Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 44 nº 1 - Jan. /Feb. of 2011
Vol. 44 nº 1 - Jan. /Feb. of 2011
|
CASE REPORT
|
|
Newborn with urinary ascites and renal calyx rupture secondary to posterior urethral valve: sonographic diagnosis |
|
|
Autho(rs): Matteo Baldisserotto1; Humberto Fiori2; Renato Fiori2; Lucia Helena Ribeiro Ferrari3; Mariana Damian Mizerkowski4 |
|
|
Keywords: Newborn; Urinary ascites; Renal calyx rupture; Posterior urethral valve; Ultrasonography. |
|
|
Abstract: INTRODUCTION
Ascites is a rare condition in neonates and generally may present several etiologies, urinary ascites being most frequently found(1,2). In most reported cases, the urinary ascites origin is related to the presence of a posterior urethral valve, determining urinary bladder rupture and consequential ascites(3). In the medical literature review, the authors have found only one case of urinary ascites secondary to rupture of a renal calyx in a newborn with posterior urethral valve(3). In the above mentioned case, the diagnosis of such complication was achieved by means of micturating cystourethrography. The authors describe a case of urinary ascites secondary to renal calyx rupture in a newborn with posterior urethral valve, diagnosed by ultrasonography (US). CASE REPORT A male infant born by normal delivery, weighting 2,815g, with Apgar 8 and 9, respectively at the first and fifth minutes. The newborn was uneventfully discharged with 48 hours of life. At his ninth day of life, the infant came back to the emergency department because of a progressive abdominal distention that had become more noticeable in the last three days. Vomiting was not observed, only a regurgitation episode in the previous day was reported. At clinical examination, the infant presented a significant abdominal distention, CASE REPORT but the abdomen was painless at palpation and apparently with no visceromegaly. Hydro-aerial bruits were present and the fluid-wave test was positive. The prenatal mothers blood tests results were normal. Three previous obstetric US studies (at the 4th, 7th and 8th months) had not demonstrated any fetal abnormality. The mother denied consanguinity and/or diseases in her other three children. Plain abdominal radiography performed immediately after the infant admission demonstrated the presence of ascites (Figure 1). Abdominal US demonstrated massive ascites with lumps, kidneys with preserved parenchymal thickness and significant dilatation of the calyceal cavities. Additionally, such study demonstrated calyceal rupture in the upper group of the left kidney and perirenal fluid (Figure 2), a poorly filled urinary bladder with slightly thickened walls. 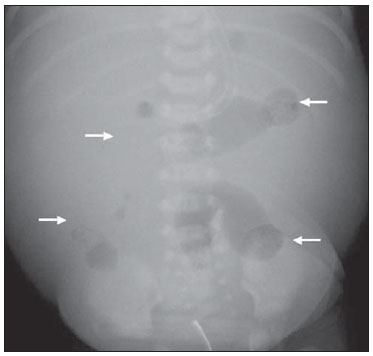 Figure 1. Plain abdominal radiography performed in dorsal decubitus, demonstrating small bowel loops centrally positioned because of massive ascites (arrows).  Figure 2. Ultrasonography demonstrates calyceal system rupture (arrows) and perirenal fluid extravasation (arrowheads). Then, the patient was submitted to micturating cystourethrography that demonstrated a urinary bladder with normal capacity, trabeculae and pseudodiverticula. Grade V vesicoureteral reflux was observed at left, represented by significant dilatation of the left sided calyceal system and ureter (Figures 3A and 3B). Contrast mean extravasation into the left peripheral space was observed with accumulation next to the upper pole of the kidney and subsequent extravasation into the peritoneal cavity. Posterior urethral dilation was observed (Figure 3B). Right-sided vesicoureteral reflux was not seen. 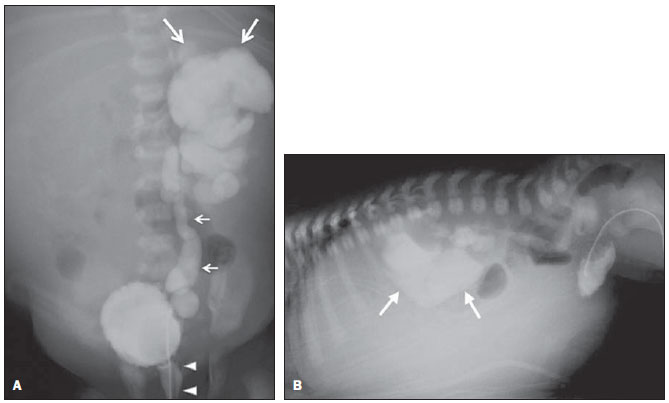 Figure 3. A: Micturating cystourethrography demonstrates massive reflux (small arrows), contrast agent extravasation into the perirenal space (large arrows) and posterior urethra dilation with abrupt caliber transition caused by the urethral valve (arrowheads). B: Micturating cystourethrography with the patient positioned in ventral decubitus provides a better visualization of the perirenal extravasation predominating in an anterosuperior site (arrows). The infant was submitted to bilateral cutaneous ureterostomy and cystoscopy. The patient was discharged in good general conditions, with weight gain, and normal blood count and electrolyte levels. DISCUSSION Ascites is a rare condition in neonates, with different causes such as problems of biliary nature, liver, heart, chylous, infectious, urinary diseases, or even a condition of unknown nature(37). Thus, the establishment of a correct diagnosis may be challenging, and many times it is defined by imaging studies such as micturating cystourethrography, US and Tc-99m scintigraphy. The establishment of an accurate diagnosis of the cause and complications of the disease is critical for the definition of a correct management and a favorable clinical progression. Amongst the above mentioned causes, urinary nature is one of the most frequently observed. The cases of urinary ascites reported in the medical literature are generally related to bladder rupture secondary to the presence of a posterior urethral valve in boys(14). Such diagnosis is achieved after extensive investigation and defined by micturating cystourethrography(1). In the medical literature review, the authors have found only one case report describing urinary ascites with renal calyx rupture secondary to the presence of a posterior urethral valve, where the diagnosis was defined by means of micturating cystourethrography(3). The original character of the present case is corroborated by the fact that the ascites was secondary to renal calyx rupture and the diagnosis was achieved by US. As a conclusion, in cases of neonatal urinary ascites caused by renal calyx rupture, US can demonstrate the rupture directing the investigation towards a specific imaging method in this case, micturating cystourethrography. REFERENCES 1. Griscom NT, Colodny AH, Rosenberg HK, et al. Diagnostic aspects of neonatal ascites: report of 27 cases. AJR Am J Roentgenol. 1977;128:9619. 2. Huang CJ, Cheng YR. Urinary ascites in young infants report of 9 cases. J Singapore Paediatr Soc. 1990;32:1214. 3. Ahmed S, Borghol M, Hugosson C. Urinoma and urinary ascites secondary to calyceal perforation in neonatal posterior urethral valves. Br J Urol.1997;79:9912. 4. Scott TW. Urinary ascites secondary to posterior urethral valves. J Urol. 1976;116:8791. 5. Haller JO, Condon VR, Berdon WE, et al. Spontaneous perforation of the common bile duct in children. Radiology. 1989;172:6214. 6. Runyon BA. Bacterial infections in patients with cirrhosis. J Hepatol. 1993;18:2712. 7. Clarke HS Jr, Mills ME, Parres JA, et al. The hyponatremia of neonatal urinary ascites: clinical observations, experimental confirmation and proposed mechanism. J Urol. 1993;150(2 Pt 2):77881 1. PhD, Associate Professor at School of Medicine of Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), MD, Radiologist at Hospital São Lucas, Porto Alegre, RS, Brazil. 2. PhDs., Associate Professors, Department of Pediatrics, Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil. 3. MD, Pediatric Gastroenterologist, Fellow Master degree, Course of Post-Graduation in Pediatrics and Child Health at Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil. 4. MD, Radiologist at Hospital São Lucas, Fellow Master degree, Course of Post-Graduation in Pediatrics and Child Health at Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil. Mailing Address: Dr. Matteo Baldisserotto. Avenida Luiz Manoel Gonzaga, 58, ap. 1201, Petrópolis. Porto Alegre, RS, Brazil, 90470-280. E-mail: matteob@terra.com.br Received June 5, 2010. Accepted after revision October 1, 2010. * Study developed at Hospital São Lucas Pontifícia Universidade Católica do Rio Grande do Sul (PUCRS), Porto Alegre, RS, Brazil. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554