Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 2 - Mar. / Apr. of 2012
Vol. 45 nº 2 - Mar. / Apr. of 2012
|
WHICH IS YOUR DIAGNOSIS?
|
|
Which is your diagnosis? |
|
|
Autho(rs): Fabiano Reis1; Lisiane Seguti Ferreira2; Guilherme Henrique Alves Vieira3 |
|
|
A female, 62-year-old patient presenting sudden onset of anterograde amnesia during 12 hours. Magnetic resonance imaging(MRI) was performed two days after the onset of the problem (Figure 1).
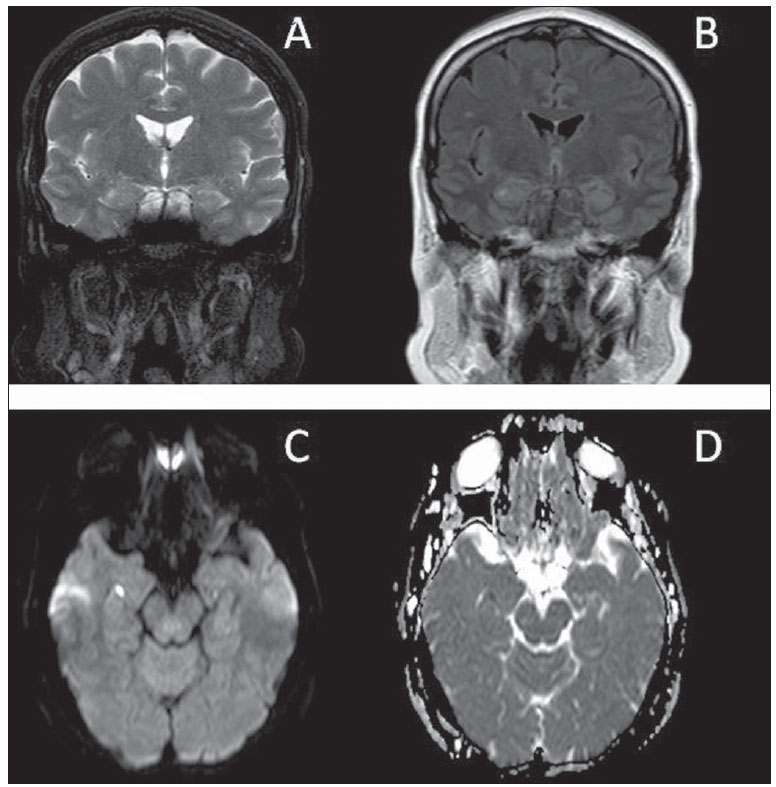 Figure 1. MRI of brain. Coronal, T2-weighted (A), FLAIR (B), diffusion-weighted (C) and ADC map (D) images. Images description Figure 1. MRI of brain. Coronal, T2- weighted image (A) demonstrates a hyperintense focus on the lateral aspect of the right hippocampus; FLAIR image (B) demonstrates a hyperintense focus on the right hippocampus; diffusion-weighted (C) demonstrates hypersignal and ADC map (D) shows hyposignal, characterizing restricted diffusion. Diagnosis: Transient global amnesia. COMMENTS The first reports on transient neurological symptoms with anterograde memory deficit were published in 1956 by Guyotat & Courjon(15). The incidence of such a condition ranges from 3 to 8 cases/100,000 people and the annual recurrence rate ranges between 6% and 10%(3). The described syndrome, called transient global amnesia (TGA), presents transient characteristics of abrupt memory loss lasting 4 to 6 hours on average, although it may persist for days, in patients with mean age of 60 years presenting predisposing factors such as an emotionally intense state and pathophysiological vascular alterations such as systemic arterial hypertension, migraine, diabetes mellitus and hypercholesterolemia/ dyslipidemia(1,2). The clinical symptoms associated with such transient memory loss are characterized by nonspecific headache of variable duration, nausea, dizziness and temporospatial disorientation. There is a direct relationship of this condition with psychiatric disorders such as depression, anxiety and post-traumatic stress disorder. It is accepted that decreased hippocampal perfusion and decrease in cortical blood flow are the pathophysiological characteristics of such syndrome(3). Venous congestion with consequential ischemia in hippocampal structures has also been associated with TGA syndrome(68). The diagnosis must be based on clinical data and corroborated by MRI studies(4). Diffusion-weighted MRI sequences demonstrate small foci of restricted diffusion, particularly on the lateral aspects of the hippocampi (Ammon's horn, CA1 region), and that may either be uni or bilateral(4). The sensitivity of diffusion MRI for detecting restricted diffusion is dependent on the length of the interval between the symptoms onset and the performance of the study(6,7). In the present case, the patient underwent MRI 48 hours after the symptoms onset, a period in which the method is quite sensitive to detect alterations(4). Such restriction to diffusion may result from different mechanisms which lead to focal energetic failure(8). The syndrome is self-limited, with spontaneous resolution after a critical period of hippocampal ischemia/hypoperfusion(2). In most of cases, MRI follow-up does not demonstrate residual alterations. REFERENCES 1. Quinette P, Guillery-Girard B, Dayan J, et al. What does transient global amnesia really mean? Review of the literature and thorough study of 142 cases. Brain. 2006;129:164058. 2. Felix MM, Castro LH, Maia AC Jr, et al. Evidence of acute ischemic tissue change in transient global amnesia in magnetic resonance imaging: case report and literature review. J Neuroimaging. 2005;15:2035. 3. Lewis SL. Aetiology of transient global amnesia. Lancet. 1998;352:3979. 4. Winbeck K, Etgen T, von Einsiedel HG, et al. DWI in transient global amnesia and TIA: proposal for an ischaemic origin of TGA. J Neurol Neurosurg Psychiatry. 2005;76:43841. 5. Guyotat J, Courjon J. Les ictus amnésiques. J Med Lyon. 1956;37:697701. 6. Godeiro-Junior C, Miranda-Alves MA, Massaro AR. Diffusion magnetic resonance imaging in transient global amnesia. Arq Neuropsiquiatr. 2009;67:1301. 7. Weon YC, Kim JH, Lee JS, et al. Optimal diffusionweighted imaging protocol for lesion detection in transient global amnesia. AJNR Am J Neuroradiol. 2008;29:13248. 8. Sander D, Winbeck K, Etgen T, et al. Disturbance of venous flow patterns in patients with transient global amnesia. Lancet. 2000;356:19824. 1. PhD, Professor, Faculdade de Ciências Médicas Universidade Estadual de Campinas (FCM-Unicamp), Campinas, SP, Brazil. 2. PhD, Associate Professor, Universidade de Brasília (UnB), Brasília, DF, Brazil. 3. Graduate Student of Medicine, Faculdade de Ciências Médicas Universidade Estadual de Campinas (FCMUnicamp), Campinas, SP, Brazil. Mailing Address: Dr. Fabiano Reis Hospital de Clínicas, Universidade Estadual de Campinas (HC-Unicamp) Rua Vital Brasil, 251, Cidade Universitária Zeferino Vaz Campinas, SP, Brazil, 13083 888 E-mail: fabianoreis2@gmail.com Study developed at Faculdade de Ciências Médicas Universidade Estadual de Campinas (FCM-Unicamp), Campinas, SP, Brazil. |
|
GN1© Copyright 2024 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554