Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 5 - Sep. / Oct. of 2007
Vol. 40 nº 5 - Sep. / Oct. of 2007
|
RADIOLOGY UPDATE
|
|
Use of FDG-PET/CT scan in the planning of radiation therapy for non-small cell lung cancer |
|
|
Autho(rs): Sergio L. Faria, Robert Lisbona, Jerry Stern, Slobodan Devic, Luis Souhami, Carolyn R. Freeman |
|
|
Keywords: Radiotherapy, PET scan, Planning, Lung cancer |
|
|
Abstract:
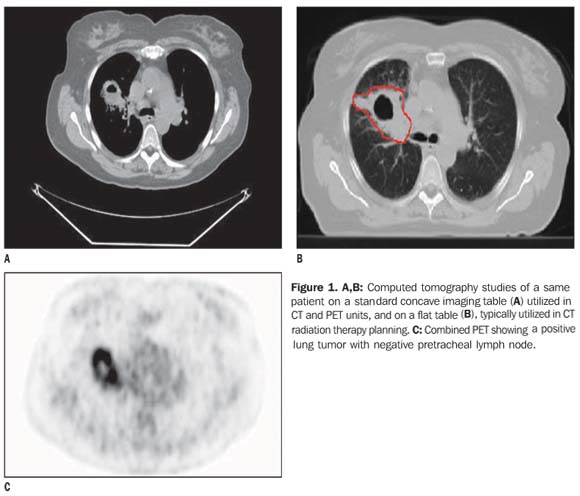
INTRODUCTION Radiation therapy (RT) is frequently utilized with curative purposes in cases of lung cancer. A probable complication of this treatment is actinic pneumonitis, since the radiation dose required to eradicate cancer (> 50 Gy) is usually higher than the dose tolerated by the lungs (around 20 Gy)(1). In radiation therapy for non-small cell lung cancer (NSCLC), the target volume has no longer been the whole mediastinum, but only the areas of tumor involvement(2). As a result, the radiation dose can be increased on the tumor without increasing the toxicity on the normal tissues. How to know which are the areas affected by a tumor? The definition of the areas of tumor involvement may come from the results of invasive procedures such as mediastinoscopy, although usually it depends on radiological studies, particularly computed tomography (CT). In the planning of radiation therapy, it may be difficult to accurately define the gross tumor volume (GTV). In some cases, a cancer cannot be differentiated from an equally dense non-tumor like areas on CT, for example, athelectasis or normal regions on the mediastinum. This difficulty can explain the significant interobserver variation in radiotherapy fields delineation in cases of lung cancer (3). A functional imaging study, like FDG-PET scan that can distinguish a cancer from other equally dense, non-tumor like areas on CT scans, meets the radiotherapist's need of a biological target to be defined. Recent studies demonstrate that the utilization of combined FDG-PET/CT changes significantly about 50% of the plannings based on CT alone(4,5), and suggest that combined FDG-PET/CT should be routinely utilized in cases of curative radiation therapy for NSCLC(6). For the last two years, the McGill University Department of Radiation Oncology has been operating in association with the Department of Nuclear Medicine, utilizing a PET/CT equipment adapted for radiation therapy planning. The present study is aimed at discussing aspects connected with the implementation of combined FDG-PET/CT in the planning of radiation therapy, and, particularly, in the definition of GTV in patients with NSCLC. PET/CT versus PET alone FDG-PET scan is used as the acronym for positron emission tomography with 18F-fluorodeoxyglucose (18FDG) as a tracer. The study detects the increased metabolism of glucose that usually is higher in malignant tumors as compared with normal tissues. As a functional imaging study, FDG-PET is limited as compared with CT to demonstrate anatomic locations. Modern PET equipment are currently available in combination with CT, with the advantage that both studies (PET and CT) require only one visit of the patient to the clinic and are performed one immediately after the other, while the patient lies in the same position on the imaging table. CT is utilized for attenuation correction and better localization of small lymph nodes or non-tumor like soft tissues. Although there is no "significant evidence" justifying the use of combined PET/CT instead of PET alone, like in other radiotherapy technical aspects, it is difficult not accepting the irreversibility of the use of combined PET/CT (7). Imaging table and patient positioning Figure 1 shows two CT images of a same patients: the first one acquired with the patient on a concave imaging table, and the second one, with the patient on a flat table, with the arms up, the typical position during radiotherapy sessions. This is the first difficulty to be overcome: standard PET/CT equipment come from the manufacturer with concave imaging tables. On the other hand, RT treatment is delivered by equipment with flat tables, with patients with their arms up in order to allow the use of lateral fields. Therefore, combined PET/CT scan for RT planning purposes should also be performed on a flat imaging table. Besides, the examination room should have the same facilities found in the radiotherapy treatment room (including a laser alignment system for isocenter setup, etc.). This is a paramount condition to allow an appropriate fusion between PET/CT images and simulation CT images utilized in the radiotherapy planning, and that the patient positioning can be adequately reproduced in the different examination and radiotherapy rooms.
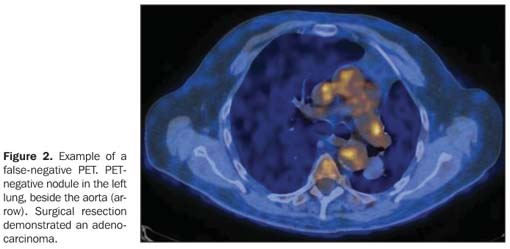
PET may yield false results There are many studies demonstrating FDG-PET is better than CT alone for lung cancer detection, and so it is useful to define the tumor extent; but PET is not an accurate method(8,9). Figure 2 shows an example of a false-negative PET. A pulmonary nodule clinically suggestive of malignant neoplasm had not shown any hypermetabolism on PET, but a surgical resection confirmed an adenocarcinoma.
Table 1 demonstrates the comparison between CT and FDG-PET sensitivities and specificities in patients with NSCLC-type lung cancer(8). One can see that FDG-PET is better than CT for cancer detection, but there is still a 10-20%- risk of false-negative or false-positive results with FDG-PET. This is a relevant information because patients referred for curative radiotherapy treatment have not been submitted to surgery, and, therefore, there is no histological confirmation of imaging findings, and it is a radiotherapist responsibility to define the target volume (GTV). Figure 1 illustrates such difficulty, with a clinically inoperable smoker patient presenting with hemoptysis, whose CT demonstrated a tumor-like mass in the right lung and mediastinal lymph nodes, besides a 2.0 cm tracheal lymph node. CT showed this lymph node as positive for cancer. Needle biopsy demonstrated that the pulmonary tumor was an adenocarcinoma. Pretreatment FDG-PET scan was positive for the pulmonary tumor, and negative for the mediastinal lymph nodes. Considering that the tracheal lymph node could not be considered as cancer without a histological study, it was impossible to know whether the mediastinal lymph node should or not be included in the GTV. In this case, a mediastinoscopy demonstrated that, despite increased in size, the lymph node was benign.
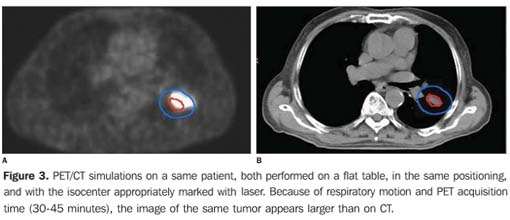
Images acquisition time and motion artifacts Tumors and thoracic organs move as a result of respiratory motion(10). With the currently available FDG-PET/CT equipment, the CT acquisition time is short (measured in seconds), but the PET acquisition time is longer (about 30-45 minutes). So, a tumor visualized on CT reflects only one position during respiratory motion whereas the PET images show the whole area of this movement. Figure 3 illustrates this difference. Considering that radiotherapy sessions take some minutes, maybe the adoption of the volume shown by PET would be more appropriate than the one shown by the simulation CT.
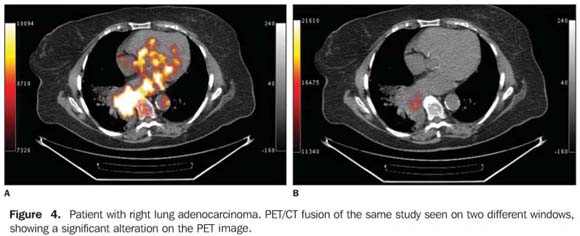
Tumor extent evaluation by FDG-PET Finally, a case where the PET/CT scan was performed with the patient on a flat imaging table, with arms up, with appropriate marking for fusion with simulation CT images, and positive (hyperactive) areas disclosed by PET included in the GTV contour. The radiotherapist has only to define the target volume to be treated. Unfortunately, the size of the hyperactive area detected by PET scan changes significantly, depending on the window selected, as shown on Figure 4.
Studies in the literature report different methods utilized to define GTV by means of FDG-PET: a) Visual method, without any grounding in physics or mathematics, simply based on visual comparison between images by the radiologist. This method was reported in the first studies on the utilization of PET for radiotherapy planning purposes(11). b) A percentage of the highest hypermetabolic value (the threshold) defines the tumor margins. Based on simulations, a threshold of 40% has been adopted(12,13). This contour may be automatically calculated by a relatively simple software. Unfortunately, one cannot guarantee that areas with a threshold lower than 40% are free from active cancerous cells; this is usual in necrotic areas, for example. c) A certain standard uptake value (SUV) will define the tumor volume; for example, a SUV higher than 2.5 that is considered by the majority of nuclear medicine specialists as an activity probably positive for NSCLC(9). Also by this method, a software can automatically calculate the tumor volume, but one cannot guarantee that areas with SUV < 2.5 are free from cancerous cells. A definition on which would be the best method to define GTV by means of FDG-PET is still to be known. What should be done? Considering the absence of a consensual guidance about this matter, the recommendation is that all of the factors must be taken into consideration in a GTV delimitation, and the clinical common sense should be adopted for each case individually(14). Recently, the Radiation Therapy Oncology Group (RTOG) initiated the study RTOG-0515 called "A comparative study of gross tumor volume definition with or without PET fusion for patients with NSCLC". This study is aimed at determining the impact of PET/CT fusion on the GTV delimitation as compared with CT. Considering the limitations of PET in the definition of tumor margins, this protocol establishes that "the tumor volume (primary tumor and lymph nodes) contour should be based only on the CT images from PET/CT studies".
CONCLUSION There is no imaging method with 100% sensitivity and specificity for lung cancer. Therefore, besides clinical information, the radiotherapist depends on the imaging methods available to define and delineate tumor margins, and CT remains as the method most frequently utilized for treatment purposes. FDG-PET/CT has shown higher sensitivity and specificity in the determination of lung cancer extent. For some experts, FDG-PET is essential in the planning of radiation therapy in patients with NSCLC; for others, the FDG-PET/CT value as a clinical tool has been overestimated(7). Although the role of FDG-PET/CT in the optimization of radiotherapy is controversial(8,9), it seems there is no doubt that this is an extremely useful imaging method for evaluating tumors extent, and, also, delimiting GTV in patients with NSCLC. Presently it is still to be established if FDG-PET-based radiotherapy planning will improve treatment outcomes and/or quality of life of patients affected by NSCLC. Positron emission tomography (PET) performed with 18F-fluorodeoxyglucose (FDG) represents a significant first step towards the application of this technique in oncology. Other tracers have been studied, representing promising alternatives for cancer diagnosis and staging, as well as in the planning of radiation therapy.
REFERENCES 1. Emami B, Lyman J, Brown A, et al. Tolerance of normal tissue to therapeutic radiation. Int J Radiat Oncol Biol Phys 1991;21:109–122. [ ] 2. Rosenzweig KE, Sim SE, Mychalczak B, Braban LE, Schindelheim R, Leibel SA. Elective nodal irradiation in the treatment of non-small-cell lung cancer with three-dimensional conformal radiation therapy. Int J Radiat Oncol Biol Phys 2001; 50:681–685. [ ] 3. Hamilton CS, Denham JW, Joseph DJ, et al. Treatment and planning decisions in non-small cell carcinoma of the lung: an Australasian patterns of practice study. Clin Oncol (R Coll Radiol) 1992; 4:141–147. [ ] 4. Ciernik IF, Dizendorf E, Baumert BG, et al. Radiation treatment planning with an integrated positron emission and computer tomography (PET/CT): a feasibility study. Int J Radiat Oncol Biol Phys 2003;57:853–863. [ ] 5. Bradley J, Thorstad WL, Mutic S, et al. Impact of FDG-PET on radiation therapy volume delineation in non-small cell lung cancer. Int J Radiat Oncol Biol Phys 2004;59:78–86. [ ] 6. Mac Manus MP, Wong K, Hicks RJ, Matthews JP, Wirth A, Ball DL. Early mortality after radical radiotherapy for non-small cell lung cancer: comparison of PET-staged and conventionally staged cohorts treated at a large tertiary referral center. Int J Radiat Oncol Biol Phys 2002;52:351–361. [ ] 7. Xing L, Wessesl B. The value of PET/CT is being over-sold as a clinical tool in radiation oncology. Point/counterpoint. Med Phys 2005;32: 1457–1459. [ ] 8. Gregoire V. Is there any future in radiotherapy planning without the use of PET: unraveling the myth... Editorial. Radiother Oncol 2004;73:261–263. [ ] 9. Paulino AC, Johnstone PA. FDG-PET in radiotherapy treatment planning: Pandora's box? Editorial. Int J Radiat Oncol Biol Phys 2004;59:4–5. [ ] 10. Allen AM, Siracuse KM, Hayman JA, Balter JM. Evaluation of the influence of breathing on the movement and modeling of lung tumors. Int J Radiat Oncol Biol Phys 2004;58:1251–1257. [ ] 11. Nestle U, Walter K, Schmidt S, et al. 18F-deoxyglucose positron emission tomography (FDG-PET) for the planning of radiotherapy in lung cancer. High impact in patients with atelectasis. Int J Radiat Oncol Biol Phys 1999;44:593–597. [ ] 12. Erdi YE, Rosenzweig, K, Erdi AK, et al. Radiotherapy treatment planning for patients with non-small cell lung cancer using positron emission tomography (PET). Radiother Oncol 2002;62: 51–60. [ ] 13. Black QC, Grills IS, Kestin LL, et al. Defining a radiotherapy target with positron emission tomography. Int J Radiat Oncol Biol Phys 2004;60: 1272–1282. [ ] 14. Mac Manus M. Role of PET-CT in the optimization of thoracic radiotherapy. Lung Cancer (Suppl 3) 2005;49:S74–75. [ ]
Received June 14, 2006. Accepted after revision September 20, 2006.
* Study developed at McGill University - Department of Radiation Oncology, Montreal, Quebec, Canada. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554