Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 2 - Mar. / Apr. of 2007
Vol. 40 nº 2 - Mar. / Apr. of 2007
|
RADIOLOGY EDUCATION
|
|
Scanometry of lower extremities: revisiting Dr. Juan Farill |
|
|
Autho(rs): Henrique Zambenedetti Werlang, Gabriel Antônio de Oliveira, Ana Maria Tamelini, Ben Hur Madalosso, Francisco da Silva Maciel Júnior |
|
|
Keywords: Farill, Orthoradiographic measurement, Lower extremities, Difference |
|
|
Abstract:
ITitular Members of Colégio Brasileiro de Radiologia e Diagnóstico por Imagem (CBR), MDs, Residents at Centro de Diagnóstico por Imagem (CDI)/Hospital Universitário Cassiano Antônio de Moraes (HUCAM)/Hospital Infantil Nossa Senhora da Glória (HINSG), Vitória, ES, Brazil
INTRODUCTION The most accurate way to evaluate the difference in lengthbetween lower extremities is by means of imagingstudies(1). Scanography was first described byMerrill in 1942(2). In 1953, Dr. Juan Farilldescribed a practical technique for measuring differences inlength between the lower limbs(3). Theprinciple is very simple: in the measurement of the differencebetween the two distances, the elimination of equal segments fromboth distances does not change the final result. Since it is aneasy-to-perform method and does not require any specificequipment, it is routinely performed in any general Radiologyservice. However, few specialists had the opportunity to read theoriginal article of Dr. Juan Farill; they have almost alwayslearned the method with someone who also has not read it.Consequently, the measuring method is not standardized andincorrect results are obtained, affecting the patient'streatment, which varies according to the type and degree ofdeformity observed(4). This method, likewiseothers is limited, and is contraindicated in some cases. The objective of the present study is to restore and divulgethe measurement technique recommended by the author, as well asto compare its efficiency with the other methods available(scanography with millimetric ruler, panoramic radiography andcomputed tomography).
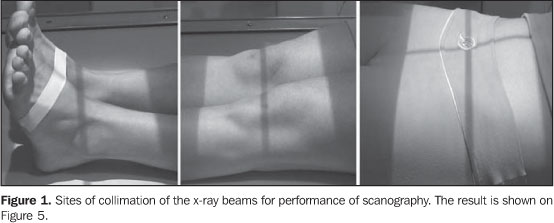
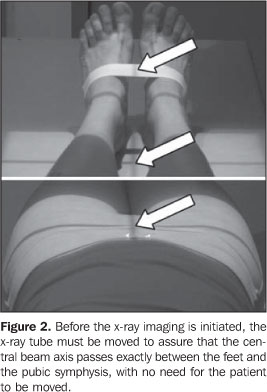
SCANOGRAPHY (TECHNIQUE) The examination is performed in two stages. In the first one, with the patient lying in supine position on a Potter-Bucky table, his/her feet are placed together with their longest axes forming an angle of approximately 90º with the table (Figure 1); the longitudinal, central axis of the collimator is aligned in a way that it passes exactly between the ankles and the pubic symphysis of the individual (Figure 2). The patient must remain still until the examination is completed. With two lead plates, the film is divided into three segments, which are separately radiographed: in the first one, the hip x-ray is performed; in the second one, the knees; in the third one, the ankles. The numbering device at the patient's right, indicates the side. Between images acquisitions, only x-ray-drawers can be moved. In no hypothesis should the chassis be removed from the drawer until the three exposures are completed.
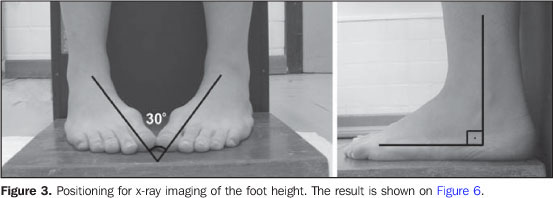
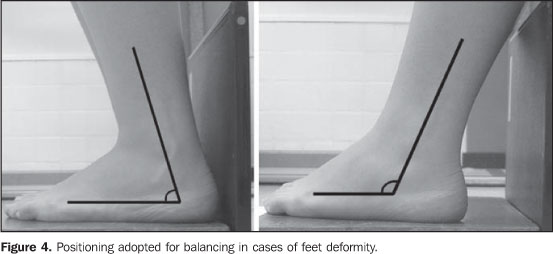
In a second stage, the study proceeds to measure the feet height. With the feet internally rotated about 30º on a wood platform whose posterior surface is covered with lead, the chassis is positioned immediately behind the feet, and an anteroposterior x-ray view from the ankles is made. This positioning determines a dissociation of malleolus, allowing a total visualization of the tali. For an adequate imaging the foot soles must be totally resting on the platform (Figure 3). In case this is not possible because of any deformity, for example, towards or backwards inclination should be tried, as necessary, until an appropriate positioning is achieved (Figure 4).
This second stage usually is neglected because of unawarenessor because most of times there are no significant differencesbetween feet height. However, there are situations where this mayhappen (congenital lesions, poliomyelitis sequelae,osteocartilaginous destruction by inflammatory or surgicalprocesses, etc.). Contraindications of the method The most important aspect is the impossibility of a completecontact of all the surfaces of the lower limb with the tablesurface, because flexed positions distort bone images on x-rayfilms. This occurs when external fixators areutilized(5), in femur and tibia deformities onsagittal plane or contractures with flexion of hip or knee. Pronounced valgus, varus or equinus deformities hinder areliable evaluation of the differences between foot heights.
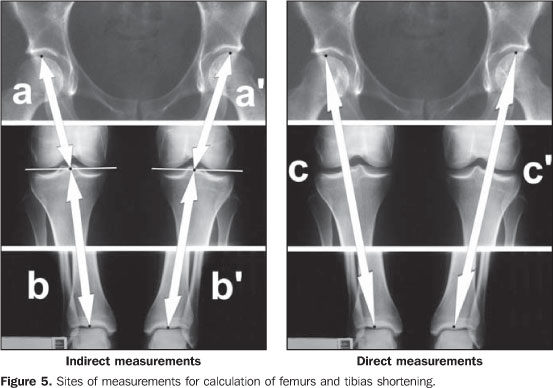
SCANOMETRY (MEASUREMENTS) The first measurement is performed in the scanography, between the highest point on the femoral head and the projection of the center of the intercondylar notch on a line touching the femoral condyles (Figure 5a). The same procedure is performed in the contralateral limb (Figure 5a'); the difference between these two measurements representing the femoral shortening.
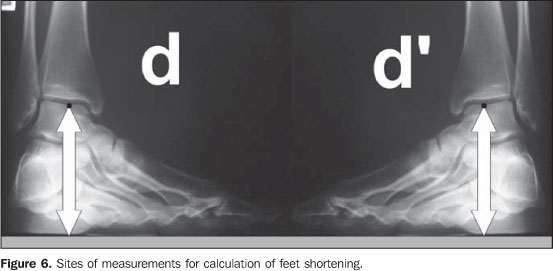
The second measurement is the distance from the same point on the line between the femoral condyles up to the lowest point on the tibial articular surface, in the ankle (Figure 5b). This measurement is repeated for the contralateral bone (Figure 5b'); the difference between these two measurements represents the tibial shortening. The third measurement is performed directly from the highest point on the femoral head up to the lowest point on the tibial articular surface (Figure 5c). This procedure is repeated for the contralateral limb (Figure 5c'); the difference between these two measurements was named functional shortening by Farill. Finally, the fourth measurement concerns the foot height; it is performed from the lowest point of the talus, on the tibiotarsal joint surface, up to the line resulting from the lead plate on the posterior surface of the wood platform (Figure 6d); this measurement is repeated for the contralateral foot (Figure 6d'). The difference between these two measurements corresponds to the foot shortening.
Calculation and discrepancies analysis Lower limbs length discrepancy may basically be due to threetypes of alterations: The first one is bones with differentlengths in relation to their contralateral; the second, is apatient with varus deviation or valgus asymmetry, that is, when alimb presents a greater curvature than its contralateral; thethird one is isometric femurs and tibias and discrepant footheights. Overlapping of such alterations is frequently found, sothese measurements should be evaluated as whole. Initially, the right functional measurement must be added tothe right foot height. This calculation is repeated for the leftside. Then, one measurement is subtracted from the other, so thefunctional discrepancy between the lower limbs is found. This isthe discrepancy that must be mentioned in the medical report, theindirect measurements being utilized only for analyzing thedeformity. So, once the discrepancy between lower limbs is found, we must perform a comparative analysis of the indirect (Figures 5a + 5b; Figures 5a' + 5b') and direct measurements (Figure 5c; Figure 5c'). The results will be: – The lower limbs length discrepancy is the same both fordirect and indirect measurements. This means that the shorteningis real, i.e., femurs and/or tibias present different lengths(example 1); – Indirect measurements indicate limb length equality, anddirect measurements indicate limb length discrepancy. Thisindicates that the shortening is probably due to a varus orasymmetrical valgus deformity (example 2); – Both the direct and indirect measurements indicate adiscrepancy between lower limbs. In this case, there is summationof these deformities (actual shortening + varus/valgusdeformity)(example 3). Although the indirect measurement is aimed only at definingwhether the limbs shortening is real or is due to a varus/valgusdeviation, this analysis should be always performed, since it mayaffect directly the therapy of the patient. As regards the feet, the evaluation of the discrepancy between heights provides essential information. Some times femurs and tibias may present lengths equality and a discrepancy between foot heights; if this discrepancy is significant and we fail to perform this part of the examination, we are likely to fail in diagnosing an asymmetry in the total lower limbs length. On the other hand, a discrepancy between femurs and/or tibias could be balanced by an opposite asymmetry in foot heights; in this case, a treatment for the functional measurements discrepancy would be contraindicated (example 4). The Farill technique does not take into consideration the highest point from the iliac crest to the acetabulum – Figure 7). However, this measurement might to be performed with the same objective of the foot height measurement(6).
In the cases where there are knees dysplasias, and a linecannot be drawn between femoral condyles, Farill recommends thatonly direct measurements are utilized in conjunction with thefoot height measurements. In cases of hip or ankle dysplasias, the author does notmention alternatives; for these cases, we suggest the methodemployed by Terry et al.(7), where themeasurement is performed directly from the anterior superioriliac spine to the outermost point of the lateral malleolus. Forthis purpose a film with only two exposures is necessary, witheach exposure including the anatomical points of reference(anterosuperior iliac spine and lateral malleolus). Even so, itis our understanding that the foot height as well as the iliacwings measurements should be performed and included in thediscrepancies calculation. In our opinion, the Bell-Thompson method (with a millimetricruler), although being recommended by someauthors(8,9), does not offer any substantiveadvantages over the Farill technique. As the ruler remainspositioned on the chassis, it does not follow the magnificationof the long bones in the radiographic imaging, which could resultin measurement errors(10). Additionally, fordemanding a strict immobilization of the patient, it is verydifficult to employ this method inchildren(8). The panoramic x-ray of lower limbs is a very accurate methodand presents as an advantage the possibility of being performedin orthostasis(10). However, it presents theinconvenience of not being widely available, besides the highcost. Also, it does not measure appropriately feet and iliacwings heights, and must be complemented by x-rays appropriate forsuch measurements. The measurement of lower limbs discrepancy by means of CTtopogram is mentioned by some authors as the most accurate methodfor diagnosis of lower limbs asymmetry(5,11).This is true, mainly in the cases where a complete resting of thefoot soles on the platform is not achieved (deformities,utilization of external fixators, etc.); in these cases, it isnecessary to perform a lateral topogram with the measurements onthis view(5). Additionally, amongst the methodsanalyzed in the present study, this is the method with lowestradiation dose(5,10,11), and is the method ofchoice for young patients who need serial studies during thetherapy management. But, besides not being widely available,presents high cost(10). In summary, considering the low cost, high availability andreasonable accuracy, we recommend the Farill technique,complemented with an iliac wing measurement. In cases where thereis a contraindication, we recommend a panoramic x-ray or computedtomography.
REFERENCES 1. Lampe HI, Swierstra BA, Diepstraten AF. Measurement of limb length inequality. Comparison of clinical methods with orthoradiography in 190 children. Acta Orthop Scand 1996;67:242–244. [ ] 2. Merrill OE. A method for roentgen measurement of the long bones. Am J Roentgenol Radium Ther Nucl Med 1942;48:405–406. [ ] 3. Farill J. Orthoradiographic measurement of shortening of the lower extremity; technic. Med Radiogr Photogr 1953;29:32–38. [ ] 4. Dahl MT. Limb length discrepancy. Pediatr Clin North Am 1996;43:849–865. [ ] 5. Aaron A, Weinstein D, Thickman D, Eilert R. Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992; 74:897–902. [ ] 6. Badii M, Shin S, Torreggiani WC, et al. Pelvic bone asymmetry in 323 study participants receiving abdominal CT scans. Spine 2003;28:1335–1339. [ ] 7. Terry MA, Winell JJ, Green DW, et al. Measurement variance in limb length discrepancy: clinical and radiographic assessment of interobserver and intraobserver variability. J Pediatr Orthop 2005;25:197–201. [ ] 8. Lebouchard R, Denis JP, Trope J, Duranteau Mme. Mensuration radiologique osseuse par la méthode de Bell Thompson. J Radiol Electrol Arch Electr Medicale 1956;37:108–110. [ ] 9. Delouvrier JJ, Nahum H. Longueur des membres. Précision des méthodes orthoradiographiques. J Radiol 1981;62:647–651. [ ] 10. Machen MS, Stevens PM. Should full-length standing anteroposterior radiographs replace the scanogram for measurement of limb length discrepancy? J Pediatr Orthop B 2005;14:30–37. [ ] 11. Aitken AG, Flodmark O, Newman DE, Kilcoyne RF, Shuman WP, Mack LA. Leg length determination by CT digital radiography. AJR Am J Roentgenol 1985;144:613–615. [ ]
Received September 22, 2005.
* Study developed at Centro de Diagnóstico por Imagem (CDI) and at Hospital Infantil Nossa Senhora da Glória (HINSG), Vitória, ES, Brazil. |
|


Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554