Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 3 - May / June of 2007
Vol. 40 nº 3 - May / June of 2007
|
WHICH IS YOUR DIAGNOSIS?
|
|
QUAL O SEU DIAGNÓSTICO? |
|
|
Autho(rs): Rafael Burgomeister Lourenço, Marcelo Bordalo Rodrigues |
|
|
A female, 45-year-old patient complaining of pain on the anterior aspect of the left knee for about five years. At presentation, the patient reported a history of direct local trauma eight months ago, with worsening of the pain, swelling, and restricted movement amplitude. She denied previous surgical interventions or other relevant antecedents. At clinical examination she presented swelling in the infrapatellar region, tender to palpation and incomplete flexo-extension. Imaging findings Figure 1: Calcified mass with bone matrix on the infrapatellar fat pad.
Figure 2: Heterogeneous, solid expansive formation in the Hoffa's fat pad.
Figure 3: Areas of high signal intensity in the middle of the lesion suggesting a chondroid component. Also, joint effusion and patellar tendinopathy can be observed. Free intra-articular bodies were not identified.
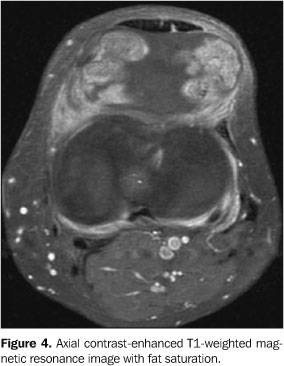
Figure 4: Lesion with heterogeneous impregnation and signs of synovitis.
Diagnosis: Chondroma of the Hoffa's fat pad as an end-stage Hoffa's disease.
COMMENTS Hoffa's disease (or infrapatellar fat pad syndrome) was first described by Albert Hoffa in 1904(1), and is characterized by the development of chronic inflammatory alterations associated with the impingement of the infrapatellar fat pad between the femorotibial and femoropatellar spaces. The process may be caused by a major acute (direct or indirect) trauma or by chronic repetitive traumas, resulting in hemorrhage and edema in the infrapatellar fat pad. The resulting swelling predisposes to impingement and impact on the infrapatellar fat pad, accentuating local inflammatory alterations, fat pad hypertrophy and further injury and inflammation. The progress of chronic inflammation results in adipocytes fibrosis and fibroblast proliferation with marked fibrosis(2). Chondroid metaplasia may eventually occur, and endochondral ossification is rare, resulting in the development of true osteochondromas just like in the present case. Primary mechanical changes, such as genu recurvatum, rotational microinstability or other conditions affecting the femorotibial and femoropatellar spaces contribute to the process and may result in primary impact, progressing to chronic entrapment with a similar appearance, in the absence of a triggering, traumatic factor, this entity being characterized as Hoffa's syndrome(3). In the literature, there are some case reports and series about patients presenting with history, symptoms, radiological and anatomopathological findings similar to those described for Hoffa's disease, and characterized as "para-articular" or "intracapsular" chondromas(4_7). Because of the similarity between these processes, some authors(8), have considered that both entities are related, and that these chondromas, in truth, are more than simple areas of osteocartilaginous change or heterotopic ossification randomly developing within the infrapatellar fat pad, as a matter of fact representing an end-stage Hoffa's disease. Main clinical symptoms are pain on the anterior aspect of the knee, and reduced movement amplitude. The typical clinical finding is hypertrophied, hardened and painful fat tissue (Hoffa's sign _ pain at knee extension with digital compression over the infrapatellar fat pad). The radiographic diagnosis is based on the direct identification of osteochondroma and only can be achieved late in time, after ossification. Likewise, scintigraphy is effective only during the active phase of the ossifying process(7). Magnetic resonance imaging allows evaluating the presence of inflammatory alterations both at acute and chronic phases of the disease. At the acute phase, edemas can be identified as areas of lowintensity signal on T1weighted images and increased signal intensity on T2-weighted images. Also, areas with extremely low signal intensity may be demonstrated in both sequences as a result of hemorrhage with hemosiderin deposition. At the chronic phase of the disease, fibrous scarring tissues may be identified as irregular areas with low signal intensity on T1- and T2-weighted images. Chondroid matrix may be identified as nodular areas with increased signal intensity on T2-weighted images. In case of endochondral ossification, areas with increased signal intensity may be identified within the lesion on T1-weighted images, representing proliferation of medullary adipocytes. Regardless the phase of the disease, occurrence of contrast impregnation is frequent as a result of local inflammatory alterations. Differential diagnosis at early phases of the disease include infrapatellar plica syndrome. When signal abnormalities follow the course of the infrapatellar plica (a line extending from the inter-condylean sulcus to the retropatellar fat tissue, parallel to the anterior cruciate ligament), most probably the diagnosis is plica syndrome. More diffuse abnormalities affecting the whole posterior aspect of the infrapatellar fat pad indicate the diagnosis of Hoffa's disease(9). Other differential diagnoses to be considered are: synovial chondromatosis, pigmented villonodular synovitis, calcinosis, osteochondrosis, calcareous tendinopathy, femur, tibia or even patella tumors with infrapatellar fat tissue invasion, and, even though extremely rare, primary chondrosarcomas of the Hoffa's fat pad. The primary therapeutic approach should be clinical. Refractory cases require surgical approach for lesion resection, both the open(4_7) and the arthroscopic(2,8,10) approaches being feasible. In most of cases, resection results in symptoms resolution, without recurrence of the lesion.
REFERENCES 1.Hoffa A. Influence of adipose tissue with regard to the pathology of the knee joint. JAMA 1904;43: 795_796. 2.Magi M, Branca A, Bucca C, Langerame V. Hoffa disease. Ital J Orthop Traumatol 1991;17:211_216. 3.Jacobson JA, Lenchik L, Ruhoy MK, Schweitzer ME, Resnick D. MR imaging of the infrapatellar fat pad of Hoffa. RadioGraphics 1997;17:675_691. 4.Mosher JF, Kettelkamp DB, Campbell CJ. Intracapsular or para-articular chondroma: a report of three cases. J Bone Joint Surg Am 1966;48:1561_1569. 5.Milgram JW, Dunn EJ. Para-articular chondromas and osteochondromas: a report of three cases. Clin Orthop Relat Res 1980;148:147_151. 6.Smillie IS. Lesions of the infrapatellar fat pad and synovial fringes: Hoffa's disease. Acta Orthop Scand 1963;33:371_377. 7.Böstman O, Karaharju E, Heikkonen L, Holmström T. Extraskeletal ossifying chondroma in the knee: a case report. Acta Orthop Scand 1985;56: 87_89. 8.Krebs VE, Parker RD. Arthroscopic resection of an extrasynovial ossifying chondroma of the infrapatellar fat pad: end-stage Hoffa's disease? Arthroscopy 1994;10:301_304. 9.Saddik D, McNally EG, Richardson M. MRI of Hoffa's fat pad. Skeletal Radiol 2004;33:433_444. 10.Ogilvie-Harris DJ, Giddens J. Hoffa's disease: arthroscopic resection of the infrapatellar fat pad. Arthroscopy 1994;10:184_187. |
|



Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554