Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 44 nº 2 - Mar. / Apr. of 2011
Vol. 44 nº 2 - Mar. / Apr. of 2011
|
WHICH IS YOUR DIAGNOSIS?
|
|
Which is your diagnosis? |
|
|
Autho(rs): Marcelo Souto Nacif1; Nadine Kawel2; Christopher T. Sibley3; Anna Zavodni2; João A. C. Lima4; David A. Bluemke5 |
|
|
Forty-one year old hypertensive (African American) male patient, with a history of drug abuse for a short period at the age of 29 years, was referred to the Radiology Department at National Institutes of Health Clinical Center for evaluation by cardiac computed tomographic angiography (CTA) and cardiac magnetic resonance imaging (CMR).
Images description Figure 1. ECG-gated CMR (A,B) and CTA (C,D). Cine-CMR, two chamber view (A) and late enhancement (B). Proximal left anterior descending coronary artery (C,D). Observe marked left ventricular dilatation associated with wall thinning in the territory of the left anterior descending coronary artery related to previous infarction caused by vasospasm. Enlargement of the apical trabeculated region with calcified thrombus. CTA (C,D) demonstrating a soft plaque in the proximal left anterior descending coronary artery with positive remodeling and subtle luminal narrowing (30% stenosis). 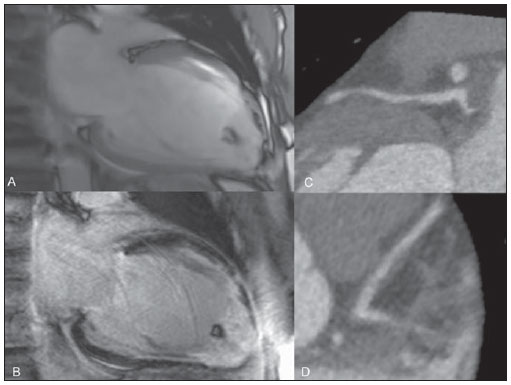 Figure 1. ECG-gated CMR (A,B) and CTA (C,D). Two chamber cine-CMR (A) and late enhancement (B). Proximal left anterior descending coronary artery (C,D). Figure 2. Tagging analysis (A,B). Strain rate (A) and mesh ejection fraction (B). Pre-contrast (C) and post-contrast (D) MOLLI T1 color maps. The tagging analysis showed poor segmental ejection fraction (base = 21.4%, midcavity = 7.7%, and apex = 2.4%), and the peak Ecc strain (%) at the base, midcavity and apex were respectively 10.6%, 5.7% and 0.6% of the average LV midwall. Pre-contrast (C) and post-contrast (D) MOLLI T1 color coded maps for visual (qualitative) analysis: in the regions of delayed gadolinium enhancement, T1 color maps demonstrate yellow color on pre-contrast and dark blue on postcontrast maps according to a longer T1 time in the pre-contrast phase and a shorter T1 time in the post-contrast phase. As the precontrast green myocardium (shorter T1 time) and the post-contrast blue myocardium (longer T1 time) are compared, regions with larger amounts of fibrous tissue and extracellular space enlargement can be differentiated. Analysis of T1 mapping: extracellular volume fraction for the myocardium at the base of the heart without late enhancement corresponded to 32%, while, in the apical region with late enhancement, it corresponded to 57%. 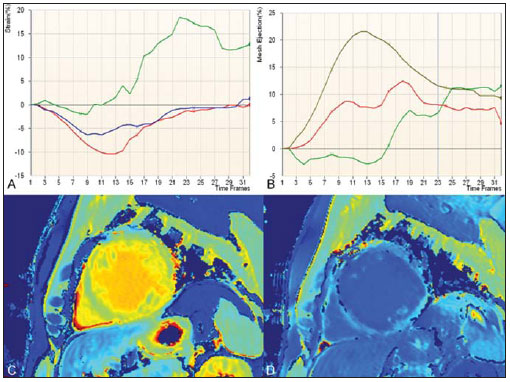 Figure 2. Tagging analysis (A,B). Strain rate (A) and mesh ejection fraction (B). Pre-contrast (C) and post-contrast (D) MOLLI T1 color maps. Background: The normal range for midwall peak Ecc strain (%) is 17.5 ± 4%(1). The extracellular volume fraction is calculated from the ratio of the myocardial relaxation rates and blood corrected by the hematocrit value: (ΔR1myocardium/ΔR1blood)*(1 Ht). Healthy volunteers assessed with the same protocol in our lab demonstrated that the normal extracellular volume fraction (± standard deviation) corresponds to 27 ± 3%. Diagnosis: Cocaine-related myocardial infarction in association with poor global strain rate and increased extracellular volume fraction calculated on T1 maps. COMMENTS Association between cocaine use and myocardial ischemia/infarction was first reported by Coleman et al. in 1989(2). Frequently, the diagnosis depends on correct information about the patients history of drug abuse. The assisting physician should be aware of the differential and try to confirm the diagnosis with blood or urine tests. The clinical history will always be difficult to assess, depending on the patients cooperation( 3). In spite of the fact that the most common form of myocardial infarction is related to the rupture of an unstable (vulnerable) atherosclerotic plaque, coronary vasospasm, either in association or not with the development of a secondary thrombus is also a potential cause for myocardial necrosis(4). Cocaine acts as a powerful sympathomimetic agent, producing central and peripheral adrenergic stimulation which induces coronary vasoconstriction that is usually related to the peak blood concentration of cocaine. However, a late effect may occur as a result of endothelial activation and the synergic prothrombotic activity, causing hypercoagulability and acute thrombus formation in the coronary vessel( 5,6). The early development of coronary atherosclerosis in chronic cocaine abusers has been reported in the literature(7,8). In the present case, a soft plaque with mild stenosis was detected in the proximal left anterior descending coronary artery. Minimal data are available to guide the evidence-based treatment of cocaine-related myocardial infarction. Usually, the treatment is clinical, with benzodiazepines, aspirin, nitroglycerin, verapamil, besides stimulus for behavioral change . However, some authors such as Sharma et al.(7) believe that a percutaneous coronary intervention at the moment of the vasospasm is the treatment of choice for such patients. In the present case, at the time of the acute precordial pain at the age of 29, the patient underwent percutaneous coronary intervention (angioplasty), and was hospitalized in a coronary care unit for three weeks. Among Americans over 12 year of age, 27.7 million, corresponding to 12% of the population, have used cocaine at some point in their lifetime; and more than 5.9 million, or 2.5% of the entire US population, have used cocaine in the last year(9,10). Cocaine use is a major public health problem worldwide and has increased in popularity in the last decades(5,8). The potential impact on the public health policies is worrisome(11). At long term, the best strategy to be adopted would be to enter patients and users into a substance abuse program to educate them about the irreversible harmful effects of cocaine on the cardiac muscle 5). We strongly support a massive public health policy to reduce the number of cocaine users and avoid the related complications. Non invasive cardiac imaging Computed tomography coronary angiography can non-invasively and accurately detect and quantify coronary plaque (12). In the present case, it was straightforward to detect the soft plaque in the proximal left anterior descending coronary artery on CTA images. Many precise software tools are available for the assessment of ventricular function using tagging(1) and diffuse or focal fibrosis with modified Lock-Locker inversion recovery (MOLLI)(1315) imaging. Cardiac magnetic resonance tagging is a powerful non-invasive diagnostic tool for quantifying regional systolic and diastolic myocardial function. Ongoing technological developments, particularly in imaging techniques, equipment and analytical tools utilized to implement CMR tagging, will improve the analyses of regional myocardial function. This will be useful for comparison and precise follow up of patients. In the present case, we could accurately assess the regional function. The quantification of fibrosis, even in cases where late enhancement images demonstrate negative results, became feasible with the T1 mapping CMR technique. The T1 time is shortened by the presence of fibrosis, and T1 mapping is a powerful tool for quantifying the extent and aggressiveness of such abnormality. The T1 mapping technique has already been validated by means of myocardial biopsies in the clinical context of patients with nonischemic fibrosis who were referred for cardiac transplant(16). Myocardial extracellular volume measurements quantify diffuse fibrosis not readily detectable by conventional late gadolinium enhancement(13,14). In the present case, we could differentiate the fibrosis detected by late enhancement on the apex of the left ventricle (high extracellular volume ECV, 57%) from the fibrosis present on the bottom of the left ventricle (high ECV, 32%) in comparison with healthy hearts (ECV = 27%). Important considerations Non-invasive studies, such as CTA and CMR are fundamental in the evaluation of subclinical atherosclerotic disease and quantification of myocardial fibrosis. Randomized, prospective studies would be extremely important to better understand these powerful techniques. REFERENCES 1. Fernandes VR, Cheng S, Cheng YJ, et al. Racial and ethnic differences in subclinical myocardial function: the Multi-Ethnic Study of Atherosclerosis. Heart. 2011;97:40510. 2. Coleman DL, Ross TF, Naughton JL. Myocardial ischemia and infarction related to recreational cocaine use. West J Med. 1982;136:4446. 3. Rao SC, Main ML. Acute severe functional mitral regurgitation secondary to cocaine-mediated anterior myocardial infarction. J Am Soc Echocardiogr. 2008;21:297.e34. 4. Kloner RA. Natural and unnatural triggers of myocardial infarction. Prog Cardiovasc Dis. 2006;48:285300. 5. Rezkalla SH, Kloner RA. Cocaine-induced acute myocardial infarction. Clin Med Res. 2007;5: 1726. 6. Raddino R, Pedrinazzi C, Zanini G, et al. Acute myocardial infarction in a young woman with antiphospholipid syndrome and occasional cocaine abuse. Int J Cardiol. 2005;105:2368. 7. Sharma AK, Hamwi SM, Garg N, et al. Percutaneous interventions in patients with cocaine-associated myocardial infarction: a case series and review. Catheter Cardiovasc Interv. 2002;56:34652. 8. Sonne C, Stempfle HU, Klauss V, et al. Intravascular ultrasound-guided percutaneous coronary intervention in a human immunodeficiency viruspositive patient with cocaine-associated acute myocardial infarction: case report and review. Heart Lung Circ. 2005;14:197200. 9. Bansal D, Eigenbrodt M, Gupta E, et al. Traditional risk factors and acute myocardial infarction in patients hospitalized with cocaine-associated chest pain. Clin Cardiol. 2007;30:2904. 10. Aslibekyan S, Levitan EB, Mittleman MA. Prevalent cocaine use and myocardial infarction. Am J Cardiol. 2008;102:9669. 11. Coombs M. Cocaine-induced myocardial infarction. Nurs Crit Care. 2007;12:17680. 12. Rinehart S, Vazquez G, Qian Z, et al. Quantitative measurements of coronary arterial stenosis, plaque geometry, and composition are highly reproducible with a standardized coronary arterial computed tomographic approach in high-quality CT datasets. J Cardiovasc Comput Tomogr. 2011;5:3543. 13. Piechnik SK, Ferreira VM, DallArmellina E, et al. Shortened Modified Look-Locker Inversion recovery (ShMOLLI) for clinical myocardial T1- mapping at 1.5 and 3 T within a 9 heartbeat breathhold. J Cardiovasc Magn Reson. 2010;12:69. 14. Schelbert EB, Testa SM, Meier CG, et al. Myocardial extravascular extracellular volume fraction measurement by gadolinium cardiovascular magnetic resonance in humans: slow infusion versus bolus. J Cardiovasc Magn Reson. 2011;13:16. 15. Messroghli DR, Radjenovic A, Kozerke S, et al. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med. 2004;52:1416. 16. Nacif MS, Noureldin RAA, Sibley CT, et al. Insuficiência cardíaca com análise de strain e caracterização de tecido fibrótico (mapa T1) [qual o seu diagnóstico?]. Radiol. Bras. 2010;43(5):xixiii. 1. MD, PhD, Professor at Radiology Department Universidade Federal Fluminense (UFF), Niterói, RJ, Brazil, Fellow of Radiology and Imaging Sciences, National Institutes of Health (NIH) Clinical Center, Bethesda, MD, USA. 2. MD, Fellow of Radiology and Imaging Sciences, National Institutes of Health (NIH) Clinical Center, Bethesda, MD, USA. 3. MD, Staff Clinician, Department of Radiology and Imaging Sciences, National Institutes of Health (NIH) Clinical Center, Bethesda, MD, USA. 4. MD, Professor at Division of Cardiology, Johns Hopkins University School of Medicine, Baltimore, MD, USA. 5. MD, PhD, Director, Department of Radiology and Imaging Sciences, National Institutes of Health (NIH) Clinical Center, Bethesda, MD, USA. Mailing Address: Dr. Marcelo Souto Nacif. Cordell Avenue 4583, 20814 Bethesda, MD, USA. E-mail: msnacif@yahoo.com.br Web site: www.msnacif.med.br Study developed at Department of Radiology and Imaging Sciences, National Institutes of Health (NIH) Clinical Center, Bethesda, MD, USA. |
|
GN1© Copyright 2024 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554