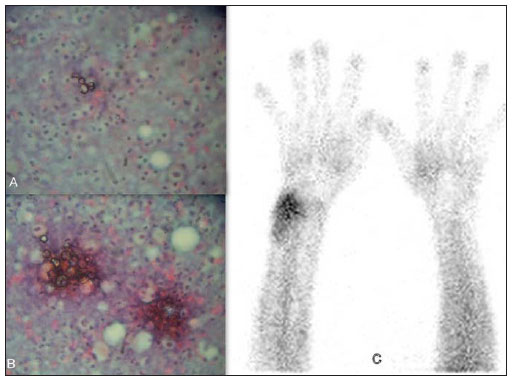 Figure 4. Scintigraphy and cytology of right wrist. A,B: Cytology of the right wrist secretion demonstrates the presence of a high number of fungi compatible with Paracoccidioides brasiliensis. C: Significant radiopharmaceutical uptake in the distal wrist, indicating the presence of active disease. The patient was admitted and initially treated with Amphotericin B. After improvement of the respiratory symptoms and decrease in volume of soft tissue components in his right wrist, the patient was discharged with sulfamethoxazole-trimetropim, remaining under regular follow-up on an outpatient basis. DISCUSSION Paracoccidioidomycosis affects primarily adult individuals in their most productive phase, causing high social and economic impact. More than 90% of cases occur in male individuals(1,4), representing a relevant public health problem because of its high disabling potential and high mortality in cases of disseminated disease(4,5). Accurate epidemiological data on the disease are not available in Brazil, since Brazilian regulations do not require mandatory notification(6). Paracoccidioidomycosis may manifest in several organs, particularly in lungs, skin, mucosas and lymph nodes. Lungs are most commonly affected(7), with radiographic changes in 60% of acute cases and in up to 80% of chronic cases(8). Small opacities constitute the most common pulmonary findings, generally with bilateral and symmetric distribution of the lesions(4). Bones involvement is extremely rare.(3,9-11) The typical finding is a well-defined lytic area, either with or without a sclerotic halo that may be observed in any bone, either with or without involvement of soft tissues. The disease is generally multifocal. Differential diagnoses include other infectious diseases such as chronic bacterial osteomyelitis, tuberculosis and primary or metastatic tumors such as lymphoma and osteosarcoma. The disease location is determined by hematogenous dissemination. It was first described by Pereira and Vianna in 1911, in a case with multiple bone lesions affecting the sternum, ribs, skull, tibia, sternoclavicular joint and shoulder. Few cases of single bone involvement are reported in the literature. In many cases, osteomyelitis secondary to paracoccidioidomycosis is a late diagnosis, resulting in high morbidity and mortality. Imaging studies are useful to evaluate the disease extent. Suspicious areas must be radiologically investigated. Bone scintigraphy can assess the whole body. Gallium scintigraphy can detect inflammatory activity. Therefore, the identification of imaging findings in cases of osteomyelitis secondary to paracoccidioidomycosis is extremely relevant for early diagnosis and treatment, reducing morbidity. REFERENCES 1. Shikanai-Yasuda MA, Telles Filho FQ, Mendes RP, et al. Consenso em paracoccidioidomicose. Rev Soc Bras Med Trop. 2006;39:297-310. 2. Souza AS Jr, Gasparetto EL, Davaus T, et al. Highresolution CT findings of the 77 patients with untreated pulmonary paracoccidioidomycosis. AJR Am J Roentgenol. 2006;187:1248-52. 3. Pereira GH, Santos AQ, Park M, et al. Bone marrow involvement in a patient with paracoccidioidomycosis: a rare presentation of juvenile form. Mycopathologia. 2010;170:259-61. 4. Moraes CS, Queiroz-Telles F, Marchiori E, et al. Análise das alterações radiográficas pulmonares durante a terapêutica da paracoccidioidomicose. Radiol Bras. 2011;44:20-8. 5. Coutinho ZF, Silva D, Lazera M, et al. Paracoccidioidomycosis mortality in Brazil (1980-1995). Cad Saúde Pública. 2002;18:1441-54. 6. Martinez R. Paracoccidioidomycosis: the dimension of the problem of a neglected disease. Rev Soc Bras Med Trop. 2010;43:480. 7. Muniz MAS, Marchiori E, Magnago M, et al. Paracoccidioidomicose pulmonar - aspectos na tomografia computadorizada de alta resolução. Radiol Bras. 2002;35:147-54. 8. Tobón AM, Agudelo CA, Osorio ML, et al. Residual pulmonary abnormalities in adult patients with chronic paracoccidioidomycosis: prolonged follow-up after itraconazole therapy. Clin Infect Dis. 2003;37:898-904. 9. Fulciniti F, Troncone G, Fazioli F, et al. Osteomyelitis by Paracoccidioides brasiliensis (South American blastomycosis): cytologic diagnosis on fine-needle aspiration biopsy smears: a case report. Diagn Cytopathol. 1996;15:442-6. 10. Krivoy S, Belfort EA, Mondolfi A, et al. Paracoccidioidomycosis of the skull. Case report. J Neurosurg. 1978;49:429-33. 11. Nogueira SA, Guedes AL, Wanke B, et al. Osteomyelitis caused by Paracoccidioides brasiliensis in a child from the metropolitan area of Rio de Janeiro. J Trop Pediatr. 2001;47:311-5. 1. MD, Resident in Radiology and Imaging Diagnosis, Universidade Federal do Espírito Santo (UFES), Vitória, ES, Brazil. 2. Nuclear Physician, CMEN - Centro de Medicina Nuclear, Preceptor of Radiology and Imaging Diagnosis, Universidade Federal do Espírito Santo (UFES), Vitória, ES, Brazil. 3. Fellow Master Degree, Associate Professor, Universidade Federal do Espírito Santo (UFES), Vitória, ES, Brazil. 4. PhD, Associate Professor, Universidade Federal do Espírito Santo (UFES), Vitória, ES, Brazil. Mailing Address: Dra. Juliana Santos Bayerl Rua José Batista, 14, Bairro Recanto Cachoeiro de Itapemirim, ES, 29303-012, Brazil E-mail: jubayerl@gmail.com Received January 4, 2012. Accepted after revision June 22, 2012. Study developed at Hospital Universitário Cassiano Antônio de Moraes - Universidade Federal do Espírito Santo (UFES), Vitória, ES, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554