Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 45 nº 1 - Jan. /Feb. of 2012
Vol. 45 nº 1 - Jan. /Feb. of 2012
|
WHICH IS YOUR DIAGNOSIS?
|
|
WHICH IS YOUR DIAGNOSIS? |
|
|
Autho(rs): Antônio Alberto Ferreira Barbosa1; Alberto Peters Bambirra2; Marcelo Bordalo Rodrigues3 |
|
|
A female, 66-year-old patient complaining of progressive and diffuse enlargement of the right hand index finger in association with paresthesia of the index and middle fingers over the past ten years.
Images description Figure 1. Picture of the patient's right hand showing diffuse volumetric enlargement of the index finger.  Figure 1. Picture of the hand. Figure 2. Posteroanterior radiograph of the right hand shows diffuse overgrowth of soft tissues, particularly in the radial aspect of the index finger in association with periosteal bone hypertrophy adjacent to the radial aspect of the metacarpophalangeal and distal interphalangeal joints.  Figure 2. Hand radiograph, posteroanterior view. Figure 3. MRI, axial T1-weighted sections demonstrating diffuse overgrowth of fat affecting soft tissues, highlighting the involvement of the radial palmar digital neurovascular bundle. 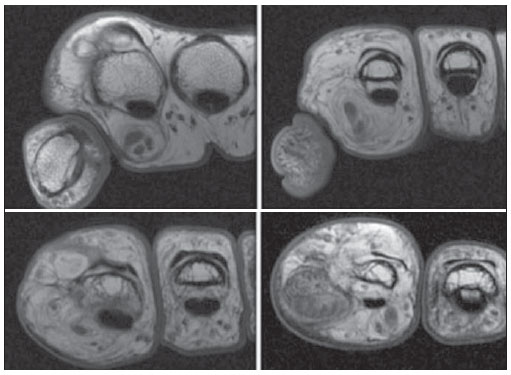 Figure 3. Magnetic resonance imaging (MRI), axial T1-weighted sections. Figure 4. MRI, coronal T1- and T2-weighted sections with fat suppression confirm the adipose nature of the soft tissue overgrowth and demonstrate the juxta-articular periosteal bone hypertrophy. 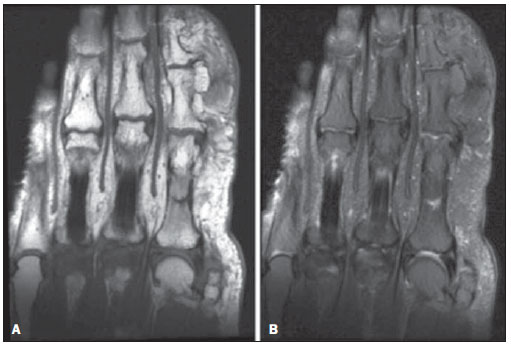 Figure 4. MRI, coronal, T1-weighted sections without fat saturation (A), and T2-weighted sections with fat saturation (B). Diagnosis: Lipomatosis of radial palmar digital nerve in right hand index finger associated with macrodactyly (macrodystrophia lipomatosa). COMMENTS Lipomatosis of nerve is a rare benign lesion characterized by anomalous growth of the neural sheath fibrofatty tissue. Its synonymia is extensive, including fibrolipomatous hamartoma of nerve, perineural lipoma, fatty infiltration of nerve, neural fibrolipoma, but, in 2002 the World Health Organization adopted the term lipomatosis of nerve for such a condition(1). Lipomatosis etiology still remains unknown and there is not hereditary predisposition for this type of lesion, although some authors believe that it is a congenital tumor while others believe it is a hamartoma whose growth is stimulated by nerve irritation or inflammation(2). Typically, patients are affected before 30 years of age, most at birth or in the childhood(1,3). The upper extremity, particularly the median nerve, is the most frequent affected, corresponding to 7896% of cases(1,3). Ulnar, radial, digital, plantar, cranial and sciatic nerves are other less affected sites. Clinical manifestations include slow-growing mass affecting mainly the wrist or hand, sometimes with symptoms related to compressive neuropathy of the median nerve in the carpal tunnel. The typical histological finding is the thickening of nerve fascicles intermingled with fatty infiltration (mature adipocytes), endo- and perineural fibrosis(4). Macrodactyly, as observed in the present case, is found in approximately 2767% of patients with lipomatosis of nerve, but the term lipomatosis of nerve either with or without macrodactyly is preferred by some authors(1,5). It is a rare, congenital and non-hereditary form of localized gigantism characterized by growth of all mesenchymal elements in the distribution of a specific nerve, with fibrofatty tissue(1), in the present case, in the distribution of the radial palmar digital nerve (Figure 3). In cases of macrodystrophia lipomatosa, the involvement of the nerve is most frequent in female patients and preferably affects the index and middle fingers(1,6), corresponding to the region the median nerve innervation, which in most cases is affected by the disease. Although macrodactyly is generally detected at birth, patients usually seek medical assistance belatedly, mainly for aesthetic reasons or in cases where there are secondary degenerative changes causing functional limitation(4). In macrodystrophia lipomatosa, the striking pathological finding is the growth of fibrofatty tissue, involving the bone marrow, periosteum, muscles, nerve sheaths and subcutaneous tissue. In cases of association of fibrolipomatous hamartoma with macrodystrophia lipomatosa, the causal relationship is not well established(4). MRI findings resembling a "coaxial cable" are considered pathognomonic for the diagnosis of fibrolipomatous hamartoma(2). The thickened nerve fascicles are homogeneously distributed over the nerve sheath and present low signal intensity on T1- and T2-weighted sequences. Homogeneous fat infiltration between nerve fascicles is seen with high signal intensity on T1- and low signal intensity on T2-weighted images with fat suppression. Imaging findings of macrodystrophia lipomatosa at plain radiography include increase in volume of bone structures and soft tissues, most prominently at the distal extremity and ventral aspect of the affected limb, besides periosteal involvement, particularly juxta-articular involvement (Figure 2)(1,6,7). Radiolucent areas reflecting overgrowth of fatty tissue are generally detectable on soft tissues. The phalanges may be elongated and widened. At MRI, the diffuse overgrowth of fatty contents in the soft tissues is defined (Figures 3 and 4). Neurofibromatosis type 1 is the main differential diagnosis for macrodystrophia lipomatosa(4). From the clinical aspects standpoint, neurofibromatosis differs from macrodystrophia lipomatosa for being hereditary, for being associated with café-au-lait skin spots, and for sometimes occurring bilaterally and with involvement of non-contiguous fingers. At imaging studies, neurofibromatosis does not present radiolucent soft tissues (adipose tissue) and presents neurofibromas which are detected as nodular areas with increased signal intensity on MRI T2-weighted images. Other differential diagnoses for macrodactyly include Klippel-Treanunay-Weber syndrome, hemangiomatosis and lymphangiomatosis(1,4). REFERENCES 1. Murphey MD, Carroll JF, Fleming DJ, et al. From the archives of the AFIP. Benign musculoskeletal lipomatous lesions. Radiographics. 2004;24:143366. 2. Marom EM, Helms CA. Fibrolipomatous hamartoma: pathognomonic on MR imaging. Skeletal Radiol. 1999;28:2604. 3. Blacksin M, Barnes FJ, Lyons MM. MR diagnosis of macrodystrophia lipomatosa. AJR Am J Roentgenol. 1992;158:12957. 4. Coelho RDS, Simão MN, Trad CS. Hamartoma fibrolipomatoso e macrodistrofia lipomatosa: análise dos achados clínicos e de imagem em quatro casos, com revisão da literatura. Radiol Bras. 2002;35:28791. 5. Murphey MD, Smith WS, Smith SE, et al. From the archives of the AFIP. Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. Radiographics. 1999;19:125380. 6. Goldman AB, Kaye JJ. Macrodystrophia lipomatosa: radiographic diagnosis. AJR Am J Roentgenol. 1977;128:1015. 7. Singla V, Virmani V, Tuli P, et al. Case Report: Macrodystrophia lipomatosa illustration of two cases. Indian J Radiol Imaging. 2008;18:298301. 1. MD, Resident at Instituto de Radiologia Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (InRad/HC-FMUSP), São Paulo, SP, Brazil. 2. Physician Assistant of Radiology, Instituto de Ortopedia e Traumatologia Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (IOT/HC-FMUSP), São Paulo, SP, Brazil. 3. MD, Head of Division of Musculoskeletal Radiology, Instituto de Ortopedia e Traumatologia Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (IOT/HC-FMUSP), São Paulo, SP, Brazil. Mailing Address: Dr. Marcelo Bordalo Rodrigues Avenida Doutor Eneas de Carvalho Aguiar, 255, Pinheiros São Paulo, SP, Brazil, 05403-001 E-mail: mbordalo@uol.com.br Study developed at Instituto de Ortopedia e Traumatologia (IOT) and Instituto de Radiologia (InRad) Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HC-FMUSP), São Paulo, SP, Brazil. |
|
GN1© Copyright 2025 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554